Article Text

Abstract
BACKGROUND Osteoporosis has been reported as a complication of cystic fibrosis (CF).
AIMS To measure bone mineral density (BMD) in non-acutely ill adults and bone mineral content (BMC) in children with CF.
METHODS We analysed data from 28 adults and 13 children with CF. Corticosteroid use was minimal for the year prior to study in both groups. Dual xray absorptiometry was used to measure total body and regional bone mineral density in adults. In children, whole body BMC was measured. Lean tissue mass (LTM) was also measured in all subjects. There were two control groups: A (matched for LTM and height, in addition to age and gender); and B (matched for age and gender only).
RESULTS There was no difference in whole body or regional BMD density between adult CF patients and control A subjects. Both whole body and regional BMD were significantly lower in adult CF patients than in control B subjects. Total body BMD was correlated with body mass index, LTM, and percent fat in both CF and control subjects. There was no significant correlation between total body BMD or regional BMD and either NIH clinical status scores, or pulmonary function tests in adults. There was no difference in total body BMC between CF children and control A subjects. Total body BMC was significantly lower in CF children than in control B subjects. There was no correlation between pulmonary function results and BMC in children.
CONCLUSION Osteopenia and osteoporosis in CF may be caused more by malnutrition and chronic use of intravenous or oral corticosteroids than by a CF related inherent defect in BMD. Appropriate “normal” data should be selected when determining whether or not osteoporosis is present in a CF patient.
- osteoporosis
- osteopenia
- bone mineral density
- cystic fibrosis
Statistics from Altmetric.com
Cystic fibrosis (CF) is the most common inherited genetic disorder and is caused by the mutation of cystic fibrosis transmembrane regulator (CFTR). It occurs in approximately one of every 2500 live births in the white population,1 and leads to death or lung transplantation in more than 500 patients annually in the United States.2 Recent medical advances have increased the life span of CF patients, and survival to adulthood is common. Unfortunately adults with this disorder often face many long term complications including diabetes, liver disease, and infertility. Osteoporosis3-6 and osteopenia3 ,4 ,7 ,8have also been reported as common complications of CF.
Osteoporosis can be defined as bone mineral density (BMD) more than 2.5 standard deviations below the mean for age and sex matched normal values; and osteopenia is generally defined as BMD between one and 2.5 standard deviations below the mean for age and sex matched normal values.9 ,10 Cystic fibrosis patients have many known risk factors for the development of osteoporosis, including inadequate dietary intake, inactivity, and glucocorticoid use. Another risk factor for osteoporosis could be inadequate concentrations of sex steroids. Several studies have documented delayed pubertal maturation in CF,11 ,12 and one study described lower concentrations of sex steroids in males.13 Furthermore, in 1979 Hahnet al described osteoporosis in CF secondary to malabsorption of calcium and altered vitamin D metabolism.4
Although previous studies have reported the presence of significant osteopenia or osteoporosis in CF patients, it is unclear whether or not osteoporosis is present in the majority of CF patients. Several previous studies5-7 report data from CF subjects who had poor clinical status; and some previous studies3 ,4 ,9have included CF subjects taking oral or intravenous corticosteroids. The first goal of our study was to determine if osteopenia and osteoporosis were present in CF patients who were not chronically treated with oral or intravenous corticosteroids, and who were, in general, clinically stable.
Several studies6 ,7 have compared BMD in adult CF patients to age and gender matched reference data provided by the maker of the dual x ray absorptiometry (DXA) scanner. Although other studies have specifically recruited healthy volunteers as controls for comparison with the CF subjects, these control subjects were matched only for gender and age.4 ,8-10 Bone mineral density has been clearly linked to body size, including height14; we therefore wished to compare BMD values from CF subjects to data from control volunteers specifically matched for height and lean tissue mass (LTM), in addition to age, gender, and ethnicity.
Methods
SUBJECTS
Adults
We analysed DXA data from 28 adult CF subjects (table 1) who had previously participated in our studies of carbohydrate metabolism.15-17 None had been acutely ill for at least four weeks and had not taken oral or intravenous steroids for at least four months. Many patients, however, used low doses of inhaled corticosteroids. All patients had undergone measurement of glucose tolerance by an oral glucose tolerance test and had been classified as having normal glucose tolerance, impaired glucose tolerance, or diabetes. Pulmonary function and overall clinical status ranged from poor to excellent; however, the majority of subjects had moderately good pulmonary function.15 Patients were excluded from participation if they were colonized withBurkholderia cepacia, had liver disease, or were pregnant. All CF patients required replacement of pancreatic enzymes (pancreatic exocrine insufficient).
