Fortnightly Review: Bone densitometry in clinical practice
BMJ 1995; 310 doi: https://doi.org/10.1136/bmj.310.6993.1507 (Published 10 June 1995) Cite this as: BMJ 1995;310:1507
- J E Compston, honorary consultant physiciana,
- C Cooper, reader in rheumatologyb,
- J A Kanis, professor of human metabolism and clinical biochemistryc
- a Department of Medicine, University of Cambridge Clinical School, Addenbrooke's Hospital, Cambridge CB2 2QQ
- b Medical Research Council Environmental Epidemiology Unit, Southampton General Hospital, Southampton SO16 6YD
- c Department of Human Metabolism and Clinical Biochemistry, University of Sheffield Medical School, Sheffield
- Correspondence to: Dr Compston.
- Accepted 30 January 1995
Abstract
Summary points
Osteoporosis is a major health problem in the elderly population. It causes more than 150000 fractures each year in the United Kingdom with an estimated cost of pounds sterling742 million
Bone mass is a major determinant of risk of fracture and can be assessed by non-invasive techniques such as dual energy x ray absorptiometry
Densitometric criteria based on standard deviation scores expressed in relation to reference values in premenopausal women (T scores) provide diagnostic categories from which thresholds for prevention and treatment can be defined on the basis of risk of fracture
Population based screening for low bone mass in perimenopausal women cannot at present be justified. In clinical practice, however, bone densitometry has an important role in the diagnosis of osteoporosis in high risk groups and in the monitoring of treatment in some patients
For these indications, it is estimated that about 175 bone scans per 100000 population would be needed annually, requiring an annual expenditure for the average health district of pounds sterling25200
At present, bone densitometry resources in the United Kingdom are inadequate to meet these needs. There is an urgent need to improve existing facilities so that effective strategies for the prevention and treatment of osteoporosis in clinical practice can be implemented
Osteoporosis is characterised by low bone mass and disruption of bone architecture resulting in reduced bone strength and increased risk of fracture.1 The fractures which arise are widely recognised as a major health problem in the developed world, causing considerable morbidity and mortality in the elderly population and imposing an enormous financial burden on the health services. The remaining lifetime risk of osteoporotic fracture in 50 year old British white women has been estimated at 14% for the hip, 11% for the spine, and 13% for the radius.2 3 The corresponding figures in North American women are slightly higher: 17.5%, 15.6%, and 16%, respectively. The remaining risk for any fragility fracture approaches 40% in women and 13% in men.4 For women this risk is as great as that of cardiovascular disease and six times higher than that of breast cancer. In the United Kingdom it is estimated that about 60000 fractures of the hip and 50000 fractures of the radius occur annually. The number of clinically diagnosed vertebral fractures is around 40000,5 but this represents only a proportion of the total number as many vertebral fractures, possibly as many as two thirds, do not come to medical attention. The total annual cost of osteoporotic fractures in England and Wales is estimated at pounds sterling742 million, most of which is attributable to the direct hospital costs of hip fractures.6 This paper reviews methods which now exist for the diagnosis of osteoporosis, their use in clinical practice, and likely service implications in the United Kingdom.
Bone mass and risk of fracture
After the attainment of peak bone mass, bone loss in women begins at or shortly before the menopause in the spine and possibly as early as the mid-30s in the femoral neck. Bone mass is a major determinant of bone strength, and prospective studies have shown an increasing gradient of risk of fracture with decreasing bone density, a decrease in the latter of 1SD being associated with a 1.5-fold to 3.0-fold increase in risk of fracture.7 8 9 10 The strength of this relation is similar to that between blood pressure and stroke and is equivalent to an eightfold to 12-fold difference in risk of fracture across the four quartiles of the distribution of bone density. Though measurement of bone mass at any of the skeletal sites commonly assessed is of value in defining risk of fracture, there is evidence that measurement of the site of potential fracture may provide the best prediction, at least in the case of fracture of the hip.10 11 12 Many of these studies have been conducted in women in the seventh and eighth decades of life, and more data are required to confirm the relation between perimenopausal bone mass and subsequent risk of fracture.
