Article Text

Abstract
Objective To examine the impact of the ban on smoking in enclosed public places implemented in England in July 2007 on children's exposure to secondhand tobacco smoke.
Design Repeated cross-sectional surveys of the general population in England.
Setting The Health Survey for England.
Participants Confirmed non-smoking children aged 4–15 with measured saliva cotinine participating in surveys from 1998 to 2008, a total of 10 825 children across years.
Main outcome measures The proportion of children living in homes reported to be smoke-free; the proportion of children with undetectable concentrations of cotinine; geometric mean cotinine as an objective indicator of overall exposure.
Results Significantly more children with smoking parents lived in smoke-free homes in 2008 (48.1%, 95% CI 43.0% to 53.1%) than in either 2006 (35.5%, 95% CI 29.7% to 41.7%) or the first 6 months of 2007, immediately before the ban came into effect (30.5%, 95% CI 19.7% to 43.9%). A total of 41.1% (95% CI 38.9% to 43.4%) of children had undetectable cotinine in 2008, up from 34.0% (95% CI 30.8% to 37.3%) in 2006. Geometric mean cotinine in all children combined was 0.21 ng/ml (95% CI 0.20 to 0.23) in 2008, slightly lower than in 2006, 0.24 ng/ml (95% CI 0.21 to 0.26).
Conclusions Predictions that the 2007 legislative ban on smoking in enclosed public places would adversely affect children's exposure to tobacco smoke were not confirmed. While overall exposure in children has not been greatly affected by the ban, the trend towards the adoption of smoke-free homes by parents who themselves smoke has received fresh impetus.
- Cotinine
- environmental tobacco smoke
- public policy
- surveillance and monitoring
Statistics from Altmetric.com
Introduction
Legislation banning smoking in enclosed public places in England came into effect in July 2007. The ban would be expected to have a direct impact on adult exposures through reductions in secondhand smoke in workplaces, pubs, bars and other places of entertainment. Reduced adult exposures have indeed been observed (Sims M, Mindell J, Jarvis M, et al. Did smokefree legislation in England reduce exposure to secondhand smoke among non-smoking adults?: an analysis of the Health Survey for England. submitted) as in other jurisdictions,1 2 along with declines in hospital admissions for myocardial infarction.3 Potential impacts on children are harder to gauge. Children's exposure to other people's smoke takes place largely in the home, and is overwhelmingly determined by parental smoking.4 Any effects on children are therefore likely to be mainly indirect and mediated by changes in parental smoking. During the debates preceding the introduction of legislation it was suggested that a ban could have adverse consequences on children by displacing smoking back into the home. In 2005, giving evidence to the Health Committee of parliament and justifying his preference for a partial ban, the then Secretary of State for Health, Dr John Reid, said: “There will be a displacement if you allowed no smoking in any public place whatsoever. In our case we have got 90% of pubs and restaurants which will be non-smoking, but there will be some areas. So if you allow none whatsoever there will be a displacement”.5 6 One study of US data has concluded that smoke-free ordinances there have perversely increased children's exposure.7 In Scotland there were reductions in child exposure following introduction of a ban, but the decline only reached statistical significance in children from homes where neither parent smoked.8
Over the decade or so leading up to the ban there was a substantial decline in children's exposure to tobacco smoke in England.4 9 10 This was due in part to declines in smoking prevalence in young adults, but also to the increased adoption of smoke-free policies in homes with smoking parents.11 We use data from the Health Survey for England (HSE) to examine the impact of the 2007 ban on children's exposure. Specifically, we aim to test whether the ban led to fewer smoke-free homes where parents were smokers and whether there was an overall adverse effect on children's exposure.
