Article Text

Abstract
Objective To compare the effectiveness of interventions aimed at reducing the rate of acute paediatric hospital admissions.
Design Systematic review.
Data sources Medline, Embase, PsychINFO, The Cochrane Library, Science Citation Index Expanded from inception to September 2010; hand searches of the reference lists of included papers and other review papers identified in the search.
Review methods Controlled trials were included. Articles were screened for inclusion independently by two reviewers. Data extraction and quality appraisal were performed by one reviewer and checked by a second with discrepancies resolved by discussion with a third if necessary.
Results Seven papers were included. There is some evidence to suggest that short stay units may reduce admission rates. However, there is a general lack of detail in the reporting of interventions and the methods used in their evaluation which precludes detailed interpretation and extrapolation of the results. The authors found no evidence that the use of algorithms and guidelines to manage the admission decision was effective in reducing acute admission rates. Furthermore, the authors were unable to locate any eligible papers reporting the effects on admission rates of admission decision by paediatric consultant, telephone triage by paediatric consultant or the establishment of next day emergency paediatric clinics.
Conclusion There is little published evidence upon which to base an optimal strategy for reducing paediatric admission rates. The evidence that does exist is subject to substantial bias. There is a pressing need for high quality, well conducted research to enable informed service change.
Statistics from Altmetric.com
Introduction
The number of children and young people admitted to hospital through emergency departments in England has risen by 6.8% over the last 3 years. In 2008/9, 15% of all patients requiring emergency admission in England were aged 0–16 years with a mean length of stay of 1.5 days, although significant variation exists between acute trusts for both these measures (the percentage of admissions ranging from 1% to 41% and mean length of stay varying between 0.1 and 4.4 days).1 The factors underlying the striking and continued rise in acute paediatric admission rates are not fully understood but are likely to be multi-factorial.2 3 Changes in the organisation of primary care in the UK have meant that unwell children are much less likely to be assessed out-of-hours by their own family doctor, and with their more limited knowledge of the family situation, emergency department and out-of-hours primary care clinicians may have a lower threshold for inpatient referral. Contributory factors may also include an increase in clinician caution stemming from a perceived increase in risk of legal claims,3 decreasing admission thresholds applied by less experienced junior doctors or an increase in parental expectation of admission.4 Changes in the definition of ‘hospital admission’ may also have played a part in the perceived rise in paediatric hospital admissions; funding initiatives providing financial incentives to classify ‘attenders’ at paediatric assessment units as ‘admissions’ may have artificially skewed the figures. While it is imperative that children receive the medical and surgical care they require, unnecessary hospital admission may be an undesirable process for children and their parents. It is possible that a proportion of acute hospital admissions could be prevented and/or reduced in length without compromising children's safety or the quality of their medical care.3 5 Given the regional variation that exists in the UK, there is clearly the potential for more efficient care in some organisations and this has been highlighted by the NHS Institute for Innovation and Improvement in their Emergency and Urgent Care Pathway for Children and Young People.1
What is already known on this topic
▶ The rate of paediatric hospital admissions continues to rise; this situation is generally considered unsustainable.
▶ A range of initiatives are being introduced to hospitals in the UK and beyond to reduce acute paediatric admissions.
▶ The relative effectiveness of initiatives to reduce inappropriate admissions while avoiding adverse consequences for the children discharged is unclear.
What this study adds
▶ There is little good quality published evidence to inform the most appropriate method for reducing paediatric admissions.
▶ Changes in the definition of ‘admission’ have hampered result interpretation; other outcome measures may be more useful in future evaluation of service re-design.
▶ Future service improvement should be implemented in such a way as to allow objective evaluation.
