Article Text

Abstract
Introduction Patients who survive an intensive care unit admission frequently suffer physical and psychological morbidity for many months after discharge. Current rehabilitation pathways are often fragmented and little is known about the optimum method of promoting recovery. Many patients suffer reduced quality of life.
Methods and analysis The authors plan a multicentre randomised parallel group complex intervention trial with concealment of group allocation from outcome assessors. Patients who required more than 48 h of mechanical ventilation and are deemed fit for intensive care unit discharge will be eligible. Patients with primary neurological diagnoses will be excluded. Participants will be randomised into one of the two groups: the intervention group will receive standard ward-based care delivered by the NHS service with additional treatment by a specifically trained generic rehabilitation assistant during ward stay and via telephone contact after hospital discharge and the control group will receive standard ward-based care delivered by the current NHS service. The intervention group will also receive additional information about their critical illness and access to a critical care physician. The total duration of the intervention will be from randomisation to 3 months postrandomisation. The total duration of follow-up will be 12 months from randomisation for both groups. The primary outcome will be the Rivermead Mobility Index at 3 months. Secondary outcomes will include measures of physical and psychological morbidity and function, quality of life and survival over a 12-month period. A health economic evaluation will also be undertaken. Groups will be compared in relation to primary and secondary outcomes; quantitative analyses will be supplemented by focus groups with patients, carers and healthcare workers.
Ethics and dissemination Consent will be obtained from patients and relatives according to patient capacity. Data will be analysed according to a predefined analysis plan.
Trial registration The trial is registered as ISRCTN09412438 and funded by the Chief Scientist Office, Scotland.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
The optimum method to maximise the rate and magnitude of recovery following an illness requiring intensive care is unknown.
Rehabilitation is a complex healthcare intervention, which following critical illness involves multiple healthcare professionals including doctors, nurses, physical therapists, dietitians, occupational therapists and other allied professionals.
The RECOVER trial hypothesises that providing more coordinated and intensive rehabilitation, delivered by a specialised generic rehabilitation assistant supported by the existing multidisciplinary team, will improve recovery as judged by a range of patient-centred outcome measures and is cost-effective.
Key messages
The RECOVER study will evaluate whether enhanced rehabilitation is clinically effective and cost-effective in patients enrolled at the time of ICU discharge.
Both positive and negative results will be clinically important in guiding future research directions and health service improvement.
Strengths and limitations of this study
RECOVER was informed by the recommendations of recent evidence-based NICE guidance, and a significant body of research was used to develop the intervention.
The trial has been designed to adhere closely to recent guidance concerning the evaluation of complex healthcare interventions, especially the measurement of process.
A weakness may be the inclusion of patients with a range of illness severity and disability from a general intensive care population; this could miss important effects in patient subgroups.
Introduction and background
Survivors of critical illness frequently suffer from severe disabilities that include physical, psychological, and social problems. These typically persist for many months, may not resolve completely1–3 and are associated with reduced health-related quality of life (HRQoL), which often fails to achieve preillness levels.1–4 The direct (healthcare) and indirect (carers/family) costs during this period are probably high but are not well studied. In the UK, a recent report (‘Quality Critical Care’)5 and a NICE guideline6 have highlighted the need to improve rehabilitation for this patient group. A systematic review undertaken during NICE guideline development indicated a lack of high-quality research concerning what interventions improve patient outcomes and their clinical and cost-effectiveness.6 Recommended future research questions included: “For patients at high risk of critical illness-associated morbidity, what is the clinical effectiveness and cost effectiveness of organised critical care rehabilitation versus usual care on physical and psychological functioning, participation and quality of life?”
Our pretrial work identified the following key issues in this area:
Patients have wide ranging health problems: the health problems that follow critical illness have been called the ‘post-ICU syndrome’.2 Physical impairment is typified by malnutrition, which is worsened by poor appetite and nausea. Patients can lose 10%–30% of their body mass during critical illness.3 Recovery is further delayed by joint stiffness, pain and neuropathies; levels of fatigue and breathlessness are high. Muscle weakness is particularly common and strongly associated with poor outcome. Problems with psychological health and social functioning are also common.7 ,8 Anxiety, depression and post-traumatic psychopathology (such as post-traumatic stress disorder) are reported in 10%–40% of patients. These problems are rarely screened for or addressed in most acute hospitals.
