Article Text

Abstract
Objectives To determine: (a) prevalence of clinically unsuspected nocturnal hypoventilation (NH) in a clinic population of children with progressive neuromuscular disease; (b) whether NH can be predicted from clinical/laboratory parameters; and (c) change over 1 year in pulmonary function decline, quality of life and attention in children with NH treated with non-invasive positive pressure ventilation (NPPV) compared with children without NH.
Design Prospective cohort study.
Setting Two tertiary-care paediatric neuromuscular clinics.
Patients 46 children (6–17 years) with progressive neuromuscular disease without neurocognitive impairment or dystrophinopathy.
Interventions Polysomnography, pulmonary function, manual muscle strength, quality of life (CHQ-PF50) and Conners questionnaires.
Outcome measures (a) Prevalence of NH; (b) predictive value of surrogate clinical measures for NH; and (c) differences in change over 1 year in pulmonary function, muscle strength, quality of life and attention between children with and without NH.
Results Prevalence of NH was 14.8%, 95% CI 8.0% to 25.7%. Maximal sensitivity and specificity for NH were achieved with thresholds of forced vital capacity <70% and forced expiratory volume in 1 s <65% predicted (sensitivities: 71.4, 71.4; specificities: 64.1, 79.5). Scoliosis also predicted NH (sensitivity 88.9; specificity 80.4). Over 1 year, those with NH had a greater increase in residual volume/total lung capacity (0.075 (−0.003 to 0.168) vs −0.03 (−0.065 to 0.028)), decline in muscle strength (−0.67 (−0.90 to 0.10) vs 0.53 (−0.05 to 0.90)) and worsened perception of health status.
Conclusions 15% of subjects had clinically unsuspected NH, predicted by moderate pulmonary function test impairment and scoliosis. Over 1 year those with NH had increased gas trapping, decline of muscle strength and worse perception of health status, despite NPPV.
Statistics from Altmetric.com
Introduction
Nocturnal hypoventilation (NH) develops with respiratory muscle involvement in progressive neuromuscular conditions.1 NH, however, may be difficult to diagnose in a clinic setting as symptoms are insidious.2 3 Daytime clinical assessments and pulmonary function tests (PFTs) fail to reliably identify patients with NH.4 5 Overnight polysomnography remains the gold standard for documenting sleep-related hypoventilation,1 6 but has limited availability. Optimal timing and indications for screening children with neuromuscular disease using polysomnography are not known.
What is already known on this topic
▶ Nocturnal hypoventilation (NH) develops insidiously in neuromuscular conditions and is difficult to detect with daytime clinical assessments. It is often the first manifestation of respiratory failure.
▶ Daytime clinical assessments with pulmonary function tests have failed to reliably identify NH until diurnal respiratory failure is present, indicating advanced stages of disease.
▶ Nocturnal non-invasive ventilation for NH improves survival and quality of life in children with neuromuscular disease. It may minimise loss of chest wall compliance.
What this study adds
▶ The prevalence of nocturnal hypoventilation (NH) is common (15%) in children with neuromuscular disease, regardless of symptoms. Clinicians should screen for NH with polysomnography.
▶ Clinical predictors of isolated NH include pulmonary function (forced vital capacity <70%/forced expiratory volume in 1 s <65%) and scoliosis, which can be used to prioritise individuals for screening.
▶ This study prospectively compares change in pulmonary function, muscle strength, quality of life and attention between children with NH (non-invasive positive pressure ventilationtreated) and those without.
Detection of NH is important, however, since treatment with nocturnal non-invasive positive pressure ventilation (NPPV) may be offered earlier. Small uncontrolled studies of NPPV in children with chronic respiratory failure have demonstrated survival4 7,–,10 and quality of life benefits.5 7 11,–,13 Blood gas values also improve when NPPV is used to treat NH,14 although its effect on preservation of pulmonary function is unknown. The impact of NPPV on other facets of neuromuscular disease also remains unexplored. It may aid neurocognitive function in a manner analogous to correction of sleep-disordered breathing caused by obstructive sleep apnoea,15,–,21 which, like NH, results in sleep fragmentation and hypoxaemia. If such benefits of NPPV are documented, this would provide additional impetus to initiate treatment earlier in the disease process for children with neuromuscular disease.