Methods
The HSE is an annual survey designed to provide samples representative of households in England in terms of age, gender, geographical location and socioeconomic circumstances. The HSE uses a clustered, stratified multistage sample design. In some years a core sample from the general population is supplemented with a boost sample of respondents from particular population groups. Full details of the HSE methodology are available in published reports12 and online (http://www.ic.nhs.uk/statistics-and-data-collections/health-and-lifestyles-related-surveys/health-survey-for-england). All adults and up to two children in participating households are interviewed in the home, followed by a nurse visit to take biological measures (including saliva samples for cotinine) about 1 week later. In 2007 and 2008 66% and 64%, respectively, of eligible households participated, with 95% and 93% of children in cooperating households being interviewed, 68% and 66% seeing the nurse, and 59% and 57% giving saliva.12 13 These response rates were significantly lower than in 1998, when 74% of eligible households participated, with 96% of children in cooperating households being interviewed, 83% seeing the nurse and 81% giving saliva.14
Parental smoking was ascertained at the initial interview, smokers being identified by a positive response to the screening question “Do you smoke cigarettes at all nowadays?” Children aged 8 and above were asked about smoking through a six-level smoking experience scale incorporated into a self-completion booklet to encourage more accurate self-report. There was no attempt to assess active smoking in children aged under 8.
Information about smoking in the home was gathered for the whole household from a single adult respondent at the initial interview. The household reference person or their partner was asked “Does anyone smoke inside this house/flat on most days?” As previously,11 we define as smoke-free those homes where the response to this question was ‘no’, although it is in principle possible that such homes could be mostly rather than completely smoke-free.
Cotinine
Cotinine is a sensitive and specific quantitative indicator of the extent of uptake of nicotine over the past few days and is accepted as the best available biomarker of exposure to secondhand smoke.15 Specimens for cotinine were collected from children aged under 8 using a straw to dribble saliva through into a sample tube. Older children, like adults, were asked in earlier surveys to keep a dental roll in their mouths until it was saturated and then replace it in the sample tube but since 2007 have collected saliva directly into the tube or using salivettes.
For all years up to and including 2007 an assay using liquid extraction and gas chromatography with nitrogen phosphorus detection (the technique known as GC-NPD) was employed.16
Part way through 2008, a new method was introduced using high performance liquid chromatography coupled to tandem mass spectrometry with multiple reaction monitoring (LC-MS/MS).17 To ensure that the LC-MS/MS technique provided results which were comparable with the GC-NPD method, the two techniques were cross-validated. This showed the results from the two methods to be interchangeable. Regular quality controls were run to ensure reliability.12 The limit of detection was 0.1 ng/ml.
Sample
We combined all available data on non-smoking children from 1998 to 2008 inclusive. We excluded data from 1999 to 2004 when only ethnic minorities had a nurse visit, and from 2000, when cotinine specimens were not collected. We defined non-smoking children as those who reported no current smoking and whose cotinine levels were below a cut-point of 12 ng/ml for active smoking.18 Children aged under 8 were not asked their smoking status and were assumed to be non-smokers unless their cotinine levels were above 12 ng/ml.
Statistical analysis
Data were analysed using the Complex Samples procedures in SPSS 18 to adjust appropriately for the complex survey design involving clustering and stratification. We used supplied weights to compensate for any potential non-response to the nurse visit. These weights are available for the 2003 and later surveys. In the 2007 survey, an additional weight was introduced to further adjust for non-participation in the saliva sample and we used this weight when it became available.
Since the distribution of cotinine concentrations in non-smokers is positively skewed, we subjected the data to logarithmic transformation, first assigning a value of 0.05, half the limit of detection, to undetectable concentrations. We used three main outcome measures: the proportion of homes that were smoke-free; the proportion of children with undetectable cotinine concentrations (ie, below the limit of detection of the assay); and geometric mean cotinine concentrations as a quantitative measure of exposure to secondhand tobacco smoke. We compared values in the second half of 2007 and in 2008, after the ban had come into force, with those observed in January–June 2007 and earlier years.
Results
Table 1 shows the numbers of confirmed non-smoking children sampled in each year, and the percentages with smoking or non-smoking parents. There was a significant decline in the percentage of children with smoking parents across years, from 39% in 1998 to 33% in 2008 (p<0.001), but there was no significant change between 2006 and 2008 over the period when the ban came into effect.