Patient rehabilitation is currently not coordinated: survivors are currently managed in acute hospitals with inconsistent fragmented strategies post-intensive care unit (ICU) discharge. Typically, specialty-based teams lead care and patients are widely dispersed within the hospital. Importantly, patients effectively ‘compete’ with less sick patient groups (eg, elective surgery patients) for limited rehabilitation resource. In a local audit, we found that 70% of patients were discharged directly home from the acute hospital without clearly planned rehabilitation.9 Coordination with primary care services was poor and inconsistent, and knowledge of the specific problems faced by the post-ICU patient was very limited among staff on the general wards and after discharge to the community.
Patients are major users of acute hospital resource: intensive care costs are high, mainly because of the high staffing levels required to provide multiple organ support on an individual patient basis. The duration of ICU stay is skewed towards a median stay of 2–3 days in most healthcare systems, but the minority of patients requiring longer ICU stay utilise the majority of ICU bed days and continue to utilise enormous hospital resource post-ICU discharge as a result of their residual disability. As the population ages and numbers of ICU admissions are expected to increase, this cohort of ICU survivors will place increasing pressure on acute hospital services. Clinically effective rehabilitation strategies therefore have potential to be both efficient and cost-effective.
Patient outcomes are poor: many patients report poor pre-ICU HRQoL and have chronic health problems prior to ICU admission,1 but HRQoL is significantly reduced in most patients following ICU discharge. Impaired physical function is particularly common during the first 3–6 months after discharge.1 ,4 Typically, recovery of HRQoL takes at least 12 months. Over 50% of patients are below retirement age and only half of those previously working have returned to work by 12 months. Patients have an excess risk of death compared with age- and sex-matched population for up to 5 years after discharge.10
Little research has evaluated interventions to improve outcomes following ICU discharge. A small randomised controlled trial (RCT) showed that self-help manuals, supported by a researcher, improved physical function at 6 months.11 A recent randomised trial found improvements in physical function at hospital discharge associated with early mobilisation in the ICU but did not address longer term patient benefits or report cost-effectiveness.12 Many critical care services provide nurse-led follow-up clinics at 3–12 months after hospital discharge, but this approach has little, if any, emphasis on the early recovery phase and a recent randomised trial was unable to demonstrate any clinical benefits or cost-effectiveness.13
Our pretrial work included a qualitative interview-based study evaluating the experience of 20 survivors of long-term ventilation during the 6 months following ICU discharge.14 We found that patients experienced profound debilitation during the ward phase of recovery and were frustrated by fragmented or specialty-led care, which seemed neither to take account of their individual needs nor issues specific to critical illness. Many were distressed by a perceived indifference among busy ward staff towards their significant dependence and needs. Concerns focused on the brevity and perceived inadequacy of rehabilitative provision (especially physiotherapy), while others felt ‘outside’ the rehabilitation process, in terms of their individual contribution and longer term goals and strategies. Many patients were discharged home with limited understanding of the nature or severity of their critical illness, which contributed to unrealistic expectations of recovery. In general, patients were ill equipped to manage their own recovery following hospital discharge and had limited access to clinicians in order to address their concerns. We developed a service model based around a generic rehabilitation assistant (GRA) to coordinate and deliver rehabilitation for these patients throughout their hospital stay and maintain contact after hospital discharge.15 In our model, rehabilitation is planned and supervised by ‘hard-stretched’ specialist staff (physiotherapists, dietitians, occupational therapists) but delivered by a single specifically trained GRA who develops a close relationship with the patient. We tested our model in a feasibility RCT and showed that markedly enhanced levels of treatments could be successfully delivered with this model, and the GRAs could function autonomously across specialist boundaries in the acute hospital.9 We further refined our service model to include a GRA training programme, predefined competencies and input from critical care staff to provide information to patients and families.
Methods
Trial objectives
Our primary objective is to evaluate the impact on physical, psychological and social functioning of a novel complex intervention strategy to enhance delivery of physical and nutritional rehabilitation to patients during the 3 months following ICU discharge. Our secondary objectives are to evaluate the cost-effectiveness of our approach and compare patient and carer experiences and satisfaction between usual care and the new strategy.
General design
RECOVER is a prospective, randomised, parallel group, controlled trial with concealment of outcome assessment. We are comparing our novel intervention with usual care. A schematic diagram describing the trial structure is shown in figure 1. The primary study outcome is the Rivermead Mobility Index (RMI) at 3 months postrandomisation, which is a measure of physical function in relation to mobility. As this is a trial of a complex intervention with potential effects on many outcomes important to patients and health services, we are measuring a range of secondary outcomes during 12 months of follow-up (table 1). The full trial protocol is available on the Edinburgh Clinical Trials Unit (ECTU) website: http://www.clinicaltrials.ed.ac.uk.