Clinical characteristics of adults with CF
We compared the data in our CF subjects to data from 17 normal healthy adults who were recruited as control volunteers for our previous studies.15-17 Their BMD data were used for this study and they are referred to as control A subjects. These volunteers were matched to the CF patients for height, LTM, and ethnicity, as well as age and gender. Control volunteers were screened by history, and physical and laboratory examination to exclude for chronic illness and/or eating disorders. All were judged to be in normal health. All subjects gave written informed consent as approved by the Institutional Review Boards at the University of Texas Health Science Center and Baylor College of Medicine, Houston.
A second set of controls (control B) for the adults was obtained from the reference data maintained by the manufacturer of the DXA instrument (Hologic, Waltham, Massachusetts). This data bank includes DXA information for 7116 healthy men and women of all races, aged 20 years or above, and all in normal health. The data are categorised by age, gender, and ethnicity. Specific data used for comparison for our population included data from normal white subjects in the age range 20–34 years. To compare data for the hip, Hologic provided information from 437 females and 461 males; and for spine data, 116 females and 128 males. Data for control B subjects were matched for age and gender, but not for LTM or height. Whole body BMD was available only for females.
Children
We also reviewed DXA data from 13 prepubertal children with CF (eight boys, five girls) who were recruited for studies of pancreatic function (see table 2). All subjects were normally glucose tolerant. Tanner staging was performed in all children by the paediatric endocrinologist (DSH). In children, inclusion criteria were: no acute illness for a minimum of four weeks, and no oral or intravenous corticosteroids for a minimum of two months prior to study. Specific pulmonary function was not a recruitment criterion and ranged from moderate to good. Control data for the paediatric subjects were obtained from data collected in over 1200 healthy children and maintained locally at the Children's Nutrition Research Center.18 ,19 These healthy children were within two standard deviations of weight and height (NCHS charts) and were judged to be clinically free from disease by both history and physical examination. Further description has been previously published.18 ,19 In the age range 8–12 years, 256 girls and 192 boys were available for reference. In keeping with our two control groups for adults, control A subjects were matched for height, LTM, age, and gender. Control B subjects were matched only for age and gender.
Clinical characteristics of children with CF
DUAL x RAY ABSORPTIOMETRY
In adult and paediatric subjects, LTM, fat mass, bone mineral content (BMC), and BMD were measured by the DXA Hologic QDR 2000 instrument with standard density software (version 5.56; Hologic Inc., Waltham, Massachusetts). The total body measurements require 8–15 minutes; the error is <1% for BMC and BMD, <2% for LTM, and 2–5% for body fat mass.20 Regional (lumbar spine, right femur neck, and trochanter) BMD measurements were obtained in adults. In children, only whole body measurements were analysed. In children, BMC was reported instead of BMD. Although no consensus exists regarding the best measure of osteopenia/osteoporosis in children, BMC takes into account the age related increase in bone thickness and has been reported21 to be the superior measure in children. Using DXA we also obtained data for LTM, fat, and percentage fat.
DETERMINATION OF CF CLINICAL STATUS AND ANTHROPOMETRIC DATA
For the adult CF subjects, we assessed clinical status using a modified National Institutes of Health Score,22 which is based on pulmonary complications and general complications. Pulmonary function, specifically forced vital capacity (FVC) and forced expiratory volume (FEV1), are included as part of the pulmonary complications section of the NIH status score. In children with CF, FEV1 and FVC were the only measure of clinical status obtained. Pulmonary function and all clinical status score data were gathered within two weeks of the DXA scan. Correlation between measures of BMC or BMD, and the clinical status score and/or the pulmonary function data, was assessed for each CF patient. Anthropometric data for both adults and children were measured by a research nurse at the University of Texas Clinical Research Center using a wall mounted stadiometer and a single scale. Both instruments of measurement undergo quality control assessment twice a week.
MEASUREMENT OF SEX STEROIDS
Oestradiol and oestrogen concentrations were measured in serum obtained from all female subjects by Endocrine Sciences Laboratory (Calabasas Hills, California). Total serum testosterone was measured in all male subjects by radioimmunoassay (Testosterone 4100, Diagnostic Systems Laboratories, Webster, Texas).
STATISTICAL ANALYSIS
Results are reported as mean (SD) for each group. Student'st test was used for calculating significant differences between CF and control groups. Pearson scores were used to determine correlation analysis between BMD and various clinical variables. Statistical significance was defined as p < 0.05.
