Article Text

Abstract
Background Newborn screening (NBS) for cystic fibrosis (CF) is associated with improved early nutritional outcomes and improved spirometry in children. The aim of this study was to determine whether early diagnosis and treatment of CF with NBS in New South Wales in 1981 led to better clinical outcomes and survival into early adulthood.
Methods Retrospective observational study comprising two original cohorts born in the 3 years before (‘non-screened cohort’, n=57) and after (‘screened’; n=60) the introduction of NBS. Patient records were assessed at transfer from paediatric to adult care by age 19 years and survival was documented to age 25 years.
Results Non-screened patients (n=38) when compared with screened patients (n=41) had a higher rate and lower age of Pseudomonas aeruginosa acquisition at age 18 years (p≤0.01). Height, weight and body mass index (BMI) z scores (all p<0.01) and forced expiratory volume in 1 s (FEV1)% were better in the screened group (n=41) (difference: 16.7±6.4%; p=0.01) compared to non-screened (n=38) subjects on transfer to adult care. Each 1% increase in FEV1% was associated with a 3% (95% CI 1% to 5%; p=0.001) decrease in risk of death and each 1.0 kg/m2 increase in BMI contributed to a 44% (95% CI 31% to 55%; p<0.001) decrease in risk of death. This accumulated in a significant survival difference at age 25 years (25 vs 13 deaths or lung transplants; p=0.01).
Conclusion NBS for CF leads to better lung function, nutritional status and improved survival in screened patients in early adulthood.
Statistics from Altmetric.com
Introduction
Newborn screening (NBS) programmes for cystic fibrosis (CF) have been introduced in many countries; the state of New South Wales (NSW) in Australia was one of the first to begin NBS in July 1981. The impact of NBS on clinical outcomes has previously been reported at ages 5–10 and 15 years and demonstrated better clinical outcomes for nutrition and lung function in screened patients.1 2 In this report, we extend our observations and include a survival analysis of these cohorts into early adulthood.
Material and methods
Study design
Retrospective analyses of nutritional and spirometric outcomes for each cohort were compared at the age of transfer from paediatric to adult care and survival to age 25 years was assessed. The study was approved by the ethics committee at The Children's Hospital at Westmead, Sydney (QIE-2010-08-19).
What is already known on this topic
▶ Newborn screening programmes for cystic fibrosis have been operating for up to 30 years.
▶ Generally, newborn screening programmes have shown improved nutrition and spirometry but not a consistent survival benefit in childhood.
What this study adds
▶ Nutritional and spirometric outcomes are superior at transfer to adult care in children with cystic fibrosis diagnosed on newborn screening compared with those diagnosed symptomatically.
▶ Newborn screening for cystic fibrosis translates into improved survival at age 25, predicted by higher body mass index and FEV1% values at transfer to adult care.
Patients
A historical cohort was formed comprising patients diagnosed in the 3 years before and in the 3 years after the introduction of NBS. A total of 57 patients with CF were born before the NSW NBS program was introduced (July 1978 to July 1981, ‘non-screened’) and 60 infants were born during the first 3 years of the program (July 1981 to July 1984, ‘screened’). Infants from both groups were referred to the CF clinic at the Royal Alexandra Hospital for Children in Sydney.
A two-step immuno-reactive trypsinogen (IRT) protocol was used for the NBS process in our centre between July 1981 and October 1996. The dried blood IRT level on the newborn heelprick sample was measured with inclusion of a second test several weeks later when a child had an initially elevated IRT level (top 1% of results). If an infant had a raised second IRT, a sweat test followed to confirm the diagnosis at around 6 weeks of age.
Data collection
Data on clinical outcomes were recorded from the patients' medical records and results from the respiratory laboratory, with the last measurement being collected before the patients were transferred to adult care by age 19 years. Additionally, information on subsequent deaths of patients up to the age of 25 was provided by the national CF registry database and adult CF clinics.
Outcome measures
Clinical outcome measures included anthropometry, airway colonisation and spirometry measured.