Number of confirmed non-smoking children aged 4–15 each year, and parental smoking habits
The percentage of homes that were smoke-free when parents were non-smokers was over 95% and showed little change across years. However, there was a marked trend towards increasing adoption of smoke-free homes in households where parents were smokers: from 16% in 1998 to 48% in 2008 (table 2; figure 1). This trend continued without interruption through the period of implementation of the ban. Significantly more homes with smoking parents were smoke-free in 2008 than in either 2006 or the first 6 months of 2007, immediately before the ban came into effect (p<0.001). Overall, the percentage of smoke-free homes increased from 64% in 1998 to 80% in 2008.
Percentage of homes reported as smoke- free by parental smoking habits

Percentage of non-smoking children living in a smoke-free home.
Table 3 shows the percentage of children with undetectable cotinine. This was influenced both by whether parents were smokers and whether the home was smoke-free. Fewer than 5% of children had undetectable cotinine when parents were smokers and there was smoking in the home, but an increasing percentage of children of non-smoking parents living in smoke-free homes had undetectable cotinine, rising from 22% in 1998 to 59% in 2008. Among all children combined a similar trend was observed, and the percentage with undetectable cotinine in 2008 (41%) was significantly higher than in 2006 (34%, p<0.001), but no different from 2007.
Percentage of confirmed non-smoking children with undetectable cotinine by parental smoking and whether or not home is smoke-free
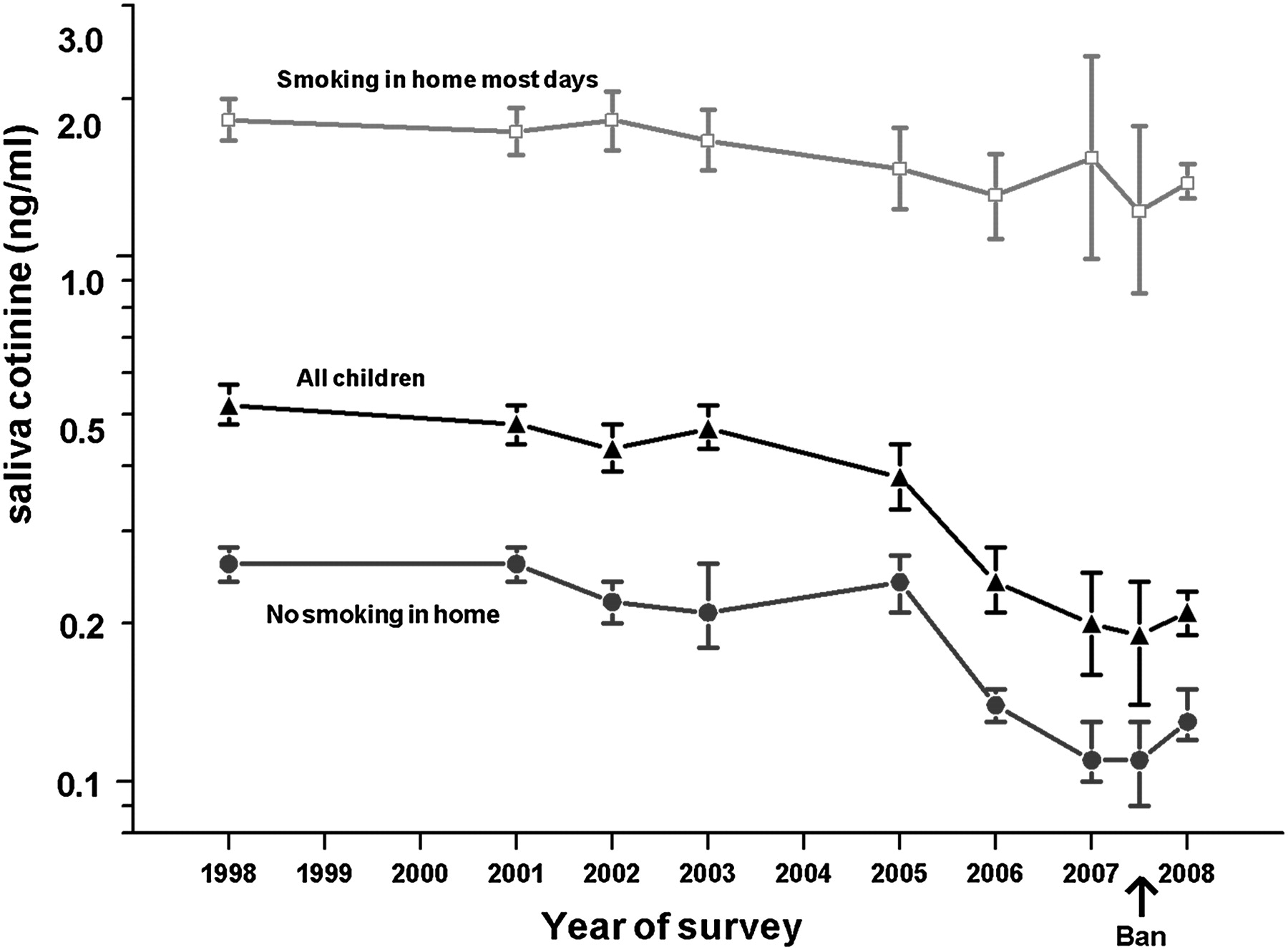
As with undetectable cotinine, geometric mean cotinine in children was strongly influenced both by parents' smoking status and by whether the home was smoke-free (table 4; figure 2). Cotinine concentrations in children with smoking parents but whose home was reported to be smoke-free were significantly higher than in children with non-smoking parents (0.35 ng/ml vs 0.11 ng/ml in 2008), but significantly lower than where parents smoked and there was smoking in the home (1.58 ng/ml in 2008), confirming the validity of the household's reported smoke-free status. Among all children combined geometric mean cotinine was on a declining trend across years, going from 0.52 ng/ml in 1998 to 0.21 ng/ml in 2008. The most marked decline occurred between 2005 and 2006 (from 0.38 ng/ml to 0 0.24 ng/ml, and there was only a modest further decline in 2008 (0.21 ng/ml).
Geometric mean cotinine in confirmed non-smoking children by parental smoking and whether or not home is smoke-free. Non-smoking children aged 4–15
{kind=link}
{kind=link}