A range of initiatives to decrease acute hospital admission rates in the paediatric population have been attempted both in the UK and beyond. There has been increasing support for ‘acute assessment units’, both from the Royal College of Paediatrics and Child Health6 7 and from clinicians who believe this type of care can deliver a more timely service with better user satisfaction.8 Other initiatives have included consultant-level telephone triage services and the provision of rapid access out-patient appointments, both aimed at reducing the numbers of patients who present to the acute service. An increased emphasis on consultant-led care in acute settings7 and the introduction of evidence-based algorithms to guide management of common presenting symptoms (eg, diarrhoea and vomiting) have both been suggested to improve clinical decision making.9
A systematic review of hospital-based alternatives to acute paediatric admission published in 200510 concluded that acute paediatric assessment services are a safe, efficient and acceptable alternative to inpatient admission. Despite this, there appears to be no clear consensus on the most effective initiatives for reducing acute paediatric admissions. We therefore conducted a broader systematic review of the evidence for the effectiveness of initiatives introduced to reduce the rate of acute hospital admissions in children in order to assess the current evidence for acute assessment services and other interventions.
Methods
The systematic review was conducted following the general principles published by the NHS Centre for Reviews and Dissemination.11 A pre-defined protocol was developed following consultation with topic and methods experts and is available from the authors on request.
Literature search and eligibility criteria
The search strategy was constructed using a mixture of MeSH and free text words after consultation with experts in the field and examination of key papers. The master search strategy is shown in Box 1. Studies were identified by searching electronic databases, scanning reference lists of articles and consultation with experts in the field. No limits were applied for language and non-English language papers were translated. This search was applied to Medline/OVID SP (1950–Present), and adapted for Embase/OVID SP (1980–Present), PsychINFO/Ovid SP (1987–Present) and Science Citation Index Expanded/ISI Web of Science (1981–Present). The Cochrane Library database and the Database of Abstracts of Reviews of Effectiveness (DARE) were also searched. The main search was run on 23 September 2010 and updated on 5 August 2011.
Master search strategy
Ovid MEDLINE(R) <1950 to September week 2 2010> master search strategy, adapted for other databases
1 (Consultant* adj10 emergency).ti,ab. (204)
2 Consultant led service.ti,ab. (9)
3 (Consultant adj2 review).ti,ab. (30)
4 Medical Staff, Hospital/ec, sd (economics, supply & distribution) (1414)
5 Triage/mt (Methods) (1263)
6 (Triage adj2 (evaluat* or scale* or tool* or system* or consultant or telephone)).ti,ab. (1003)
7 (Consultant* and telephone referral*).ti,ab. (1)
8 Assessment unit*.ti,ab. (327)
9 (Ambulatory adj2 (unit* or assessment)).ti,ab. (486)
10 (Short-stay adj2 (ward* or observation or unit*)).ti,ab. (229)
11 (Rapid access adj2 (clinic* or unit*)).ti,ab. (55)
12 Day unit*.ti,ab. (164)
13 (Fast track adj2 (ward* or observation or unit* or clinic*)).ti,ab. (34)
14 (Acute adj2 (observation or unit* or clinic)).ti,ab. (1632)
15 (Emergency adj1 (ward* or observation or unit* or clinic*)).ti,ab. (2401)
16 (Guideline* adj2 (evaluat* or implement* or develop* or approach or assess*)).ti,ab. (8877)
17 Emergency Medicine/st (Standards) (1012)
18 (Checklist adj2 (evaluat* or implement* or develop* or approach or assess*)).ti,ab. (683)
19 (Algorithm adj2 (evaluat* or implement* or develop* or approach or assess*)).ti,ab. (4695)
20 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 (24041)
21 Child/(1186919)
22 Infant/(558554)
23 Adolescence/(1374082)
24 Exp infant, newborn/(441675)
25 Exp child, preschool/(656728)
26 21 or 22 or 23 or 24 or 25 (2478894)
27 (Child* or paediat* or pediat* or adolesc*).ti,ab. (925853)
28 26 or 27 (2625615)
29 (Accident adj emergency).ti,ab. (196)
30 ‘A&E’.ti,ab. (8528)
31 Emergency room.ti,ab. (8513)
32 Emergency department.ti,ab. (27071)
33 Exp Emergency Service, Hospital/(37096)
34 Exp Hospitals/(172396)
35 (Hospital adj3 (admission* or admit*)).ti,ab. (44873)
36 ((Doctor or GP or general practitioner) adj5 refer*).ti,ab. (1472)
37 (Emergency adj2 admission*).ti,ab. (1881)
38 Emergency care.ti,ab. (3838)
39 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 (274677)
40 28 and 39 (59690)
41 20 and 40 (1189)
Studies were included if they compared the effects on admission and/or readmission rates, patient or carer experience or cost of initiatives designed to reduce acute paediatric admissions with either simultaneously or historically collected control data. The initiatives considered suitable for inclusion were (A) paediatric consultant compared to junior doctor decision on admission; (B) telephone triage by paediatric consultant; (C) short stay in hospital beyond the 4 h wait in short stay units, observation units, ambulatory care units or assessment units; (D) algorithm-based management of the admission decision or clinical guideline driven care at admission; and (E) next day emergency paediatric clinics (which may also be known as fast track clinics or rapid access clinics). Interventions had to be described in sufficient detail to enable replication and involve children between 0 and 19 years of age. Studies reported as conference proceedings were included if there were sufficient data to assess the risk of bias. Authors were contacted to supply missing data where necessary. No language restrictions were applied.