Measurement of bone mass
Several techniques are available for the assessment of bone mass.6 Dual energy x ray absorptiometry is widely used because of its ability to assess bone mass at both axial and appendicular sites, its high reproducibility, and the very low doses of radiation associated with measurement (less than the daily natural background levels).13 Single energy photon and x ray absorptiometry enable measurements only at appendicular sites, usually the forearm; the machines are portable and relatively inexpensive and, like dual energy x ray absorptiometry, have high reproducibility and require very low doses of radiation. Quantitative computed tomography enables differential measurement of cortical and cancellous bone in the spine or peripheral skeleton, but the equipment required is expensive and the radiation dose relatively high. Finally, broadband ultrasonic velocity and attenuation of the os calcis, tibia, or patella is currently being evaluated. It is radiation free and, like single energy photon and x ray absorptiometry, the machines are portable and relatively cheap.
Bone mass and fracture risk
Bone mass is a major determinant of risk of fracture
A reduction in bone density of 1SD is associated with a 1.5-3.0-fold rise in risk
Several techniques are now available for assessment of bone mass; these include single and dual photon absorptiometry, dual energy x ray absorptiometry, quantitative computed tomography, and broadband ultrasound attenuation
The optimal site for assessment of bone density for prediction of risk of fracture has not been established, although there is some evidence that measurements in the femoral neck provide the best prediction for hip fracture
With the exception of quantitative computed tomography, which measures a volumetric bone density in g/cm3, these techniques generate a linear measurement of bone mineral content (g or g/cm) which can be converted into an areal bone density (g/cm2) by dividing the bone mineral content by the width of the bone in the forearm or the area of the scan in the spine and hip. Thus bone mineral content and to a less extent bone mineral density reflect bone size as well as true bone density; the influence of size can be reduced by the use of various correction factors, but this may reduce the predictive value of the measurement as bone size is probably an important and independent determinant of risk of fracture.
Some limitations of absorptiometric techniques should be recognised. Firstly, the absolute bone mineral density for a given bone mass varies with different systems,14 and there are also differences in the reference data provided by the manufacturers,15 so that the same measured value may lie within different parts of the reference range depending on the system used. Secondly, measurement of bone mineral density in the spine may be affected by the presence of extraskeletal calcification, osteophytes, scoliosis, and vertebral deformity, particularly in elderly subjects.16 Thirdly, the distribution of osteoporosis within the spine may be heterogeneous, with differential involvement of the dorsal spine17; lateral radiographs of the dorsal spine should therefore be performed in addition to bone densitometry in patients who complain of loss of height or pain in the dorsal spine or who have evidence of dorsal kyphosis. Finally, osteomalacia also results in low bone mineral density measured by absorptiometric techniques and should be excluded in patients at increased risk of vitamin D deficiency and osteomalacia.
Densitometric criteria for the diagnosis of osteopenia and osteoporosis
Bone density values are usually expressed in relation to reference data as standard deviation scores: a Z score representing the number of standard deviations above or below the age and sex matched mean reference value and a T score similarly expressed in relation to reference values for young adults. These standard deviation units reduce the problems associated with differences in calibration between instruments; if Z scores were used to define osteoporosis, however, the prevalence of this disorder would not increase with age, whereas it is established that risk of fracture increases and bone density decreases with age. Cut off values expressed as T scores partially take these age related changes into account, and their use is thus preferred in the definition of osteopenia or osteoporosis,18 19 although they do not capture the adverse effects of aging itself on risk of fracture.8 20
As the gradient of risk of fracture across bone density values is continuous it is not possible to define an absolute cut off point of bone density below which fractures will occur and above which they will not. None the less, for diagnostic purposes a bone density can be selected at which intervention is recommended. Two thresholds have been proposed19: one which includes most of those women who will sustain a fracture in the future (osteoporosis), and a higher threshold which has lower specificity but is regarded as an appropriate criterion for prophylaxis in perimenopausal women (osteopenia). According to this classification, osteoporosis is defined as a T score below -2.5 and osteopenia as a T score between -1 and -2.5. Established osteoporosis denotes a T score below -2.5 in the presence of one or more fragility fractures. Osteoporosis and established osteoporosis may be regarded as indications for intervention in most cases; the prevalence of osteoporosis in women aged 50-54 years (based on United Kingdom reference data obtained on Hologic DXA systems) is approximately 3.5% and 2.0% in the spine and femoral neck, respectively; the corresponding figures in women aged 70-74 years are 15% and 20%. The prevalence of osteopenia in women at the menopause is around 15%, rising to over 90% by the age of 80 years. Indications for prophylactic measures in women with osteopenia will be influenced by several factors, including age and the risks and benefits of the proposed treatment. These thresholds apply only to women; appropriate criteria for men, in whom areal bone density values are higher, require further research.