The general structure of the RECOVER trial.
The patient outcomes measured in the trial
Trial setting
The trial is taking place in Lothian Health Board's two major acute hospitals, which serve Edinburgh and the surrounding region. The hospitals are run as a single organisation with each major specialty grouping managed by a clinical director and management team. The critical care service is run as a discrete directorate with a single general critical care unit on each site. The Edinburgh Royal Infirmary ICU cares for approximately 700 mechanically ventilated patients each year and the Western General hospital ICU approximately 450 patients. Cardiac surgery and paediatric critical care are provided in separate ICUs. Further information about the critical care setting is available in the Scottish Intensive Care Society Audit report (http://www.sicsag.scot.nhs.uk/).
Subject screening and selection
All ICU admissions will be accounted for, and those receiving 48 h of continuous ventilation will be screened for eligibility. Inclusion criteria are the patient required ≥48 h of continuous invasive (via an endotracheal and/or tracheostomy tube) mechanical ventilation in the ICU and the consultant in charge of the patient considers them fit for discharge from the ICU. Exclusion criteria are a primary neurological admission diagnosis (brain trauma, intracerebral bleed, stroke, Guillain–Barre syndrome); the clinician in charge of care has agreed with the patient and/or family that only palliative care will be provided; patients currently receiving home ventilation or planning to commence a programme of home ventilation; patients expected to be discharged from ICU to a non-study hospital where the intervention cannot be received; gaining informed consent following the intervention or follow-up is not feasible due to communication difficulties; the patient currently enrolled in another RCT with similar endpoints and aged <18 years at the time of screening. The recruitment window will be up to 7 days from the time the patient fulfils entry criteria.
Consent
The study involves participants who may lack capacity as a result of acute illness. For these patients, the Adults with Incapacity Act (Scotland; 2000) applies. Patients with mental capacity will be approached for consent to participate in the trial. For those lacking mental capacity, the welfare attorney or next of kin will be approached for consent. For patients enrolled with this approach, patients will be approached for consent to remain in the trial once they regain capacity. The study information sheets are available on the ECTU website (http://www.clinicaltrials.ed.ac.uk).
Sample size
Based on our pilot study, we estimated that the mean (SD) RMI at 3 months postrandomisation will be 10 (4.3), with normal mobility being 15 on a 0–15 scale. Our pilot data suggested a change from baseline to 3 months in RMI of 2 (SD 5) is currently typical.9 We have powered the study to detect an improvement in the change from baseline RMI of 2 points at 3 months in the intervention group compared with usual care. This would be a clinically relevant difference in physical disability for patients in relation to activities of daily living and independence. To detect this difference, we require 100 evaluable patients per group at 3 months (80% power; 5% significance level). Assuming a 12% death rate before 3 months (based on pilot work) and 95% follow-up of remaining patients at 3 months (facilitated by home visits by research nurses), we require to randomise 240 patients in total. Using local audit data, we estimated that 498 eligible patients will be cared for each year of whom 309 will be discharged alive from ICU. Assuming 70% enrolment, we expect to enrol 216/year or 18/month. The planned recruitment period is therefore 14 months.
Method of assignment to treatment groups
Patients will be randomised 1:1 to receive either existing usual care or the novel intervention. Randomisation will be by a remote computer-based telephone system to ensure allocation concealment. At randomisation, minimisation with a random element will be used to balance the following baseline variables: age (>65 vs ≤65 years); disability at study entry (RMI 0–5 vs 6–10 vs 11–15); nutritional status at randomisation (physical assessment element of the Subjective Global Assessment of nutrition16: malnourished versus well nourished); the presence/absence of delirium (using CAM-ICU) and the ward destination of patient (surgical vs medical).
Study intervention
Duration
The study intervention will start from the time of patient randomisation, which will be within 48 h of consent, and last until 3 months postrandomisation. Patients are expected to require variable periods of time in the acute hospital and the community during the 3-month intervention, depending on individual health status. Following the 3-month assessment, all patients will receive usual care irrespective of their location, but relevant healthcare professionals will be made aware of any key issues by the research team to ensure patient safety. Based on audit data, we expect only a small proportion of patients to remain in hospital at 3 months when the primary outcome is measured.
