Article Text

Abstract
The relation between different doses of vitamin K supplementation, several bone markers, and PIVKA-II concentrations in cystic fibrosis (CF) patients compared to controls was evaluated. Results suggest that a increased vitamin K intake may have significant health benefits for children with CF.
- cystic fibrosis
- vitamin K
- osteocalcin
- PIVKA-II
- bone status
Statistics from Altmetric.com
Cystic fibrosis (CF) is the most prevalent fatal, autosomal, recessive genetic disease in white people, affecting approximately 1 in 3400 live births.
Children with CF are at high risk for developing vitamin K deficiency because of fat malabsorption. The prevalence of vitamin K deficiency in CF is not precisely known, but it is common in unsupplemented patients with pancreatic insufficiency.1
Besides its function in blood clotting, accumulating evidence suggests that vitamin K plays a key role in improving bone health.1 Vitamin K is a cofactor in the post-translational γ-carboxylation of glutamic acid residues (Glu) to form γ-carboxyglutamic acid (Gla) residues which are able to bind calcium. Gla containing proteins are found in the clotting cascade (vitamin K dependent clotting factors) and in bone (osteocalcin). In the absence of vitamin K, Glu residues remain undercarboxylated, resulting in a strongly decreased affinity for calcium. Undercarboxylated coagulation factors are known as PIVKAs (protein induced by vitamin K absence); notably PIVKA-II (undercarboxylated prothrombin) serves as a sensitive marker for vitamin K status. Circulating undercarboxylated osteocalcin (u-OC) is considered to be an even more sensitive marker for vitamin K status than PIVKA-II concentrations.1 High serum u-OC concentrations are indicative of a poor bone status and are associated with low bone mineral density and increased risk of osteoporotic fractures.2,4
There is little consensus about the appropriate dose needed to prevent vitamin K deficiency in CF. Even in a large CF database (Dundee, UK) no indication can be found concerning the most appropriate dose of vitamin K to be used. Because vitamin K deficiency in CF patients may affect bone mineral status, associated complications may be prevented by adequate vitamin K supplementation.
SUBJECTS AND METHODS
In this uncontrolled study, 39 subjects were divided in four groups: 19 healthy subjects, 10 CF patients with no vitamin K (CFno), six CF patients with low dose vitamin K (<0.25 mg/day = CFlow), and four CF patients with high dose vitamin K (⩾1 mg/day = CFhigh) supplementation. Inclusion criteria for CF patients were pancreas insufficiency without liver function disturbances. Serum or urine concentrations of different bone markers and serum PIVKA-II concentrations were determined in healthy subjects and in and CF patients on different vitamin K supplementation. Serum concentrations of the bone formation markers osteocalcin (OC, total OC (t-OC), undercarboxylated OC (u-OC) and carboxylated OC (c-OC)) and bone alkaline phosphatase (BAP) as well as the bone resorption marker N-terminal collagen type 1 (NTX) were determined. The bone resorption marker deoxypyrodinoline (DPD) was determined in urine.
Data were analysed using the non-parametric Wilcoxon’s (Mann-Whitney) rank sum test (p<0.05 two sided).
RESULTS
Serum t-OC was measured in 10 controls only and was significantly higher in CFhigh patients (p = 0.016) than in controls (see fig 1). Serum u-OC was significantly lower in CFhigh patients than in controls (p = 0.005), CFno (p = 0.011), and CFlow patients (p = 0.033). Serum c-OC was significantly lower in CFno (p = 0.001) and CFlow patients (p = 0.011) than in controls, whereas c-OC was significantly higher in CFhigh patients than in CFno (p = 0.005) and CFlow patients (p = 0.010).

Boxplot showing total osteocalcin (t-OC in black), undercarboxylated osteocalcin (u-OC in grey), and carboxylated osteocalcin (c-OC in white) for vitamin K supplementation in CF patients, compared to healthy controls. Vitamin K supplementation is shown in three different groups: CFno = no supplementation; CFlow = <0.25 mg/day; and CFhigh = ⩾1 mg/day. Significant p values are shown.