Results
ADULTS
Total body BMD was significantly lower in female CF subjects than in control B subjects (total body BMD results for control B subjects were available only in females). There was no difference in total body BMD between CF subjects and control A subjects (matched for LBM and height). Figure 1 depicts data from the female subjects. The Z score for the total body BMD in CF was −0.951, or 91.8%, when compared to reference data provided by Hologic (approximately 8% below the average).
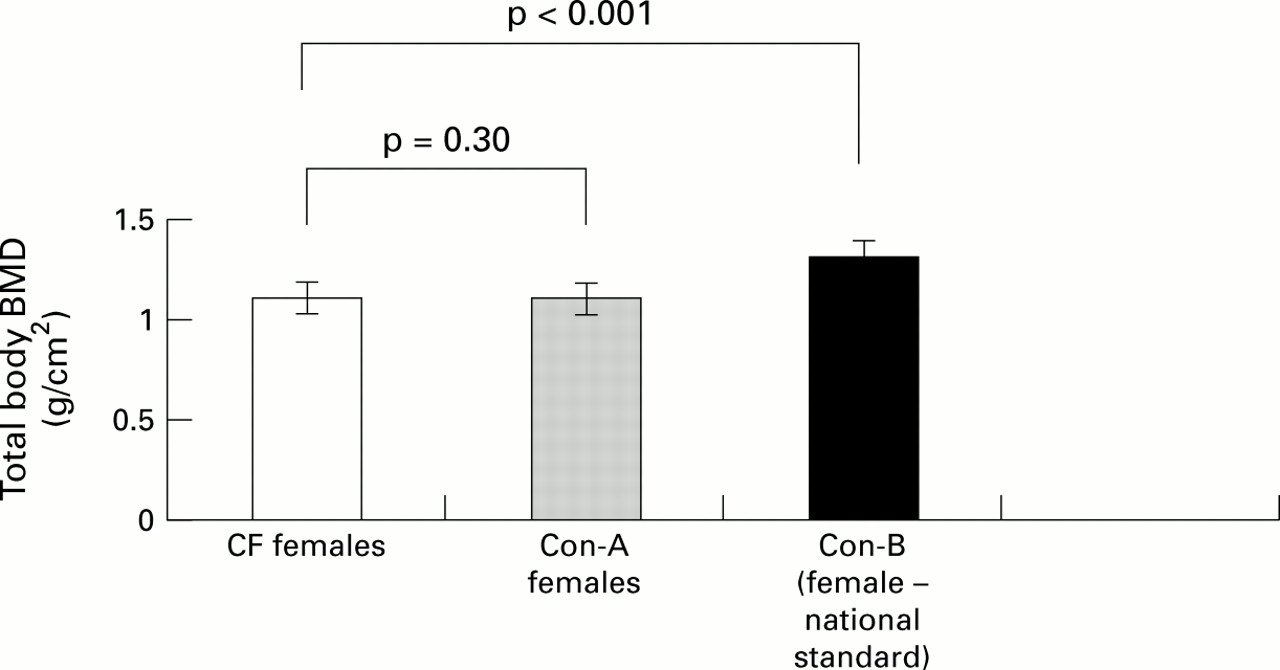
Total body BMD in adult CF, control A, and control B females.
Regional BMD data were available for control B subjects of both genders. There was no difference in regional BMD (spine, trochanter, and femur neck) between CF and control A subjects, but BMD was significantly lower in CF subjects compared to control B subjects (table 3). In both CF and control A adults, total body BMD was correlated with body mass index (r = 0.9, p = 0.01), LTM (r = 0.85, p < 0.001), and percentage fat (r = 0.8, p = 0.06). Figure 2 shows the correlation between BMD and LTM. There was no statistically significant correlation between either total body or regional BMD and the NIH clinical status scores, or between BMD and FEV1 or FVC values.
Regional BMD in CF adults and controls

Correlation between BMD and LTM in adult CF subjects.
To qualify for study participation, none of our subjects had used oral or intravenous corticosteroids for at least four months prior to study. Review of each subject's chart for the preceding year revealed that no patient had received intravenous corticosteroids. Table 4 documents oral and inhaled corticosteroid use. There was no difference in BMD at any site when subjects were grouped according to the route of corticosteroid inhalation (intranasal versus oral inhalation). The three subjects who had been treated with oral corticosteroids during the previous year tended to have worse clinical status (average clinical status = 74; average in the three on steroids = 68). They also tended to have lower total body BMD (mean = 21.8 kg; mean in the three on steroids = 20.3 kg). Glucose tolerance showed no relation with BMD in these subjects.