Densitometric criteria for the diagnosis of osteoporosis
Diagnostic classification of osteoporosis is based on densitometric criteria, bone density values being expressed in relation to the mean reference value in premenopausal women (T score)
Osteopenia is defined as a T score between -1 and -2.5 and may constitute an indication for prophylaxis depending on the age of the woman and the risks and benefits of the proposed treatment
Osteoporosis is defined as a T score below -2.5 and includes nearly all women who will sustain a fragility fracture. It can be regarded as an absolute indication for intervention
Clinical indications for bone densitometry
The severity of bone loss and structural disruption of cancellous bone in established osteoporosis with fracture argue strongly for the more frequent use of bone densitometry early in the clinical course of the disease, particularly as most interventions act predominantly by reducing bone loss rather than increasing bone mass. Preventive strategies may be targeted at everyone in the population (for example, modifications in diet or physical activity) or at high risk subgroups. In recent years there has been much discussion about the potential use of population based screening, using measurement of bone density to indicate risk of fracture, as part of such a high risk strategy.21 22 Although such an approach has its advocates, the case for screening of women at the menopause is not strong.23 The consensus view that population based screening cannot at present be justified should not, however, be confused with the role of bone densitometry in the diagnosis and management of osteoporosis. In particular, it is important to recognise the conceptual difference between screening, which involves a case finding approach among people who have not sought medical advice, and clinical practice, in which patients seek such advice.
In the absence of population based screening, selection of patients for bone densitometry on the basis of strong clinical risk factors provides the most logical approach to the prevention and treatment of osteoporosis.6 24 In this context assessment of bone mass is justified only in those cases in which the result obtained will influence decisions about treatment. For example, in women with a premature menopause, hormone replacement is prescribed routinely without assessment of bone mass unless strong contraindications exist. If treatment is refused for any reason, assessment of bone mass may nevertheless be useful in reaching a decision about other interventions. For most of the clinical indications listed in the box, however, bone densitometry is preferred to “blind” treatment as not all patients will have low bone mass.
Many risk factors have been identified for osteoporosis.25 The relatively poor specificity and sensitivity of risk factor scores in predicting either bone density or risk of fracture26 27 partly reflect the varying strength and prevalence of the risk factors used. Thus common but relatively weak risk factors, such as cigarette smoking, physical inactivity, high caffeine consumption, and a family history of osteoporosis, will have a greater influence on risk factor scores in the general population than stronger risk factors, such as premature menopause and treatment with cortiscosteroids, which are more important in individual patients. Prevalent fractures are particularly strong risk factors for subsequent fractures of the spine, an effect which is to some extent independent of bone mass.28 29
Diagnostic uses of bone densitometry can be divided into two general categories. Firstly, measurement of bone mass is indicated in patients who have strong risk factors to assess risk of fracture and select for treatment. In those patients with bone density above the treatment threshold, the measurement may be repeated at intervals of two to three years unless the underlying cause has been successfully treated. Secondly, bone densitometry should be used to confirm or refute the diagnosis of osteoporosis in patients with radiological evidence of osteopenia or vertebral deformity, or both, and those with a history of fragility fracture at the wrist, hip, or spine. In patients with multiple vertebral deformities, however, bone densitometry is not usually required for diagnostic purposes.
Clinical indications for bone densitometry
Presence of strong risk factors:
Premature menopause (<45 years)
Prolonged secondary amenorrhoea
Primary hypogonadism
Corticosteroid therapy (>7.5 mg/day for one year or more)
Anorexia nervosa
Malabsorption
Primary hyperparathyroidism
Organ transplantation
Chronic renal failure
Myelomatosis
Hyperthyroidism
Prolonged immobilisation
Radiological evidence of osteopenia or vertebral deformity, or both
Previous fragility fracture of the hip, spine, or wrist
Monitoring of therapy:
Hormone replacement therapy in patients with secondary osteoporosis
Newer drugs—for example, bisphosphonates, calcitonin, vitamin D metabolites, sodium fluoride
Clinical indications for bone densitometry
Population based screening of perimenopausal women for low bone mass cannot at present be justified
In clinical practice, selection of patients for bone densitometry should be made on the basis of strong clinical or historical risk factors if the result obtained will influence management of the disease
Measurement of bone mass is indicated in the monitoring of treatment in some patients
Measurement of bone mass may also be used to monitor treatment. In healthy perimenopausal or postmenopausal women taking bone-sparing doses of hormone replacement therapy, repeated assessment of bone density is not routinely indicated, but in the presence of complicating factors, for example malabsorption or treatment with corticosteroids, monitoring is justified. In those receiving treatments other than hormone replacement—for example, bisphosphonates, calcitonin, vitamin D metabolites, and sodium fluoride—bone density should also be monitored as the effects of these drugs on bone mass are less well documented, and differential effects on cortical and cancellous bone mass and site specific changes may occur.