Two reviewers (KB and JTC) independently screened titles, abstracts and full texts and applied the inclusion and exclusion criteria. For potentially relevant references the same procedure was performed for the full text articles (KB, JTC, AM and AA). Any discrepancies were resolved through discussion with a third reviewer (KB, JTC, AM and AA).
Data collection
Data on study design, intervention, participant characteristics, relevant outcomes and risk of bias were independently extracted by one reviewer (AA or AM) and checked by a second (either AM, AA or JTC) using a standardised, piloted data extraction form.
Risk of bias
The methodological quality of each included paper and thus the risk of bias in the reported results was assessed by one reviewer and the judgements were checked by a second with discussion to achieve consensus. We used a bespoke checklist based on both the Quality Checklist for Healthcare Intervention Studies, developed by Downs and Black,12 and the Cochrane Effective Practice and Organisation of Care (EPOC) Group data collection list.13
Data synthesis
Due to the paucity of studies eligible for inclusion, the heterogeneity of the study design, population and outcome measures used and the risk of bias in the identified studies, no formal statistical synthesis was performed. The results of the included studies have been tabulated and evaluated in a narrative format to provide a detailed summary of the identified evidence.
Results
Study characteristics
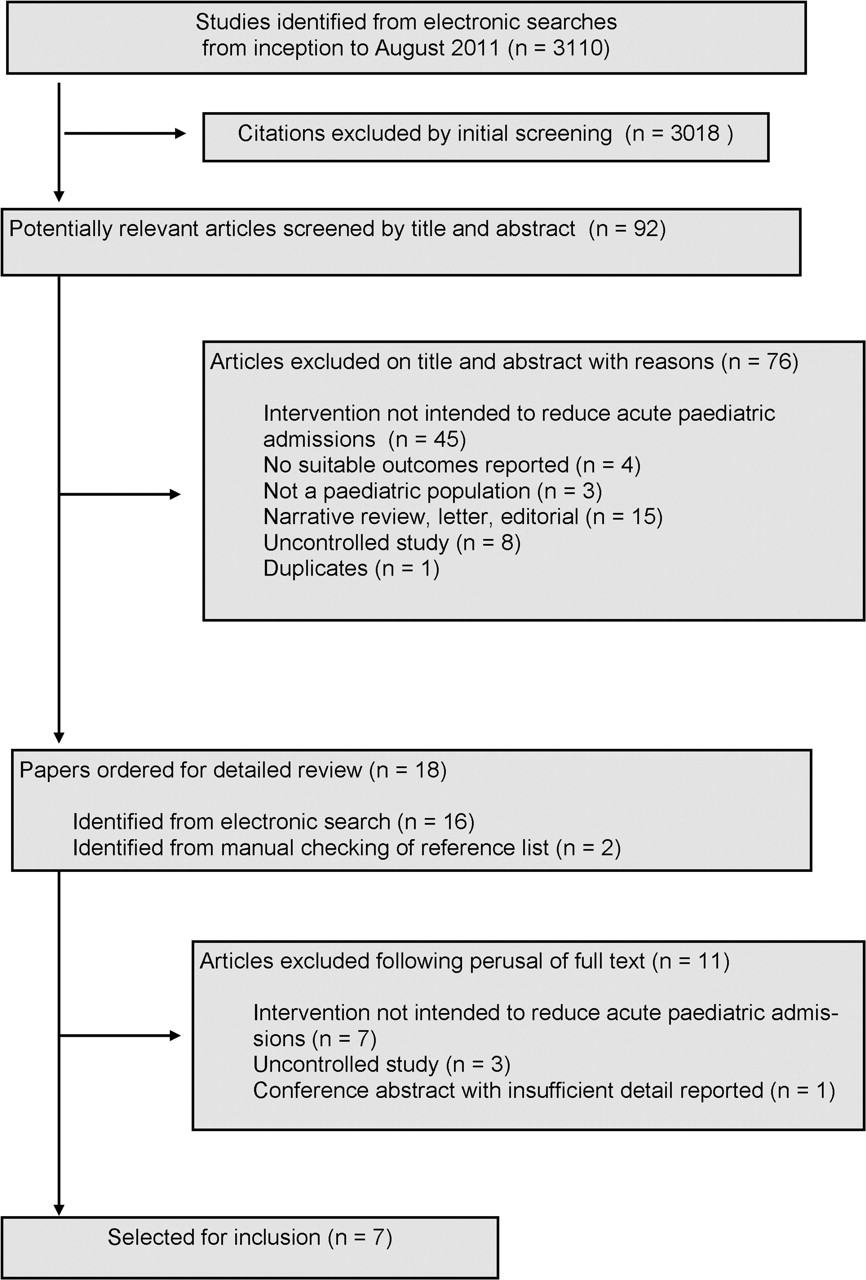
The initial search produced a total of 2719 results, of which 739 were duplicates and 1980 were excluded following examination of the title and abstract. Full texts of the remaining 88 papers were retrieved for closer examination. Eighty-two papers were excluded (intervention not designed to reduce acute paediatric admissions n=48; non-systematic review, letter or editorial n=15; uncontrolled study n=10; no relevant outcome measures n=4; not a paediatric population n=3; duplicate publication n=1; full text unobtainable n=1; and results available only as a conference abstract with insufficient detail available to assess study design or risk of bias n=1) on perusal of the full text and of the bibliographies of included papers and reviews identified during the search, leaving seven studies for inclusion in the review (figure 1).14,–,20 The updated search produced 391 additional results; the full text of four of these articles was retrieved for closer examination, but none were deemed to meet the inclusion criteria (intervention not designed to reduce paediatric admissions). Five papers were published in English, one was translated from Spanish17 and one from French.18