Z scores were used to express height, weight and body mass index (BMI) and were obtained using values from the WHO.3 Sputum cultures were obtained to analyse airway colonisation with Pseudomonas aeruginosa. Spirometry was measured according to standard American Thoracic Society (ATS) criteria.4 Parameters assessed include forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and forced expiratory flow rate in the middle half of FVC (FEF25–75). Outcomes were converted to percentages using the Polgar and Promadhad reference dataset.5 The Shwachman score was recorded.6 Survival was determined at age 18 and age 25 with death or lung transplant as outcome values.
Statistical analysis
Statistical analyses were performed using SPSS v 18.0 for Windows (SPSS, Chicago, Illinois, USA). Statistical comparison between groups, using only patients with complete data at age of transfer to adult care, was carried out using Pearson's χ2 test for categorical variables and one-way analysis of variance (ANOVA) or the Student t test for continuous normally distributed variables. The Pearson's correlation coefficient was used to determine correlation between continuous variables.
The survival of screened and non-screened patients in the total cohort was compared using Cox proportional hazards models at age 18 years. For cumulative survival, a Kaplan–Meier curve was estimated for survival data to age 25 years.
Results
Between birth and age of transfer to adult care, 12 patients in the screened group and nine in the non-screened group transferred to another clinic or were lost to follow-up. In the screened group, seven children died before transfer to adult care, compared with eight in the non-screened group. As a result, complete data at age of transfer to adult care were available for 41 screened children and 38 non-screened children (figure 1).

Flow diagram with number of patients with complete data at age 5, 10, 15 and 18 years.
Demographic characteristics are outlined in table 1. The age of diagnosis for the non-screened group, born between July 1978 and June 1981, was as follows: 53% diagnosed by 6 months, 70% by 12 months, 91% by 2 years. Eighteen of the 57 patients (32%) in the non-screened group were diagnosed and started on treatment after the commencement of newborn screening on 1 July 1981. There were no significant differences between the groups other than the age of diagnosis. The CF gene mutations were known for 37 of 41 patients in the screened cohort, of whom 57% (n=21) were homozygous ΔF508.
Demographic comparison between screened and non-screened cohort
Nutrition
At the time of transfer to adult care, the screened cohort had significantly better nutritional status. Children in the screened group were (mean difference±SEM) 6.4±2.05 cm taller (p=0.003) and 6.9±2.2 kg heavier (p=0.005) than children in the non-screened group (figure 2). Analysis of the BMI z scores revealed a significant difference of 0.6±0.2 in favour of the screened group (p=0.006). Results were not altered when adjusted for pancreatic status (confirmed by 3 days of faecal fat collection).

Comparison between mean height z scores, mean weight z scores and mean body mass index (BMI) z scores with 95% CI for screened (n=41) and non-screened (n=38) cohorts at transfer to adult care. The p value is calculated with analysis of variance.
Airway bacterial pathogens
In the year of transfer to adult care, 100% of children in the non-screened group had at least one P aeruginosa positive sputum culture as opposed to 92% in the screened group (p=0.24). A significant difference was demonstrated for the number of children having chronic (defined as three successive positive sputum cultures) or mucoid P aeruginosa colonisation, with 77% children in the screened group having chronic or mucoid colonisation compared with 100% in the non-screened group (p=0.01). Screened children were significantly older when they were infected for the first time with P aeruginosa (figure 3), when they had their first chronic P aeruginosa isolate and when they had their first mucoid P aeruginosa isolate (figure 3) (all p<0.01).

Delay in acquisition of first Pseudomonas aeruginosa (PsA) infection and mucoid PsA infection. Black lines (screened patients) and grey lines (non-screened patients) represent the percentage of children not having PsA colonisation. First PsA colonisation p=0.002, mucoid PsA colonisation p<0.0001; Cox regression.
There was a significant association between age of onset of P aeruginosa infection and clinical outcomes, with children who had earlier infection having worse nutrition and lower lung function. One of the strongest correlations was seen between the age of first mucoid P aeruginosa sputum culture and FEV1%, with a Pearson correlation coefficient of 0.54 (p<0.0001). Another clinically important correlation was between P aeruginosa infection and nutritional outcome, with a correlation coefficient for age of first mucoid P aeruginosa and BMI of 0.31 (p=0.01).