Geometric mean cotinine in non-smoking children by whether or not home is smoke-free.
Discussion
Our study, based on both self-report and an objective biomarker of exposure, provides evidence that the 2007 ban on smoking in public places in England has not had adverse consequences for children's exposure to other people's tobacco smoke. Concerns that were expressed before the ban was enacted that adult smoking would be displaced back into the home have not been supported.
There was a marked increase in the 10 years since 1998 in the proportion of children living in a smoke-free home, from 64% in 1998 to 80% in 2008. This was due both to an increase in the percentage of parents who were non-smokers (up from 61% in 1998 to 67% in 2008), almost all of whom had smoke-free homes, and to a marked increase in the adoption of smoke-free homes by parents who themselves still smoked. In 2008 close to a half of all such homes were smoke-free, up from only 16% in 1998. Importantly, this trend to smokers making their home smoke-free did not receive a setback from the implementation of the smoking ban in 2007, as some had predicted. Rather, the trend to smoke-free homes was if anything accelerated. It would appear that the widespread acceptance and popularity of the ban on smoking in public places may have reinforced the emerging social norm that smoking in enclosed spaces is not acceptable.
Children's exposure to other people's smoke in England has been declining for over two decades,9 10 and is now greatly reduced from the late 1980s. This secular trend, which has been the product of major changes in smoking prevalence and of the gradual adoption of smoking bans in the workplace and on public transport, makes it more difficult to detect effects on children's exposure specifically attributable to the implementation of the 2007 legislative ban. Interestingly, the biggest declines in exposure came in the period from 2003 to 2006 during the run-up to the legislative ban, suggesting perhaps that the increased focus on secondhand smoke that accompanied the publicity surrounding the legislation's mooting and discussion in parliament may itself have been an important driver of behaviour change. Measured exposure in 2008, whether in children from non-smoking homes or in all children combined, showed only a small reduction from that in 2006 just prior to the ban's introduction. The reassuring conclusion from these data is that predictions of displacement of smoking back into the home have received no support, and this hypothesis can now be robustly dismissed. Our period of follow-up after the ban's implementation was relatively brief, and it may be that in the longer term there will be further impacts on children's exposure as emerging social norms become more firmly entrenched.