{kind=link}
Flow chart of study selection process.
In four papers, the effects of the introduction of a short stay facility on admission rates are reported,14 18,–,20 while the remaining three papers are concerned with guideline-based admission policies in various conditions (diarrhoea,15 seizures,15 gastroenteritis16 and asthma).17 We were unable to identify any eligible papers in which the effects of paediatric consultant decision on admission, telephone triage by paediatric consultant or next day emergency paediatric clinics on admission rates were studied. Six studies, using various non-randomised designs, report quantitative data15,–,20 and one reports qualitative data of the views of parents, staff and referrers.14 Characteristics of the included studies and study participants are shown in tables 1 and 2. Sample size ranged from 60 in the qualitative study14 to 8287 in a large, historically controlled trial of the use of a guideline for the management of acute gastroenteritis.16 Indicators of study quality are shown in table 2. There is a general lack of detail in the reporting of the process of selection for inclusion in each study, the completeness of the dataset, the patient characteristics at baseline and any adjustment for confounders. Two of the studies reported a sample size calculation.15 16 Data were collected prospectively postintervention in five of the studies but are compared with historical control data collected retrospectively in two of these studies.16 17 19 20 Data were collected entirely retrospectively in two studies.19 20 A clear strength of all the studies is the use of an objective primary outcome measure (‘admission’ rate), but the influence of additional factors over the course of the data collection periods (eg, changes in health service delivery and staffing, changes in methods of record keeping and disease definitions, changes in the definition of ‘admission’, varying levels of illness in the community, underlying trends in admissions patterns and changes in prescription practices or guidelines) on the effects of the intervention is unknown.