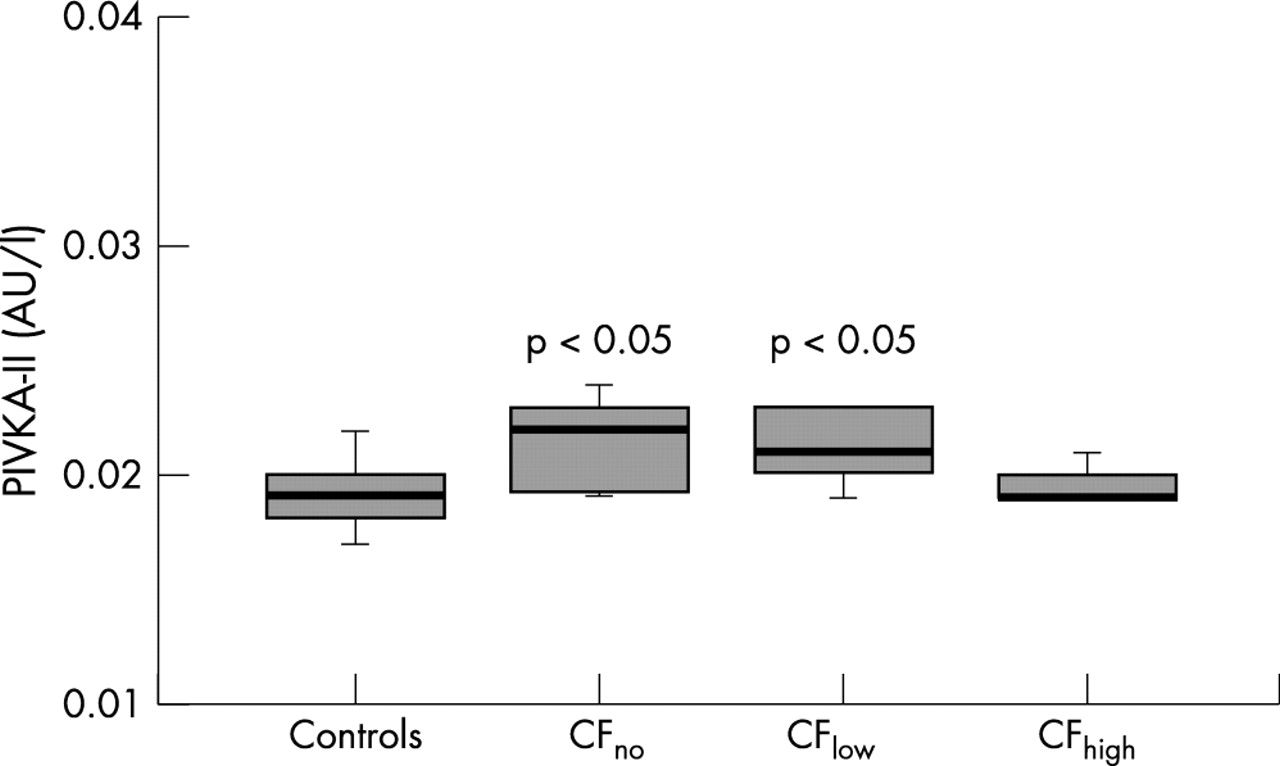
There was no significant difference in serum BAP and urinary DPD between the four groups. Serum NTX was significantly lower in CFno (p = 0.017) and CFlow patients (p = 0.020) than in controls. Serum PIVKA-II concentrations were significantly higher in CFno (p = 0.012) and CFlow patients (p = 0.022) than in controls (see fig 2).
{kind=link}
{kind=link}
Boxplot showing PIVKA-II concentrations in CF patients with three different doses of vitamin K supplementation, compared to healthy controls. Significant p values are shown.
DISCUSSION
High u-OC, low c-OC and raised PIVKA-II concentrations in all but CFhigh patients suggest a vitamin K dependent carboxylation defect in CF patients. In our study only CFhigh patients showed normal PIVKA-II concentrations suggesting that all other groups were vitamin K deficient to some degree. Hence only patients receiving a high dose (⩾1 mg/day) of vitamin K had an adequate vitamin K status. Several studies showed that vitamin K supplementation induced a decrease of serum u-OC and may alter other bone markers such as NTX and BAP.5–7 Our data showed a similar tendency, with the most prominent changes in the vitamin K-dependent osteocalcin. Whether the improved vitamin K status in CFhigh patients is associated with improved bone health still remains unclear. If vitamin K supplementation resulted in increased bone formation, both bone formation markers t-OC and BAP would be expected to be high in the CFhigh group, whereas this was only found to be the case for t-OC. Similarly, low bone resorption could be regarded as a beneficial effect. Again, our data are inconsistent, because NTX was significantly lower in the CFhigh group, whereas DPD was not. In conclusion, our results suggest that a high dose (⩾1 mg/day) vitamin K supplementation is needed to improve the vitamin K status of children with CF and to prevent potential vitamin K deficiency related complications. Long term (more than one year) randomised follow up studies are required to clarify the relation between vitamin K status and bone health in CF. This aspect will be of increasing importance as CF patients grow older and have a higher frequency of pathological fractures.2,4