Similar trends to reduced exposure to secondhand smoke over the past two decades have been observed in the USA.19 In 2008, 18% of children aged 3–11 in the USA lived with someone who smoked inside the home,20 close to the 20% of English children living in a smoking home. In the USA, the proportion of children whose cotinine was equal to or below a cotinine detection limit of 0.05 ng/ml was 46%,20 again close to the 41% of English children with cotinine below 01.ng/ml.
Our study has a number of strengths. The household based sampling frame of the HSE, with both adults and children being interviewed and measured within the home, enables within-family passive smoking effects to be accurately assessed. The design of the survey permits generalisation to the general population of England. The availability of cotinine measures serves both to validate self-reports and to provide objective quantification of exposure to tobacco smoke. There are also some limitations. In common with other surveys, response rates have declined somewhat in recent years. The relatively small sample sizes when the data for 2007 are divided into 6-month periods, before and after the implementation of the ban, lead to greater imprecision in estimates, with wider CIs. The delay of a week or so between the interview and the nurse visit at which saliva samples for cotinine were collected opens up the possibility of a reactive change in smoking habits in the intervening period. However, it is important to note that the question on whether or not there was smoking in the home was asked at the initial interview. Change in household rules subsequent to the interview but before the cotinine sample would only attenuate the relation between reported household smoking rules and measured cotinine. Furthermore, the report of whether or not there was smoking in the household was gathered from a single adult respondent, who was not necessarily a smoker or the person who smoked in the household. Any bias resulting from delay between interview and sample collection would be present in all survey years, and thus could not explain patterns of exposure change across years. Our operational measure of whether the home was smoke-free specified that there should be no smoking ‘most days’ rather than always. This means that we may have overestimated the percentage of homes that are completely smoke-free. By the same token, we may have underestimated the extent of the reduction in exposure that children receive from living in a smoke-free home. However, since cotinine levels in children with smoking parents but living in a smoke-free home were only modestly raised by comparison with children from completely non-smoking homes, it would appear that the extent of any residual smoking in the home was minimal.
There has been considerable success in reducing children's exposure to other people's smoke in England over the past 20 years, reflecting both declines in cigarette smoking prevalence and earlier moves towards restrictions on smoking in public places. It is encouraging that the gains in reduced adult exposure from the legislative ban implemented in 2007 have not come at the expense of increased child exposure. The national strategy for tobacco control adopted by the previous government earlier this year set a target for the year 2020 of increasing to two-thirds the proportion of homes where parents smoke but that are entirely smoke-free.21 The rapid increase in such homes following the ban suggests that achieving this target could be within reach well before 2020.
What this paper adds
Bans on smoking in public places reduce adults' exposure to secondhand smoke, but effects on children's exposure are less clear, with some suggesting they could increase it, by displacing smoking into the home.
This observational study of cotinine levels in children found no evidence of increased exposure following the implementation of the legislative ban in England in 2007. Adoption of smoke-free homes by smoking parents increased significantly after the ban, suggesting that the ban may have helped reinforce an emerging social norm favouring smoking restrictions.
References
Footnotes
Funding This work was supported by funding from the Department of Health's Policy Research Programme to the University of Bath. AG is supported by a Health Foundation Clinician Scientist Fellowship. MS and AG are members of the UK Centre for Tobacco Control Studies which receives core funding from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council and the National Institute for Health Research under the auspices of the UK Clinical Research Collaboration.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the local ethics committees for the whole of England.
Provenance and peer review Not commissioned; externally peer reviewed.