Description of treatments received
RECOVER is a complex intervention trial and, as recommended by the MRC complex intervention framework, we are describing the process of care received in each group in detail.17 To achieve this, we have identified four key stages of the patient pathway during which we believe key and important components of rehabilitation occur. These comprise the immediate post-ICU discharge period (stage 1); ward-based rehabilitation in the acute hospital (stage 2); acute hospital discharge planning (stage 3) and the posthospital discharge period (stage 4). These stages will have differing durations and timings in relation to randomisation according to individual patient requirements. The processes and treatments that we want to measure during each stage have been defined a priori and will be recorded prospectively according to a proforma (see data collection and table 2).
The process measures and treatments recorded prospectively to describe the rehabilitation received during the intervention period
Intervention group procedures
Generic rehabilitation assistants
GRAs will be employed to work exclusively with patients randomised to the intervention group. We previously described the concept of the specialist critical care rehabilitation assistant.15 For RECOVER, we calculated that the workload would require 2.5 whole time equivalent posts working flexibly across the two hospitals under the supervision of a multidisciplinary rehabilitation team comprising physiotherapists and dietitians and some input from speech and language therapy and occupational therapy. The GRAs will be trained to use systematic screening tools for common problems and deliver therapy according to predefined competencies. All GRAs will receive a 4-week training programme prior to starting the trial. A description of the training programme is available on the RECOVER page of the ECTU website (http://www.clinicaltrials.ed.ac.uk).
Stage 1 interventions
A lay summary will be produced by an ICU consultant or nominated member of staff and made available to patients, their relatives and relevant healthcare professionals providing a brief summary of key events that occurred during the patient's stay in intensive care. All patients will receive a visit from a Critical Care consultant or nominated deputy, organised by the GRA for an appropriate time mutually convenient to the patient, the consultant and the patient's relative (if they wish to attend). A predefined topic guide will be used to cover key aspects of the critical illness pathway and will include possible short- and long-term complications. The proforma used to dictate the lay summary, and the topic guides used for the consultant visit are available on the RECOVER page of the ECTU website (http://www.clinicaltrials.ed.ac.uk).
Stage 2 interventions
The GRA will deliver an enhanced and coordinated rehabilitation under the supervision of the multidisciplinary specialists, based on frequent visits according to the requirements of individual patients and clinical workload. Key elements will include the following: individualised goal setting with each patient in a range of areas; a clear plan of exercises and nutrition interventions aimed at achieving the goals; regular systematic screening for anticipated problems relating to nutrition and physical disability using tools agreed with physiotherapy, dietetic, occupational therapy and speech and language therapy teams. These will be used to trigger specialist input using predefined thresholds or criteria. The screening tools used by the GRAs to detect patient problems and refer to more senior specialists within the rehabilitation team are available on the RECOVER page of the ECTU website (http://www.clinicaltrials.ed.ac.uk).
Stage 3 interventions
The GRA will input into hospital discharge planning by the multidisciplinary team based on their detailed knowledge of ongoing patient problems and issues.
Stage 4 interventions
After discharge home, the GRA will contact the patient within the first week to enquire how they are managing at home and whether there are any issues that have arisen. The patient will be provided with a telephone number at discharge, through which they can contact the GRA to discuss any issues.
Usual care procedures
The NICE guideline makes recommendations regarding best practice but acknowledges that these are largely expert/opinion based or based on extrapolation from other rehabilitation settings.6 Our pretrial work showed that the intensity of physiotherapy and dietetic input was limited and that ward visits by ICU clinicians is not routine care. The strongest evidence for effectiveness on physical recovery was provision of a self-help manual, supported by expert staff, during the weeks after ICU discharge.11 For the purpose of RECOVER, we intend ‘usual care’ to be externally valid as representative of practice in the NHS (or other healthcare systems). We will include provision of an ICU recovery manual as part of ‘usual care’ because data exist to support this intervention. Otherwise rehabilitation will be provided by NHS multidisciplinary teams using the current arrangements in the study hospitals, which does not include any specialist critical care GRAs. Detailed process data collection for both groups will ensure that the treatment received in both arms is well described.
A summary of the interventions expected to occur at each stage of recovery for each group is summarised in figure 2.

A description of the conceptual stages in the patient journey and the intended differences in the rehabilitation provided for the two groups.
