Article Text

Abstract
AIM To determine normative data for arterial oxygen saturation, measured by pulse oximetry (SpO2), in healthy full term infants throughout their first 24 hours of life.
METHODS Long term recordings of SpO2, pulse waveform, and breathing movements were made on 90 infants. Recordings were analysed for baseline SpO2, episodes of desaturation (SpO2 ⩽ 80%), apnoeic pauses of ⩾ four seconds, and periodic apnoea (⩾ three apnoeic pauses, each separated by ⩽ 19 breaths).
RESULTS Median baseline SpO2 was 98.3% (range 88.7–100). Longitudinal analysis at four hour intervals showed that SpO2 remained stable until 20–24 hours of age, when it became significantly lower (p < 0.03). Episodic desaturations were identified in 23 recordings. Nine prolonged desaturations (SpO2 ⩽ 80% for ⩾ 20 seconds) were identified in six recordings. Four desaturations fell to ⩽ 60%. Periodic apnoea was identified in 60% of recordings.
CONCLUSION The range of SpO2 during the first 24 hours of life is similar to that found previously during the first month of life. The clinical significance of the prolonged episodes of desaturation observed justifies further investigation.
Key messages
Key messages
During the first day of life, healthy term infants have baseline SpO2 values that are very similar to those of older infants, with a range from 89–100%
Four healthy term infants each showed a severe oxygen desaturation; three of these events were not associated with an apnoeic pause
Apnoeic pauses, experienced by most of these infants, are rarely associated with a fall in oxygen saturation to ⩽80%
Nine infants had 10 apnoeic pauses of ⩾20 seconds, only one of which was associated with a fall in oxygen saturation to ⩽80%
- pulse oximetry
- neonate
- oxygen saturation
- apnoea
Statistics from Altmetric.com
Pulse oximetry is widely used in clinical practice to obtain data on arterial oxygen saturation (SpO2). It is a non-invasive technique which requires no calibration and is able to provide instantaneous data, which have been shown to correlate well with blood gas measurements.1-3
This department has published information on SpO2 in healthy full term infants from 2 days of life throughout the first4 and second5 months of life, during infancy,6 and the rest of childhood.7 No infants younger than 24 hours of age were included in these studies. Other investigators have obtained data on SpO2 from infants immediately after delivery.8-11 These measurements were, however, not continuous, which is unfortunate, as many cardiorespiratory changes occur during the first postnatal day. We therefore performed a study to establish oxygen saturation in healthy full term infants during their first 24 hours of life. To our knowledge, this study provides a continuum of information on SpO2 values not previously available for this age group.
Subjects and methods
Infants were recruited during the third trimester of pregnancy, from mothers booked to deliver at the North Staffordshire Maternity Hospital. Mothers were selected by a systematic sampling procedure, and informed parental consent was obtained during pregnancy. The study was approved by the local research ethics committee. Infants were only studied if they were born after 37 weeks of gestation and were apparently healthy upon delivery.
Recordings were made of arterial oxygen saturation as measured by pulse oximetry (SpO2; Nellcor N200/Mallinckrodt, St Louis, Missouri, USA; modified to produce beat to beat measurements), pulse plethysmograph for validation of the SpO2 signal, and breathing movements from a pressure capsule (Graseby Medical, Watford, Herts, UK) taped to the abdominal wall. All monitor alarms were muted. These data were recorded on to portable computers (Apple Inc, Cupertino, CA, USA) and subsequently downloaded and printed on to paper using a thermal printer (Graphtec, Tokyo, Japan). The recordings were printed at 3.1 mm/s.
The printouts were analysed by an experienced research assistant without knowledge of the infants' ages at the time of the recordings. The analysis was performed in accordance with previously published studies.5 Briefly, analysis of baseline SpO2values was restricted to periods of regular pattern breathing (RPB). Apnoeic pauses of ⩾ four seconds were identified in RPB, non-regular pattern breathing (NRPB), and periodic apnoea (PA). These pauses were split into three groups according to their lengths: 4–7.9 seconds, 8–11.9 seconds, and ⩾ 12 seconds. We also identified pauses of ⩾ 20 seconds and looked at surrounding patterns.