Lung function
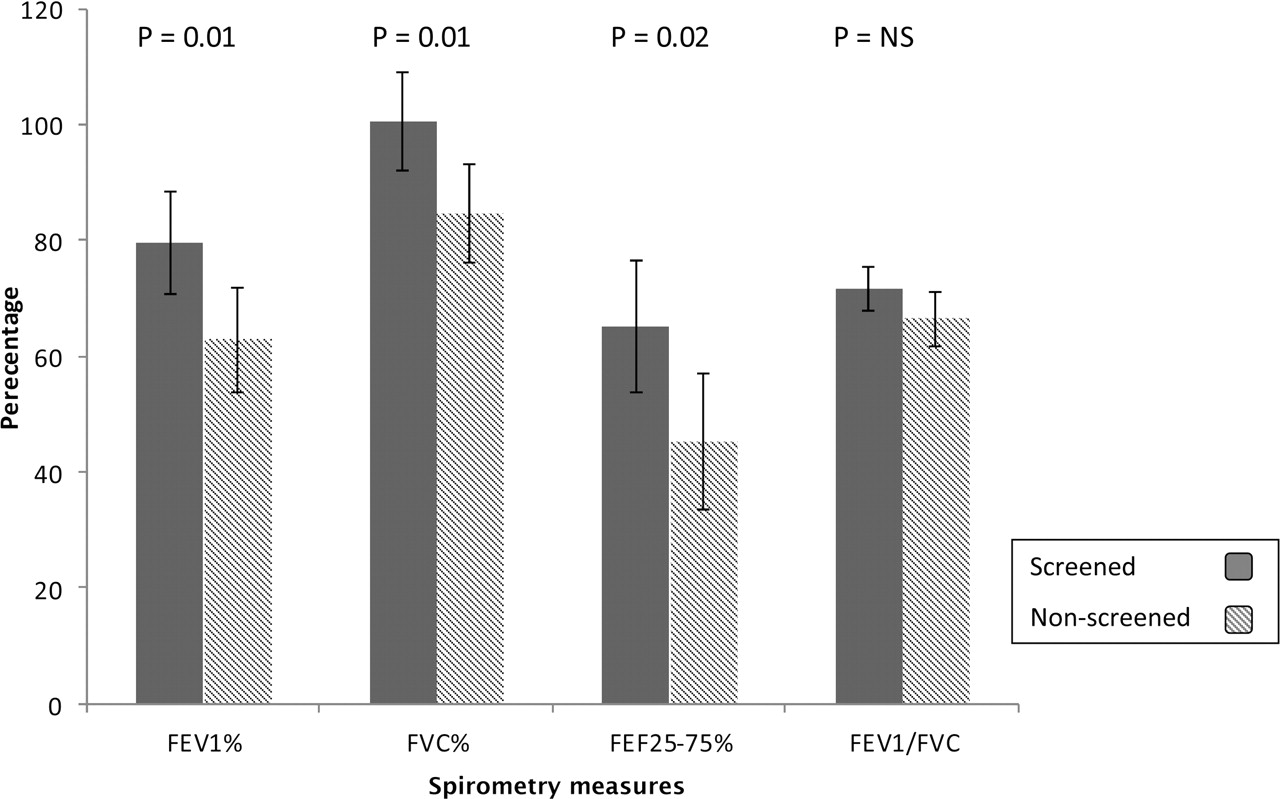
Lung function was superior in the screened group with significant differences in FEV1% (mean±SD) (62.8±28.5% vs 79.5±28.4%; p=0.01), FVC% (84.6±27.1% vs 100.5±27.5%; p=0.01) and FEF25–75% (45.3±33.8% vs 65.1±37.1%; p=0.02). The difference between FEV1/FVC ratio was not significant (66.5±14.0% vs 71.6±11.4%; p=0.09). Lung function results were not altered when adjusted for liver transplant (non-screened n=2 and screened n=1) or pancreatic sufficiency status. At the time of transfer to adult care, Shwachman scores were (mean difference±SEM) 9.1±3.9 points higher (p=0.03) in the screened group.
Longitudinal differences
The cumulative benefits of NBS become apparent with increasing age when data from ages 5, 10 and 15 years1 2 were compared with that at transfer to adult care. The difference in nutritional outcomes became more obvious at the time of transfer to adult care, with a significant difference for both height and weight (all p<0.01). Lung function measurements were consistently better in the screened group, with the difference also becoming more evident over time (figure 4). The mean difference for FEV1% increased from (mean difference±SEM) 9±3.3% at age 5 years (all p<0.01) to a mean difference of 16.7±6.4% at age of transfer to adult care (all p<0.01). Shwachman scores remained consistently higher in the screened group throughout childhood.