Data collection
Baseline data
We will record age, gender, social class (postcode based), Functional Co-morbidity Index (based on prehospital admission data), ICU diagnosis (Scottish Intensive Care Society code) and APACHE II score at ICU admission. At randomisation, we will record prerandomisation ICU length of stay and total hospital length of stay; days of mechanical ventilation, vasopressor use and renal replacement therapy; source of nutrition at study entry; Sequential Organ Failure Assessment score at randomisation; delirium at randomisation (CAM-ICU tool); RMI and the physical component of the Subjective Global Assessment of Nutrition tool score.
Process of care data
Detailed quantification of predefined elements of rehabilitation will be recorded on a weekly basis by research staff from randomisation until hospital discharge. These fields are summarised in table 2.
Outcome data
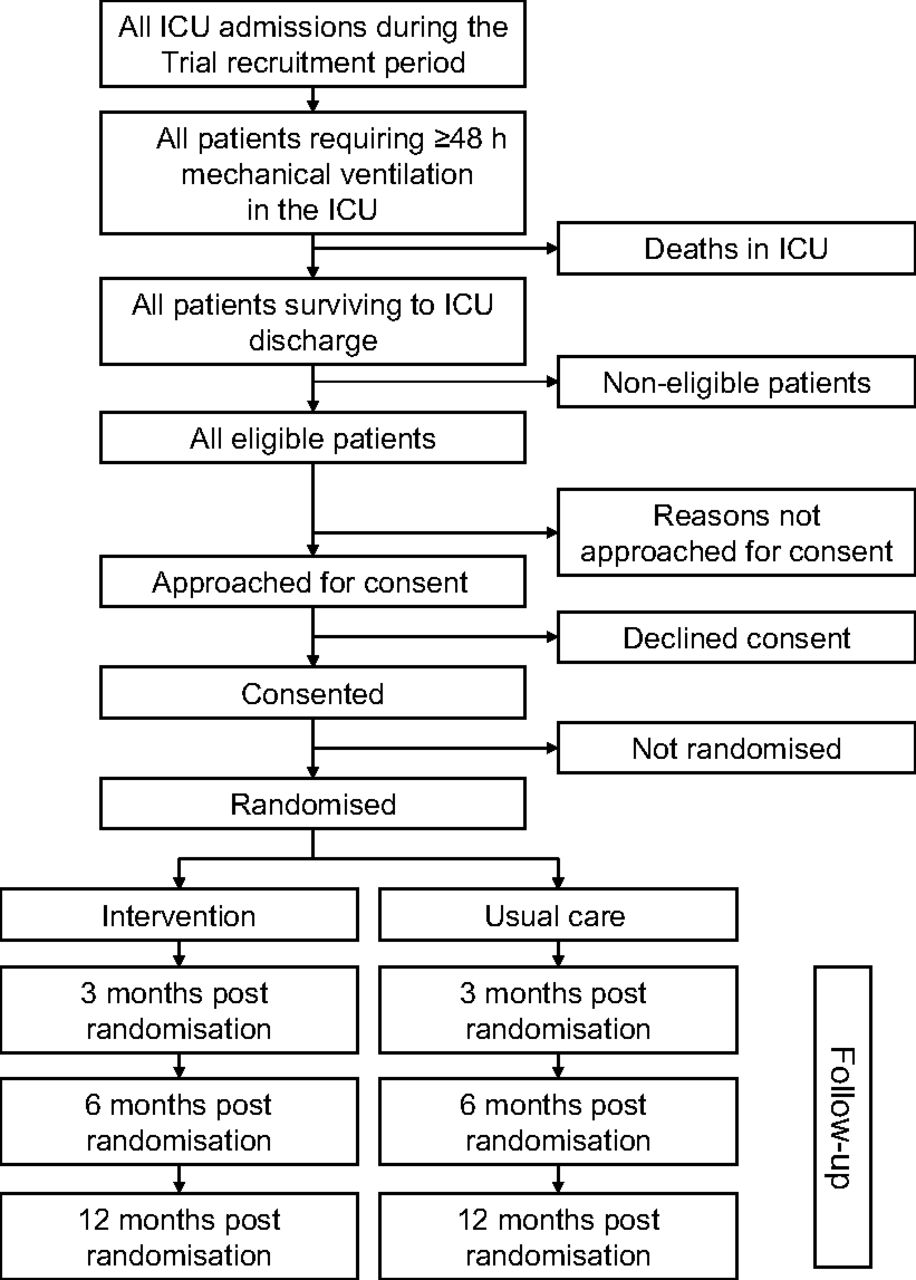
The primary and secondary outcome data are summarised in table 1. At 3 months postrandomisation, all surviving participants will be contacted and a home visit undertaken by community research nurses blinded to group allocation, with no previous knowledge of the participant. Patients remaining in hospital at 3 months will be assessed by research staff blinded to group allocation. At 6 and 12 months, postrandomisation surviving patients will be contacted by the trial office and outcomes measured using postal questionnaires. A predefined standard operating procedure will be used to maximise rates of follow-up and completion of the primary and secondary outcomes; this is summarised on the RECOVER page of the ECTU website (http://www.clinicaltrials.ed.ac.uk). Patient survival up to 10 years will be ascertained through linkage to the Information and Services Division Database through the Scottish Intensive Care Society Audit Database. The proposed CONSORT diagram is shown in figure 3.