PA, defined as the occurrence of ⩾ three apnoeic pauses each separated by ⩽ 19 breaths, was identified. Apnoeas of ⩽ 10 seconds in duration are common in infancy. Pauses in breathing of ⩾ four seconds were chosen to define an apnoeic episode in order to maintain comparability with previous studies.4-7 Other authors include pauses of breathing from ⩾ two seconds,12 ⩾ five seconds,13-15 or ⩾ six seconds in duration.16 Apnoea has arbitrarily been defined as prolonged if there is cessation of breathing for ⩾ 20 seconds, or for a shorter period if it is associated with bradycardia, cyanosis, or pallor.17
Episodic desaturations (SpO2 ⩽ 80%) were identified and their duration recorded. Episodic desaturations that occurred within 12 seconds of the start of an apnoeic pause were also identified.5
After overall measurement, the data were assigned to age intervals to allow sequential analysis; there were therefore six intervals each representing a four hour stage. These intervals represented the postnatal age of the infant. Variables were calculated for each age interval. Results are presented as medians and ranges. Statistical significance was assessed using the Mann-Whitney U test.
Results
Ninety infants were successfully studied (49 boys). Of these, 71 were born by unassisted vaginal delivery, nine by assisted delivery, and 10 by caesarean section (four emergency). Eight infants received bag and mask resuscitation at delivery.
The median age at the commencement of recordings was one hour, and the median duration of recordings was 21.5 hours (range 4.5–23.4). The median duration of RPB was 3.5 hours (range 0.75–6.5). Median baseline SpO2, as measured during RPB, was 98.3% (range 88.7–100). Analysis by intervals of four hours showed that median SpO2was significantly (p < 0.03) lower during the 20–24 hour interval than any other age interval. Although SpO2 was at its highest value during the first four hours after delivery, this was not significantly different (table 1).
Recording results in the first 24 hours after delivery divided into six four hour stages
SpO2 levels in recordings of infants who received bag and mask resuscitation were significantly lower during the 24 hour period (p < 0.03), compared with the other recordings. When analysed in intervals of four hours, SpO2 was found to be significantly lower in these infants during the first eight hours of life (p < 0.05) and also at 20–24 hours of age (p = 0.006).
Seven recordings were excluded from analysis of episodic desaturation. These had low overall baseline SpO2 values (median 91.5%) and saturation was ⩽ 80% in a proportion of their regular breathing episodes; the lowest SpO2 value within an episode of RPB had a median value of 81.2% (range 78.1–88.6). Signal at ⩽ 80% in these episodes did not therefore represent episodic desaturation. If included, it would have inflated the values for the variable artificially, and would have misrepresented the clinical state of these infants; although they had a low baseline saturation, they were not necessarily experiencing falls within it. None of these seven infants exhibited falls in SpO2 of ⩽ 60%. This subgroup of infants included five who were distressed (two received bag and mask resuscitation) and two who were delivered by caesarean section; only one of the seven infants had an unremarkable delivery.