Comparison between mean lung function parameters with 95% CI for the screened (n=41) and non-screened (n=38) groups at transfer to adult care. The p value is calculated with ANOVA. The black bars indicate the screened cohort. FEF25–75, forced expiratory flow rate in the middle half of FVC; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity.
Survival
Death before transfer to adult care by age 19 occurred in 21 children in the total cohort. In the non-screened group, 13 children died (23%) compared with eight children in the screened group (13%). Analysis using Cox regression demonstrated a non-significant 43% mortality risk reduction in screened patients as compared to non-screened patients (hazard ratio (95% CI): 0.57 (0.24 to 1.38); p=0.21).
The influence on survival was calculated for sex, pancreatic status, FEV1% and BMI. Sex and pancreatic status did not influence survival between groups. Each 1% increase in FEV1% was associated with a 3% (95% CI 1% to 5%; p=0.001) decrease in risk of death. Subsequently, each 5% increase in FEV1% led to a 14% (95% 6% to 21%) reduction and each 10% increase in FEV1% led to a 25% (95% CI 11% to 37%) reduction in mortality risk. Each 1.0 kg/m2 increase in BMI contributed to a 44% (95% CI 31% to 55%; p<0.001) decrease in risk of death.
Difference in survival did not reach significance at age 15 years or by age 19, but became significant at age 25 years with death or lung transplant occurring in 25 people (23 deaths and two lung transplants) in the non-screened group, in comparison with 12 deaths and one lung transplant in the screened group (25 vs 13; p=0.01) (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Screened patients (diagnosed through newborn screening from July 1981 to July 1984) are shown by the dark line, and non-screened patients (diagnosed clinically from July 1978 to July 1981) are represented by the grey line (p=0.01; Kaplan-Meier survival analysis).
Discussion
This report is part of one of the longest running observational cohort studies investigating the effects of diagnosing CF through NBS. Results in this paper reveal better nutritional outcomes and the maintenance of superior lung function at the time of transfer to adult care, extending the previously demonstrated benefits from NBS diagnosis at 5, 10 and 15 years of age. Importantly, the advantage of NBS translates into improved survival in early adulthood.
The difference in nutritional status at diagnosis can be reduced after necessary adjustments in diet, including pancreatic enzyme replacement therapy.2 7,–,9 However, considering our cohort and data from other studies, the effect of late diagnosis may have such a dramatic impact on nutritional state and lung function at a crucial stage in early development that non-screened children may not fully recover.10,–,15 This may translate into a delayed impact upon survival which may not become evident until the adult years. Moreover, our data confirm that good nutritional status is associated with a reduction in the prevalence of P aeruginosa colonisation and better respiratory function and prognosis.16 17
Studies have reported different outcomes in CF following airway bacterial infection.18 Observational studies from France and the Netherlands showed no significant difference in the isolation rates of or age of colonisation with P aeruginosa between screened and non-screened patients.8 14 This is in contrast with our study, with screened patients having a significantly older age of and lower rate of a first time infection with P aeruginosa or the development of a chronic or mucoid P aeruginosa infection. Our findings are supported by US CF registry data.13
The benefits on pulmonary outcome of NBS remain controversial.1 2 8 14 15 19,–,21 Several studies, including earlier results from our cohort, have shown that early diagnosis leads to superior respiratory function.1 2 We now report better lung function in the screened group for FEV1%, FVC% and FEF25–75% at transfer to adult care. The difference in lung function between groups suggests that there is a cumulative benefit of NBS favouring screened patients with age.
In contrast, a randomised controlled trial in Wisconsin showed fewer abnormalities on the first chest radiograph (CXR) in a screened group, but after 10 years of age results reversed with screened patients showing worse CXR scores.19.20 However, this latest finding was associated with earlier acquisition of P aeruginosa. Our study confirmed worse results with colonisation with P aeruginosa, although it occurred in our non-screened group.