Oral and inhaled corticosteroid use in CF subjects by gender
All adult CF subjects were fully sexually mature; females reported normal menstrual cycles. Most CF females denied using exogenous forms of birth control. Three CF women reported use of an oral contraceptive agent, and one had received a single injection of Depot Provera 2.5 months prior to study. Oestradiol concentrations were similar in control and CF females and were consistent with follicular phase (7.6 (4) ng/ml in controls, 5.7 (6) ng/ml in CF subjects; NS). Total serum oestrogens were also similar between controls and CF subjects and were consistent with follicular phase (9 (4) ng/dl in controls, 7 (3) ng/dl in CF subjects; NS).
All males reported normal sexual function. Additionally, there was no difference between testosterone concentrations in CF men and controls, and the results were within the reported normal range for both subgroups (4.0 (1) ng/ml in controls, 3.5 (0.9) ng/ml in CF subjects; NS).
CHILDREN
There was no difference in total body BMC between CF children and control children when matched for LTM and height, in addition to gender and age (0.92 (0.17) kg in CF subjects, 1.04 (0.27) kg in control A subjects; p = 0.31). However, when compared to control B subjects (matched only for age and gender), total body BMC of CF children was significantly lower (fig 3). Regional BMD and BMC measurements were not obtained in CF children. There was no correlation between BMD values and pulmonary function test results in children with CF. All children were normally glucose tolerant; we were therefore unable to evaluate possible relations between glucose tolerance and BMC in these subjects.

{kind=link}
{kind=link}
{kind=link}
Total body BMC in children with CF and control A and B subjects.
Review of each child's medical record for one year prior to study participation revealed no previous use of intravenous corticosteroids. With the exception of one subject, the paediatric CF subjects did not receive oral corticosteroids for at least four months before the study. This child was treated with a short course of oral corticosteroids 2.5 months before study participation, and had average BMC. Table 4documents use of oral and inhaled corticosteroids. There was no correlation between BMC and inhaled corticosteroids given either intranasally or by oral inhalation.
Discussion
Our study shows that whole body BMD of CF subjects who are not acutely ill, and who are not chronically using systemic corticosteriod medications, is similar to that of healthy control subjects when the groups are matched for LTM and height, in addition to age and gender. These findings do not support the general concept that all CF patients have osteopenia/osteoporosis.
Our finding of normal BMD/BMC in CF does not support reports from several previous groups5-7 ,23 ,24; however, there are several subject selection criterion used in our study which we believe account for our findings. Firstly, we have conducted this analysis in a cohort of patients who clearly were not using systemic corticosteroids on a routine basis. Several previous studies have included patients with “significant exposure” to steroids,5 or unspecified steroid use.6 ,24 For example, Shane and colleagues5 reported decreased BMD compared to the national standard in 11 adult CF patients awaiting lung transplantation. This group also found similarly low BMD in patients with chronic obstructive pulmonary disease who were treated with corticosteroids, but found normal BMD in non-steroid treated patients. Our study is the first to definitively quantify low steroid use in the subjects and clearly suggests that CF patients with low use of corticosteroids are less likely to have osteopenia/osteoporosis.
A second difference between our study and those of others is that our subjects, in general, had good clinical status. Previous studies6 ,7 have been conducted in adult patients who were probably more ill (for example, awaiting lung transplantation) than our subjects. Poor clinical status increases the risk of osteopenia/osteoporosis.6 Only a small number of subjects with either excellent or poor clinical status participated in this study; thus, the lack of correlation between NIH clinical status scores and relative BMD data may have been a result of small scatter with resultant inability to detect such a correlation. Another indicator of our subjects' good clinical status is their percentage ideal body weight. Previous studies have included poorly nourished patients. For example, Rochat and colleagues7 reported very low BMD in seven malnourished subjects, but normal BMD in three normally nourished CF subjects. Studies by Gibbens and colleagues6 and Henderson and Specter24 have reported the relation between nutritional status and osteopenia in children. Malnutrition has been clearly linked to worsened clinical status; therefore it is not surprising that CF patients with poor nutritional status would have decreased BMD. Poorly nourished patients are also less likely to be active, and more often receive systemic steroid therapy. Our finding of normal bone mineralisation in our normally nourished subjects supports this relation.
Delayed puberty and hypogonadism have been reported in CF. Both of these conditions may impair bone mineral accretion and/or accelerate bone loss.13 ,19 Puberty often occurs late in CF, and one group13 reported lower salivary testosterone concentrations in CF men. In women, ovarian function is dependent on maintenance of a minimum body weight, and in conditions associated with poor nutrition, such as CF and anorexia nervosa, hypogonadism may be a major contributor to bone loss. All adult female subjects in our study reported normal menstrual function and had normal concentrations of oestradiol and oestrogen. Adult males reported no erectile dysfunction and had normal testosterone concentrations. Thus our subjects would not be expected to have decreased BMD related to low concentrations of sex steroids.