This study therefore aims to determine: (1) the prevalence of NH in children with progressive neuromuscular disease; (2) clinical and laboratory features that predict the presence of NH; and (3) change over a 1-year period in pulmonary function, muscle strength, quality of life and attention, in a cohort of children with progressive neuromuscular disease with NH (treated with NPPV) and without NH.
Design and methods
A cross-sectional study design was used to assess prevalence of undetected NH (primary outcome) and predictive value of clinical and laboratory parameters for NH (secondary outcomes), followed by a 1-year prospective cohort study to assess the change over 12 months in other secondary outcomes. The study was conducted from December 2002 to May 2007. Ethics approval for this study was obtained at both study sites.
Participants
Children with progressive congenital neuromuscular disease, aged 6−17 years, were recruited from two tertiary care neuromuscular clinics; the Hospital for Sick Children (SickKids), Toronto, Canada and the Children's Hospital of Eastern Ontario (CHEO), Ottawa, Canada. Children with dystrophinopathies, cognitive impairment, known NH, daytime hypercapnia, chronic lung disease, congenital heart disease, acquired neuromuscular disorders and those unable to communicate in English or French were excluded.
Interventions
Polysomnography was performed according to American Thoracic Society standards.22 Baseline oxygen saturation and end-tidal pCO2 were measured while awake and recorded during polysomnography. Polysomnography parameters were analysed for the apnoea-hypopnoea index, number and degree of desaturations. With no consensus at the onset of the study as to a strict definition in children,12 23 sleep-related hypoventilation was defined as an elevated pCO2 (increase of 10 mm Hg in end-tidal pCO2) and/or a fall of at least 5% in oxygen saturation for greater than 10 min, associated with a significant reduction in tidal volume, measured by respiratory inductance plethysmography (reflecting values for gas exchange that are outside normal limits).22 Apnoea was defined as a cessation of airflow with duration of >10 s. Hypopnoea was defined as a reduction in airflow or chest wall motion of >50%, resulting in a drop in arterial oxygen saturation of at least 4%. The apnoea-hypopnoea index was calculated as the number of apnoeas plus the number of hypopnoeas divided by the total sleep time in hours.
Polysomnograms were performed at baseline and 1 year for those with no evidence of NH. Those identified to have NH were initiated on NPPV treatment within 1 month of the initial polysomnogram. Repeat polysomnograms for titration were performed at 1−3, 6 and 12 months after initiation of NPPV.
Body mass index Height (measured with a stadiometer when possible or by arm span for those who were wheelchair dependent) and weight were measured at baseline. Body mass index (BMI) was calculated as weight in kilograms divided by height in metres2.
Scoliosis The presence of scoliosis was ascertained by questionnaire, the degree verified by review of spine imaging reports.
Pulmonary function testing was performed according to American Thoracic Society standards, at baseline and 1 year.24 Outcomes included forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, forced mid-expiratory flow (FEF25–75), plethysmography (total lung capacity (TLC), residual volume (RV), RV/TLC ratio) and maximal inspiratory and expiratory pressures (MIP and MEP).
Manual muscle strength testing was performed at baseline and 1 year on all children by a paediatric physiotherapist, blinded to laboratory results. Manual muscle strength assessments were obtained for eight ipsilateral muscle groups, according to the validated Lindsley protocol.25 Scores were assigned based on the Kendall scale.26
Quality of life The Child Health Questionnaire (CHQ-PF50),27 an established paediatric multidimensional instrument addressing physical, emotional and social well-being, was administered to parents at baseline and 1 year, to assess health status and quality of life.
Conners Rating Scale This validated questionnaire28,–,30 assessing attention, hyperactivity and impulsivity in children, was administered to parents at baseline and 1 year.
Outcome measures
Primary outcome
Prevalence of NH in an unscreened clinic population of children and adolescents with progressive neuromuscular disease.
Secondary outcomes
Predictive value of surrogate clinical measures (degree of scoliosis, manual muscle strength testing, PFTs, BMI) for NH.
Difference in change over 1 year in pulmonary function, manual muscle strength, quality of life and attention between children with NH (treated with NPPV) and without NH.