Characteristics of included studies
Indicators of study quality
Algorithms and guidelines used to manage the admission decision
Three studies compared admissions to hospital prior to the implementation of an evidence-based guideline with those recorded while the guideline was in use in asthma17, seizures15 and diarrhoea or gastroenteritis.15 16 Results of the studies are shown in tables 3 and 4. There were no statistically significant differences in admission rates between data collection periods in any of the studies.
Algorithms and guidelines used to manage the admission decision: summary of results
Short stay units: summary of results
Short stay units
One paper reported quantitative results of the comparison between admission rates to a hospital with a short stay unit and those to a hospital without this facility.18 Martinot and colleagues18 compared a short stay unit in a tertiary paediatric hospital with six small local hospitals with no short stay unit and no resident paediatrician. Both sets of data were collected prospectively over the same time period and the results showed clinically and statistically significant lower admission rates in the hospital with the short stay unit than in the general hospitals (77% of children presenting with acute gastroenteritis in the general hospitals versus 42% in the short stay unit; RR of admission 0.55; 95% CI 0.49 to 0.62, p<0.000001). The length of stay was also shorter in the hospital with the short stay unit (0.8 days versus 2.4 days in the general hospitals; no statistical analysis reported). The results of this study should be treated with some caution since there are likely to be many differences between the comparison groups in addition to the presence of a short stay unit.
Two papers reported admission rates before and after the introduction of a short stay unit.19 20 Gouin and colleagues19 reported a statistically significant reduction in admission rates in children with asthma following the opening of an observation unit in a tertiary paediatric hospital (31% admitted for an overnight stay in the year prior to the opening of the unit versus 24% in the year after; RR of admission 0.91; 95% CI 0.88 to 0.94, p<0.01). There was also a reduction in the number of children with asthma hospitalised for less than 24 h (17% before versus 10% after; p<0.1). Although the data collected after the implementation of the observation unit showed a slight increase in the re-attendance rate within 72 h of discharge (3.2% before versus 5.0% after, p<0.1), only 24 of the 85 repeat visits in the postobservation unit group required hospital admission (28%), compared with 17 of the 44 repeat visits in the preobservation unit group (39%) (RR of re-attendance 0.62; 95% CI 0.43 to 0.89). The authors acknowledge that there were several other important changes occurring over the same time period which may have influenced the result. These included the attitude of the physicians, the progression of medical knowledge in asthma treatments, the development of local practice guidelines and cost cutting initiatives within the institution. A fall in admission rates in children with respiratory symptoms, gastroenteritis and fever in the year following the opening of a day assessment unit at a hospital in the UK was also documented by Meates in 1997.20 No statistical analyses were performed. There is very little reported detail of the methods used in this study or of the baseline characteristics of the study participants.
In a service evaluation, Blair and colleagues employed quantitative and qualitative techniques to assess the impact of a new paediatric ambulatory unit in the UK.14 Parental perceptions were assessed with a questionnaire which was offered to 148 of 455 eligible respondents with a 70% response rate (n=104). Almost all those surveyed were satisfied with the service and preferred it to traditional A&E services. However, parents were not offered the questionnaire during busy periods. Comparative data for this part of the study were obtained from parents attending A&E during the night when the new unit was closed and may not provide a representative sample. Interviews with staff and referrers found that the ambulatory unit was perceived to be a ‘superior’ model to A&E but that improvements were required around appropriate referrals and the need for more multi-disciplinary protocols and liaison.