The ability of repeated measurements of bone density to detect change depends on the precision of the measurement. Dual energy x ray absorptiometry has a precision error of about 1% at the spine and 2-3% at the femoral neck and greater trochanter; low bone density and the presence of osteophytes and extraskeletal calcification, however, reduce reproducibility. Forearm measurements by single energy photon and x ray absorptiometry have a reproducibility error of 0.5-1.0%. In individual patients, the demonstration of a relevant change requires an increase or decrease of two to three times the coefficient of variation. In the spine and forearm the annual bone losses in postmenopausal women are somewhat greater then the precision of the measurement, and effects of treatment can usually be detected within two years; in the femur, however, where rates of bone loss are slower and precision poorer, three or more years may be required.
Implications for health service provision
The service demands for bone densitometry estimated on the basis of these clinical indications are relatively modest. In an average health district of 300000 people with the age and sex structure of the United Kingdom population in 1990, facilities would be required to scan 125 women each year with a premature menopause or other strong risk factors who, after counselling, predicate their decision regarding use of oestrogen on the result of bone density; 200 men and women with vertebral deformities or radiographic osteopenia coming to clinical attention; 40 men and women with established secondary osteoporosis; and 160 patients in whom monitoring of treatment is required.
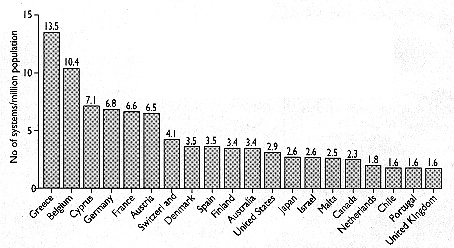
Geographic distribution of dual energy x ray absorptiometry systems. Vertical axis shows number of systems available for each million of population
{kind=link}
This annual allocation of scans of 175 per 100000 population is similar to the current rates of use of 180 per 100000 reported from existing osteoporosis units in the United Kingdom (D Reid, personal communication). Costs will vary according to through-put and capital outlay; at a relative cost of pounds sterling48 for scans of the lumbar spine and femoral neck, however, which is representative of costs in most bone density units currently operating, provision of such a service for a population of 300000 would require an annual expenditure of pounds sterling25200.
The availability of adequate facilities and equipment in the United Kingdom is patchy, with about 90 instruments currently installed, of which 31% have been purchased by charities and 12% by health authorities. Their purchase has largely been driven by local clinicians who have set out to develop a hospital based osteoporosis service. As the figure shows, the United Kingdom compares poorly with other European countries, North America, and Japan with regard to availability of bone densitometry systems. Provision of adequate access to specialist skill will require a finite, albeit relatively modest, allocation of new resources to areas which at present are lacking the required facilities.
Implications for health service provision
Annual service demands for bone densitometry can be estimated at about 175 scans per 100000 population, based on the defined clinical indications
At a relative cost of pounds sterling48 per scan the annual expenditure for each health district would be around pounds sterling25200
Availability of bone densitometry facilities in the United Kingdom is patchy, with inadequate access for many general practitioners and hospital doctors.
New resources are urgently required to meet existing demands
Conclusions
Bone densitometry represents a major advance in the clinical management of osteoporosis. Bone mass provides the best prediction of fracture risk, and its assessment in those at risk from osteoporosis enables preventive measures to be instituted before fracture occurs. A recent statement from Dr Kenneth Calman, the chief medical officer, has endorsed this view, emphasising the value of assessment of bone density in clinical practice and the need for provision of appropriate resources throughout the United Kingdom (fourth Bath conference on osteoporosis and bone mineral measurement, 1994). Improved access to this service, which should be provided only by professionals with skill in both the performance and interpretation of bone densitometry, is an essential component of future strategies for preventing and treating osteoporosis.