Statistical analysis
The Wilson score with continuity correction was used to calculate a 95% CI around the prevalence of sleep-related hypoventilation estimate.31 Descriptive statistics were generated on each measure/score for children with or without hypoventilation, to characterise both groups. Continuous variables that were not normally distributed were represented with median and IQR. Demographic and clinical characteristics at baseline were compared between study groups using Student's t tests or Mann–Whitney tests for continuous characteristics and Fisher's exact tests for dichotomous variables. Logistic regression was used to assess the relationship between the study groups for a series of clinical measures and indices.
The secondary objective consisted of assessing the sensitivity and specificity of the seven specific measures/indices to predict hypoventilation. Data from participants were cross-tabulated according to hypoventilation status and dichotomised score on the following measures: manual muscle strength testing (score above/below 5), pulmonary function testing (FVC, FEV1, MIP and MEP >50% predicted vs <50% predicted, chosen to reflect a value greater than the 40% cut-off in Hukins' study4), BMI percentiles (above/below the 95th percentiles) and presence or absence of scoliosis.
Descriptive statistics were used to summarise change over 1 year from baseline on participants for whom a complete dataset was available. The small number of participants that met the criteria for NH precluded performance of statistical tests. No adjustment for multiple testing was applied and a two-sided p value <0.05 was deemed significant.
Results
A total of 46 subjects participated in the study (n=31 at SickKids, n=15 at CHEO). Demographic features are described in table 1. No participants had cardiomyopathy. None were receiving cough assistance.
Demographic characteristics
The participation rate was 65%. The most common reason for non-participation was the time commitment required.
The prevalence of NH in this unselected group of children with progressive neuromuscular disease was 15.2% (7/46; 95% CI 7.6 to 28.2). Two subjects in the study had clinically significant obstructive sleep apnoea (obstructive apnoea-hypopnoea index 9.5, 10.9 events/h, with desaturations). One was treated with adenotonsillectomy; the other had concurrent NH, which was treated with NPPV. Symptoms of sleep disturbance and daytime fatigue were relatively rare and occurred more frequently in those without NH than in the NH group (table 2).
Symptoms at baseline
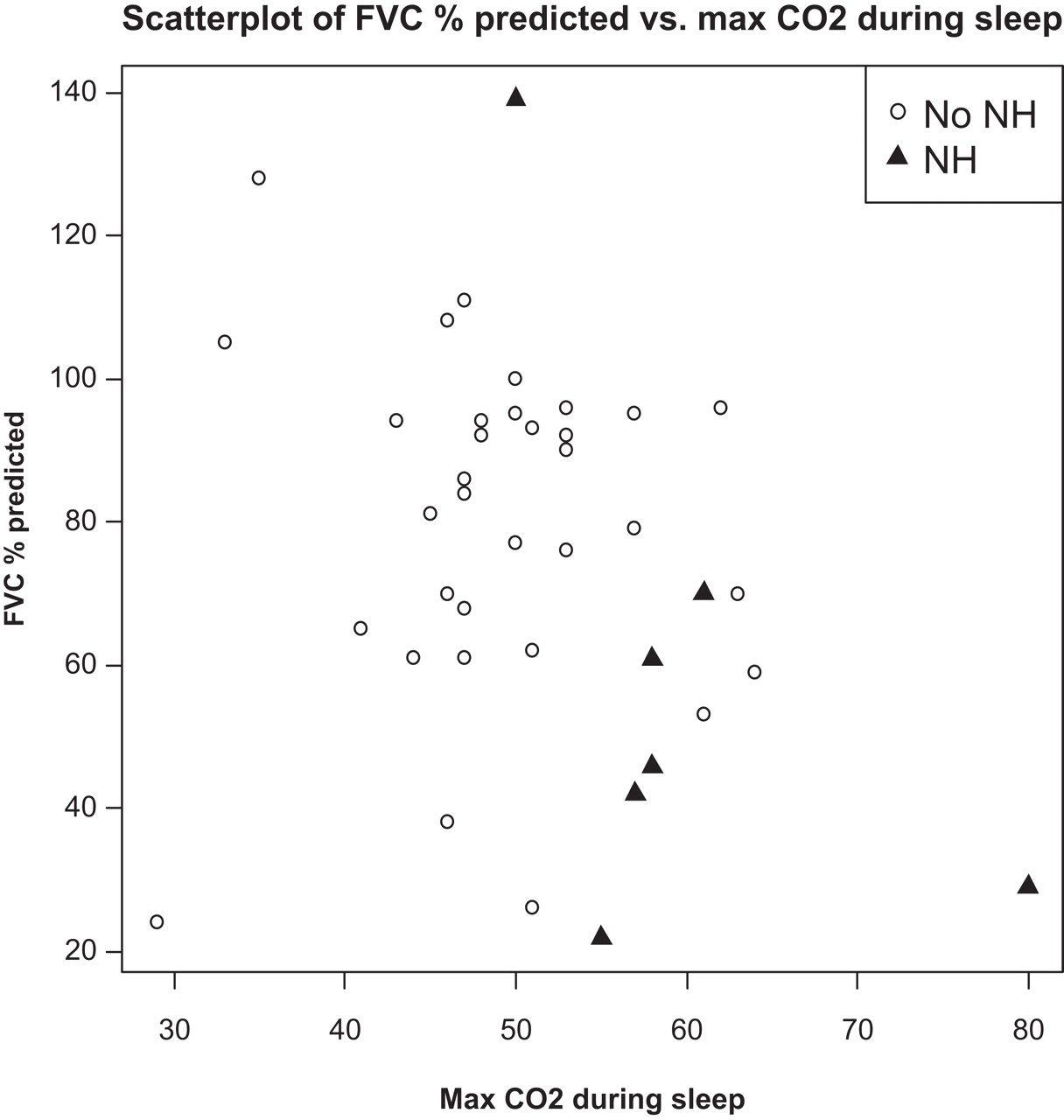