Perhaps the most significant difference between our study and reports by others is our use of two control groups: one matched for lean tissue mass (LTM) and height, in addition to age and gender; and a second group, matched only for age and gender. We believe the additional criterion for matching the control group is important for the evaluation of bone mineralisation for both adults and children with chronic illness. BMD, defined as BMC divided by bone area, was initially developed to compare bone mineral data among healthy adults whose bone area does not change substantially over time. In adults with chronic disease, both BMC and bone area can change dramatically. In children, both linear and appositional growth occurs, and both the timing and rate of growth at different bone regions can change quickly. Thus, both BMC and bone area change during longitudinal studies, and their rates of change are not necessarily coupled. Furthermore, the use of bone area to normalise BMC is questionable on statistical grounds. BMC and bone area are not independently derived. The estimate for LTM is based chiefly on an independent set of pixels in the DXA scan. Height is also an independent measure of skeletal growth. The correlation between BMC and LTM, and BMC and height has been described previously.19 ,22 Thus, inclusion of height and LTM accounts for the variation in BMC observed in the general healthy population.
Previous studies reporting osteopenia/osteoporosis in CF have not accounted for both LTM and height; therefore it is likely that these findings could be related to the larger body size of the controls. For example, Bachrach and colleagues25 reported osteoporosis of the lumbar spine, femur neck, and whole body bone sites in 22 adult CF patients. However, their control subjects were significantly taller and heavier than the CF subjects. Rochat and colleagues7also reported lower BMD in CF adults; however, they corrected the data for height, but not for LTM. Bhudhikanok and colleagues3found both low, and normal, bone mineralisation in CF adults and children. They reported that risks for osteopenia include: low body weight, hypogonadism, and use of corticosteroids. Although they matched controls only for gender and age, data were reported as bone mineral apparent density, in order to estimate volumetric bone mass. Estimates of bone mineral apparent density do not necessarily correct for differences in BMC related to LTM, and this adjustment is difficult to apply to total body BMC data. Our findings, and those of others,6 ,7 ,26 suggest that correction of data for LTM may be important, especially when interpreting data in people who are small.
BMD is influenced by bone size14 and may underestimate the bone mineral properties in smaller individuals,27 ,28 such as CF patients. We have found no difference in BMD in CF subjects when their data were compared to data from controls matched for LTM and height. Perhaps a more provocative question is whether or not our control subjects have decreased BMD, and therefore are at increased risk for fracture. Certainly when compared to gender and age matched national averages, our controls also have decreased BMD. However, as BMD is clearly linked to height and LTM, it seems more likely that our controls are simply smaller people with appropriately less BMD (compared to the usual DXA control group matched only for gender and age). We know of no longitudinal studies comparing risk for fracture in normal healthy young adults or children who appear to have lower BMD simply secondary to small body size. Studies in this area would be useful. We should also note that matching subjects for both LTM and height is certainly not conventional and requires additional study to determine general utility.
The only other study comparing BMD in CF subjects to controls who were also matched for LTM, was reported by Salamoni and colleagues.26 This group studied 14 CF patients aged 6–20 years, and found no difference in BMD, or in vitamin D metabolism in CF. It is important to note that the CF subjects in the study of Salamoni et al were not malnourished and were not using corticosteroids. These findings are similar to the findings of our current study; however, our subject number is larger.
In summary, our study has found no difference in BMD in CF adults, or BMC in CF children at any bone site when compared to controls matched for height and LTM, in addition to age and gender. It is important, however, to emphasise that our subjects had very little exposure to systemic corticosteroids and in general had good clinical status. Osteoporosis undoubtedly occurs in CF; however, it is propably related to chronic use of systemic corticosteroids, chronic malnutrition, and poor clinical status. Our findings do not support the uniform diagnosis of osteoporosis in CF and suggest that risk for osteoporosis should be assessed for each patient. Osteoporosis appears to be yet another area indicating the importance of improving the clinical and nutritional status of our patients with cystic fibrosis.
Acknowledgments
We thank Drs Patrick Brosnan for review of the manuscript and Albert C Hergenroeder for review of the sex steroid data. This study was supported by the following grants: National Institutes of Health: 1 K08 DK02365-01 (DSH) and MO1-RR-02558 (The Clinical Research Center at University of Texas), a grant from the National Cystic Fibrosis Foundation (DSH), and the United States Department of Agriculture Agreement 58-6250-1-003 (KJE).