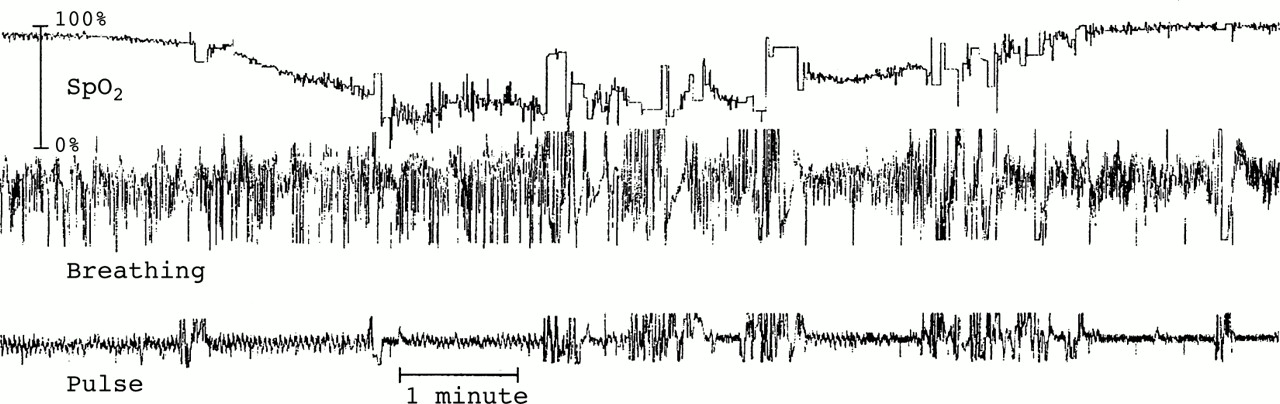
Eighty three desaturations were observed in 23 (26%) recordings. The median number of desaturations, corrected to the median duration of signal (21.5 hours), was 0 (range 0–17.4), with the 90th centile at 4.1. Forty three (52%) of these desaturations occurred without relation to an apnoeic pause; the median duration of these desaturations was 9.3 seconds (range 0.5–286.8). This compared with a median of 0.8 seconds (range 0.3–89.6) in desaturations associated with an apnoeic pause. The longest desaturation observed was therefore 4.8 minutes; for much of this time (4.0 minutes) the SpO2was ⩽ 60%. In addition to the measured artefact free desaturation, there were four brief periods of movement artefact when the infant was probably attempting to improve respiratory function (fig 1). There was no associated apnoeic pause, and this was the only desaturation identified during the recording of this infant. Clinical cyanosis was not reported.

{kind=link}
A severe and prolonged arterial oxygen desaturation.
Prolonged desaturations (SpO2 ⩽ 80% for ⩾ 20 seconds) were identified in six recordings. There were nine such desaturations, the median duration being 41.6 seconds (range 20.8–286.8). Three of the latter desaturations showed falls in SpO2 to ⩽ 60%, as did one other shorter desaturation. The median duration of these desaturations to ⩽ 60% was 14 seconds (range 6.7–237.2). During all four of these desaturations, the infants were reported to have been feeding; none were reported to have become cyanotic. Three of the four episodic desaturations that exhibited falls in SpO2 to ⩽ 60% occurred without association with an apnoeic pause.
Only one recording contained episodes of desaturation (n = 4) during RPB, and these all occurred immediately after apnoeic pauses. During NRPB, only 37% of episodic desaturations was associated with apnoeic pauses.
A minority of apnoeic pauses was associated with an episodic desaturation. In RPB there was a total of four apnoeic pauses (0.3% of all pauses), which were associated with an episodic desaturation, compared with 25 apnoeic pauses (0.3%) in non-regular breathing and 11 apnoeic pauses (0.7%) in PA with such desaturations. Overall, only 0.4% of apnoeic pauses was associated with a desaturation. PA was the only breathing pattern to show desaturations associated with apnoeic pauses in the first four hours of life, although such pauses were only identified in one infant.
Nine infants showed 10 apnoeic pauses of ⩾ 20 seconds in duration, the longest of which was 26.9 seconds. Two of these apnoeas were identified in RPB, four in NRPB, and four in PA. Only one apnoea, the longest, was associated with a desaturation; this resulted in a fall in SpO2 to below 60% for 16 seconds. Of the infants who exhibited apnoeic pauses ⩾ 20 seconds, there were significantly (p = 0.03) more who received bag and mask resuscitation at delivery.
PA was identified in 60% of recordings. In these recordings the median duration was 3.4 minutes (range 0.4–93.9). There were no significant differences between the median durations of PA when analysis was performed across intervals of four hours. The median number of episodes of PA per recording was four (range 1–55); the longest episode of PA was 5.3 minutes.
Discussion
We have defined reference data for aspects of oxygen saturation in healthy full term infants during their first 24 hours of life. Median baseline SpO2 values were higher than those reported for the first week of life,4 and were relatively stable across the first 24 hours. The median value at 20–24 hours of life (97.8%) is similar to that previously reported for healthy full term infants between 2 and 7 days of age (97.6%),4 using similar experimental methods.