PFTs were predictive of the presence of NH (table 3). Specifically, FVC or FEV1 <50% predicted was significantly more common in the NH group, although sensitivity was relatively low, ranging from 43% to 57%. Maximal sensitivity and specificity for NH were achieved with thresholds of FVC <70% (sensitivity 71.4; specificity 64.1) and FEV1 <65% predicted (sensitivity 71.4; specificity 79.5). Those with NH had lower baseline FVC and higher maximum carbon dioxide during sleep (figure 1). Surrogate measures of respiratory muscle strength (MIP and MEP) were not significant predictors of NH. Pulmonary function results were unrelated to wheelchair use in any of the study groups.
{kind=link}
Relationship of baseline forced vital capacity and maximum carbon dioxide during sleep.
Clinical predictors
The presence of scoliosis was another significant predictor of NH (table 3). The median (range) Cobb angle was 19° (10–35°) in the group without hypoventilation and was 33° (7–56°) in the group with hypoventilation (data available for seven participants in each group).
BMI was also not predictive of NH (evaluated as both a continuous and dichotomous (above/below the 95th percentile) variable). No other baseline demographic characteristics were found to be associated with NH (table 1).
Differences in change over 1 year were also evaluated between those with NH (treated with NPPV), and those with no NH (table 4). There was a trend towards more rapid decline in pulmonary function in children with NH, although this was not statistically significant, possibly due to the small sample (n=4). Gas trapping, assessed by RV/TLC, progressed more rapidly in those with NH (0.075 (−0.003 to 0.168) vs −0.03 (−0.065 to 0.028, p=0.031)). In addition, manual muscle strength declined more rapidly (−0.67 (−0.90 to 0.10) vs 0.53 (−0.05 to 0.90), p=0.019). A greater decline in general perception of health status was also seen in those with NH. There were no significant differences in attention and hyperactive/impulsive behaviours over the year.
Change over 1 year
Discussion
NH requires nocturnal respiratory monitoring for definitive diagnosis. Signs and symptoms of NH are vague and, when present, do not reliably predict the presence of NH, as evidenced by our identification of NH in 15% of 46 children in whom it was not clinically suspected. Our results mirror those of other studies that illustrate the insidious nature and subtle features of NH.2 3 NH can, however, be predicted by the presence of scoliosis and moderate PFT abnormalities, which should be considered warning signs. Patients who meet these criteria should be prioritised for polysomnography to evaluate their nocturnal respiratory parameters.