Discussion
The rate of hospital admissions among the paediatric population continues to rise and there is widespread recognition that this situation is unsustainable. A range of initiatives are being introduced to hospitals in the UK and beyond to reduce acute paediatric admissions. It is unclear which of these might be most effective at reducing inappropriate admissions while avoiding adverse consequences for the children who are discharged. The aim of this review was to synthesise the available evidence to better inform decision making when planning service improvement. Despite conducting a widespread search for possible data in a variety of sources, we were unable to identify good quality comparative data on any of the relevant initiatives. All of the studies included in the review are open to significant potential bias. There is a general lack of detail in reporting fundamental aspects of the research including the criteria for admission and discharge, the influence of possible confounding factors over the data collection period, the characteristics of the patients included and the completeness of the dataset. There are also issues with the use of terminology surrounding the care pathway in different settings (eg, are children ‘admitted’ to a short stay unit?) which complicate the interpretation of data. All these factors hinder the extrapolation of data from individual studies to draw overall conclusions as to the effectiveness of any of the included initiatives. From the data identified, it is also difficult to establish how effective the initiatives are in the wider context of the healthcare system. Overnight admissions may be reduced, but if this results in an increase in resource intensive short stay admissions the overall economic impact may not be cost-saving.
We have reported all the available data from the studies included in the review. While all the studies reported ‘admission’ rates, it is unclear whether the same definition of ‘admission’ is used in each study. Changes in the definition of ‘hospital admission’ over time may have been driven by different funding mechanisms and, of course, may differ between different countries. More revealing outcome measures might be ‘length of stay’, ‘rate of re-admission’, ‘consequences of non-admission’ or ‘resource use’. These were not widely reported in the included studies but should be considered when evaluating and reporting future service re-design. It is also important to note that while admission rates are one indicator of efficiency, there are other potential markers of improvements in service which may improve quality or address staffing issues but which may not impact on admission rates.
A previous systematic review published in 2005 by Ogilvie10 used less restrictive eligibility criteria and hence included a wide range of evidence from a variety of study designs including surveys and descriptions of current practice, some of which included comparative data. Ogilvie concluded that “the current evidence supports a view that acute paediatric assessment services are a safe, efficient and acceptable alternative to inpatient admission, but this evidence is of limited quantity and quality”. We felt that for our review to add to existing knowledge and to be useful to policy and decision makers, the intervention should be sufficiently well defined to enable replication. We also included only studies in which the effects of the intervention on admission rates could be compared with data (collected either simultaneously or historically) from a setting in which no initiative was employed, in order that the effects of the intervention could be demonstrated. It is disappointing that following the publication of the review by Ogilvie10 and with the increased interest in and implementation of acute paediatric assessment units, we were unable to identify any good quality reports in this area to supplement the previous review. Previous commentators over the past decade have stressed the need for institutions setting up new short stay units to publish clear results in terms of the effects on costs and benefits.10 20 21 It is imperative that future service improvement is implemented in such a way as to allow objective evaluation.
There is evidence to suggest that a handful of common presentations account for most medical paediatric emergency attendances. In a recent retrospective review of electronic patient records from a UK emergency department, Sands and colleagues22 found that the 10 most common presenting problems accounted for 85% of medical attendees, with just under 50% the result of either fever (14%), breathing difficulty (20%) or diarrhoea (14%). These diagnoses are most common in the very young and show seasonal variations. It has been suggested that the use of evidence-based guidelines or algorithms to manage the admission decision in these common conditions may help to reduce admissions. We were unable to find any convincing evidence to support these suggestions.
Conclusions
Admission rates for children to hospital continue to rise. Despite the widespread professional support for the introduction of acute assessment units, there is little published evidence to inform the most appropriate method for reducing admission and the evidence that does exist is of poor methodological quality and subject to substantial bias. There is a need for high quality, well conducted research in which more appropriate outcome measures are reported to enable informed service change. Any future service improvement should be implemented in such a way as to allow objective evaluation.
Acknowledgments
The authors wish to thank Oriana Ciani and Emilie Heintz for invaluable assistance with translation and Morwenna Rogers for help with document retrieval.
References
Footnotes
-
Funding This systematic review was funded by the National Institute for Health Research through PenCLAHRC. This review presents independent research commissioned by the National Institute for Health Research (NIHR). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.