There are few data on the long-term survival effects of NBS. Results from our cohort demonstrate a remarkable difference at age 25 years in mortality, with 25 deaths (or lung transplants) in the non-screened cohort (44% of the original non-screened cohort) compared with 13 deaths (or lung transplants) in the screened cohort (22%). This extends the observations of other studies which have reported survival differences at younger ages.7 9 12 14 Dankert-Roelse et al found a survival rate of 94% at the age of 11 in a screened group, in comparison with 65% in subjects clinically diagnosed (p<0.05).7 Our screened cohort has a consistent survival advantage throughout the follow-up period, which reached significance at age 25 years. The reasons are likely to be multifactorial. Potential explanations for the altered survival in a subset of non-screened patients may involve those with late diagnoses being more vulnerable to the effects of earlier infection with P aeruginosa, and having poorer lung function, phenotypically and or genetically more severe disease and perhaps poorer adherence with therapies. The fact that there is an apparent time lag before the impact of a worse clinical state is actually demonstrable on survival might be due to a cumulative effect of non-recoverable pulmonary and nutritional compromise from early childhood leading to less reserve during advanced stages of the disease.
Study limitations
A limitation of our study is the lack of availability of data for those lost to follow-up and incomplete data from the adult years. Despite considerable efforts, it was not possible to extract all the required data from adult centres or the limited information that was sent to the national CF registry database (which in Australia is sent voluntarily). Consequently, the only confirmed information available from adult care was that of survival, reported to the age of 25 years. Our study at age 18 years has comparable numbers of children from the original cohorts with complete data records (41 screened vs 38 non-screened) and a similar number of children who transferred to a hospital outside the region or who were lost to follow-up from the beginning of the study (12 vs 10). Genetic results were not available for all patients, but we assumed that in both of the cohorts approximately 50% of the children would have been homozygous ΔF508. This has been a consistent finding since the introduction of genotyping in our clinic.
During the 18 years of follow-up, there have been changes in the treatment modalities for CF patients. However, the cohorts spanning an enrolment period of only 6 years were managed in the same centre with the same treatment modalities in both cohorts.
Conclusion
For CF patients, we report a better nutritional outcome, an older age of acquiring P aeruginosa in sputum and superior lung function in screened patients at the age of transfer to adult care in comparison with non-screened patients. These cumulative benefits through childhood are predictors of survival, contributing to an increased survival at age 25 in our screened cohort. Our clinical and survival data underscore the long-term advantages of NBS for CF and argue persuasively for its implementation in countries with a high prevalence of CF.
Acknowledgments
The authors are grateful to Mr Geoff Sims for his assistance in accessing and interpreting data from the Cystic Fibrosis in Australia database, Professor Craig Mellis from Royal Prince Alfred Hospital, Professor Adam Jaffe from Sydney Children's Hospital, Associate Professor Peter Middleton from Westmead Hospital and Associate Professor Peter Wark from John Hunter Hospital in Newcastle. The authors thank Professor Bridget Wilcken and Professor Kevin Gaskin for their advice on the preparation of this manuscript as well as Mr Brendan Kennedy and Ms Anita Merchant for their assistance in accessing data in the respiratory function laboratory.
References
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The authors have requested a point of clarification regarding the timing of the diagnosis of cystic fibrosis in the non-screened cohort. Thus in the Abstract, in the Methods, it has been reworded as follows: “Retrospective observational study comprising two original cohorts born in the three years before (“non-screened cohort”; n=57) and after (“screened”; n=60) the introduction of NBS”.
Also, the following has been added as the second sentence in paragraph 2 of the Results section: “The age of diagnosis for the non-screened group, born between July 1978 and June 1981, was as follows: 53% diagnosed by 6 months, 70% by 12 months, 91% by 2 years. Eighteen of the 57 patients (32%) in the non-screened group were diagnosed and started on treatment after the commencement of newborn screening on 1 July 1 1981. There were no significant differences between the groups other than the age of diagnosis.”
Finally, author Karen McKay has had her Sydney University affiliation noted.
-
Competing interests None.
-
Ethics approval The Ethics Committee of the Children's Hospital at Westmead and the Advisory Board for the Cystic Fibrosis in Australia database approved this study (QIE-2010-08-19).
-
Provenance and peer review Not commissioned; externally peer reviewed.