Our study is unique, as it evaluated an unselected paediatric population. Other studies evaluating the utility of PFTs as predictors of NH have largely been conducted in adult, symptomatic populations. It is therefore not surprising that we identified a higher threshold for an association between FVC and NH in an asymptomatic paediatric population. Hukins identified a cut-off of 40% predicted for FEV1, below which NH was predicted with adequate sensitivity (91%) and specificity (50%).4 Many of their subjects had elevated daytime carbon dioxide tension, however, indicating the presence of more severe respiratory impairment. Since this study identified isolated nocturnal respiratory impairment, it stands to reason that this was associated with a cut-off at a higher level of pulmonary function (FEV1 <65% predicted). Another study, in adults, evaluated inspiratory vital capacity (IVC), a surrogate marker for FVC and found that onset of sleep-disordered breathing occurred with IVC <60% predicted and NH occurred throughout the night with an IVC <40% predicted.32 Finally, a smaller prospective study of children with muscular dystrophies and lower baseline pulmonary function than our study participants found that IVC <40% correlated with the presence of NH.33
As in other studies,34 35 scoliosis was an independent cause of NH. It is therefore not surprising that children with both neuromuscular weakness and scoliosis are at increased risk of hypoventilation.
Many of the clinical parameters studied are inter-related. PFTs are decreased in the presence of scoliosis. Severe chest wall deformities increase as muscle weakness progresses, and make ambulation difficult, contributing to wheelchair use. Need for a wheelchair may imply greater muscle weakness, although in our study it did not predict NH. Obesity is also common in this population, particularly in non-ambulatory adults, and is an independent risk factor for NH. It did not, however, predict NH in our population, possibly due to the low prevalence of significant obesity. Statistical determination of the degree of relatedness of these variables was beyond the small sample size of the present study, but will be an important aspect of future investigations. Furthermore, respiratory muscle endurance likely contributes to respiratory reserve and therefore risk of NH. This is, however, difficult to measure.
This is the first study to document the natural history of disease over 1 year in children with progressive neuromuscular disease with and without NH. It highlights the importance of NH in perception of health status. It is encouraging to note that in our cohort, there was no progression to NH in those without it at study onset. The modest manual muscle strength decline demonstrates the slow rate of progression of muscle weakness in our cohort. Therefore it is not surprising that children did not develop NH over this time period, if NH occurs solely as a reflection of global deterioration in muscle function.
For children with neuromuscular disease, NPPV improves NH. It may also increase muscle strength, although this has not been clearly demonstrated. In our study and one other,14 neither maximal inspiratory nor expiratory muscle strength was changed, although the increasing gas trapping seen in our study suggests progressive weakness of expiratory muscles and inability to deform the chest wall below functional residual capacity.
This study's strengths include its prospective design, sampling children who were not previously suspected to have NH, representative of the Canadian population. This allowed us to study children earlier in the disease course. It may also explain why changes in lung volumes were not seen, whereas a decline in FVC and FEV1 over time periods less than 1 year has been shown in other studies evaluating adults36 and/or individuals who were more advanced in their neuromuscular disease at baseline.33
This study is limited, however, by the small number of participants, with heterogeneous neuromuscular conditions. Our study also did not employ the current standard definition of NH in children,37 as it was not yet published. The data were, however, subsequently reviewed using the current definition of hypoventilation in children37 and no re-classification of subjects would have occurred.
Long-term studies with larger numbers of individuals early in the disease process are required to elucidate the impact of NPPV treatment on the course of pulmonary function decline, muscle strength and endurance, quality of life and daytime functioning. Such information will be useful to clinicians in determining optimal timing for introduction of NPPV for NH.
Conclusion
NH has a high prevalence in children with progressive neuromuscular disease. Clinicians should be alert to risk factors and screen for NH in individuals with neuromuscular disease with FVC <70% predicted and/or FEV1 <65% predicted, especially in the presence of scoliosis. Children with NH appear to have more gas trapping and decline in muscle strength as compared with those with no NH. They perceive a worsening of general health status although other aspects of quality of life and attention are unchanged.
References
Footnotes
-
Funding The Hospital for Sick Children Foundation, CHEO Research Institute, Ontario Lung Association, Canadian Nurses Respiratory Society.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Children's Hospital of Eastern Ontario Research Ethics Board and Hospital for Sick Children Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.