Lower SpO2 values in the period after bag and mask resuscitation at birth have not been reported previously. They are, perhaps, not surprising as the necessity to resuscitate an infant may reflect lower lung volumes after delivery and this may continue to be reflected in the significantly lower saturations measured during the first eight hours of life. A mismatching of ventilation and perfusion in areas of atelectasis can result in right to left shunting within the lung. The significantly lower values in SpO2 observed during the 20–24 hour age interval were unexpected and remain unexplained.
Episodes of desaturation, during which SpO2 fell to ⩽ 80%, were relatively uncommon, with only 26% of recordings containing such episodes. Only 20% of recordings contained episodic desaturations ⩾ four seconds in duration. The four infants who exhibited severe desaturations (SpO2 ⩽ 60%) were all reported to have been feeding, and these infants may have had difficulty coordinating breathing and feeding.18 ,19 None of the previous studies that monitored SpO2 levels during the first postnatal day8-11 reported data on episodic desaturations.
The desaturations that occurred without association with an apnoeic pause were more frequent and of longer duration than those that occurred in relation to a pause. This may suggest that ventilation/perfusion mismatching or obstructive apnoea have a role to play, although airflow was not measured in this study so obstructive apnoea could not be identified. Hypoventilation may be a contributing factor in some desaturations, particularly as this has been observed in newborn infants during feeding.20 Our methodology does not enable quantitative analyses to be undertaken on the breathing pattern. Rapid depletion of small lung oxygen stores after an apnoeic pause21 may only partly explain the desaturations observed, particularly when the desaturation is severe, as the circulation time for blood in infants is rapid (five to nine seconds).22 The proportion of apnoeic pauses of ⩾ four seconds associated with a desaturation (0.4%) also suggests that apnoeas are not the only cause of desaturation during the first day of life.
Although there is a wealth of information describing pauses in breathing as “apnoeas” when the duration of the pause is between two and six seconds,4-7 12-16 the clinician is more interested in apnoeas lasting ⩾ 20 seconds. Very few infants (n = 9) in this study exhibited this phenomenon, which is in accordance with other studies15 ,16 ,23 performed within a few days of birth. However, three of the eight infants receiving bag and mask resuscitation had apnoeic pauses ⩾ 20 seconds. The significance of bag and mask resuscitation to prolonged apnoeic pauses is not clear, although the process of resuscitation may affect lung mechanics, particularly in infants who have never breathed and whose lungs still contain fluid.
Some previous studies have shown no evidence of PA before about 48 hours of age.24 ,25 The present study is in agreement with that of Fenner et al 26 in that PA was observed in full term infants less than 48 hours old. In contrast with the results of Fenner et al, who found PA in 41% of infants, the present study found PA to occur in most of the infants studied (60%). Different definitions of PA may have contributed to the discrepancy between reports.
In conclusion, reference values for baseline SpO2 and its relation to breathing pattern have been obtained in 90 healthy full term infants throughout the first 24 hours of life. Baseline oxygenation was relatively stable during the first postnatal day, slightly higher than we have shown in healthy full term infants during their first month of life, but lower than in older infants. Episodic desaturations were apparent in 26% of infants studied, and several infants exhibited severe and prolonged episodes, most of which occurred without association with an apnoeic pause. The clinical significance of these episodes remains to be determined. PA has been identified in the breathing pattern of full term infants during their first day of life.
Acknowledgments
Our thanks go to the parents who allowed us to monitor their babies, the midwifery staff of the North Staffordshire Hospital, and Mrs Jackie Kelly who analysed the recordings. Thanks also to Mrs Fozia Hussain who assisted with the data collection. The recording/analysis equipment and consumables were provided by financial contributions from Babes in Arms, Cot Death Research, Little Ones, and the Sir Jules Thorn Trust. Mr Andrew Holder (Research Monitoring Systems, Salisbury, Wilts, UK) and Dr Chris Hall (Bournemouth University, UK) developed the recording systems.