{kind=link}
{kind=link}
{kind=link}
The CONSORT diagram that will be reported to account for all patients screened for eligibility, approached for consent, enrolled in the trial and followed up and the predefined time points. For each cell, the numbers of patients will be included. For the follow-up time points, the numbers of patients completing the various outcome measures will be recorded.
Data management
All data will be collected to paper Case Record Files and entered into a bespoke database. Quality checks will generate queries, which will be resolved with research site staff. All data queries will be resolved prior to locking the database for analysis. Data will be stored in the ECTU or associated data archiving facilities for a minimum of 15 years to enable subsequent ascertainment of long-term health status through national database linkage.
Data analysis
The primary analysis will be performed according to the intention-to-treat principle. As the trial is testing a complex intervention involving health service redesign, we do not propose a separate analysis of patients who did not receive any or certain elements of the intervention. The primary outcome measure, RMI at 3 months postrandomisation, will be compared between the groups using analysis of covariance to adjust for baseline RMI and for the factors included in the minimisation algorithm. A sensitivity analysis will be performed where the lowest possible value of RMI (0) is imputed for those patients who die within 3 months of randomisation. A similar approach will be used to analyse the secondary outcome measures. A detailed analysis plan has been written for the baseline variables, process measures and primary and secondary outcome variables. The analysis plan is available on the ECTU website (http://www.clinicaltrials.ed.ac.uk).
Qualitative study
We plan to maximise the information obtained about the intervention using a mixed methods approach, incorporating qualitative research. Focus group interviews will be conducted, recorded and transcribed at each of the participating hospitals.
Patients and carers
Using purposive sampling, we will invite 8–10 patients and carers from the ‘usual care’ and intervention groups at each site to participate in separate focus groups. Participants will be invited to discuss their experiences of recovery and rehabilitation up to 3 months post-ICU discharge. We will explore key issues and concerns and the ways in which multi-disciplinary input impacted upon recovery both during the acute hospital phase and following discharge home. A comparative analysis between the ‘usual care’ and intervention focus groups will explore the impact of the intervention on participants' key issues and concerns.
Healthcare professionals
Using purposive sampling, we will invite 8–10 representatives from key healthcare disciplines at each site to participate in focus group interviews towards the end of the recruitment period. Drawing upon our analysis of the research logs, participants will be invited to discuss barriers to the delivery and coordination of patient-led care among both groups and perceptions (including acceptability) of the GRAs as a novel strategy for the rehabilitation of patients after ICU discharge.
Assessment of research logs kept by GRAs
The GRAs will keep a log throughout the trial to record their experience of the novel role. Using thematic analysis, we will analyse these to categorise the principle barriers to the intervention and successful strategies in the implementation of the intervention both in individual patients and across ward and hospital settings. These data will supplement the quantitative measurement of process outcomes and facilitate the translation of findings into routine care.
Blood sampling for biomarker inflammation study
A substudy will investigate the prevalence of persisting inflammation following ICU discharge and its relationship with recovery. For patients who consent to additional blood sampling, a 10 ml blood sample will be collected at randomisation, weekly until hospital discharge and at the 3-month visit, and stored frozen as plasma and serum. Biological substances involved in the inflammatory response will subsequently be measured and related to measures of physical recovery.
Health economic evaluation
Cost-effectiveness will be estimated using a prospective within trial analysis of treatment effects analysed on an intention-to-treat basis and a decision model of long-term costs and health outcomes. The primary endpoint for the economic analysis will be incremental cost-effectiveness ratios comparing the intervention group with the usual standard of care impact, focusing on health service use and HRQoL. Health service costs will be assigned to the type and intensity of resource use measured by rehabilitation interventions/contacts, medications, hospital clinic attendances and hospitalisation episodes from randomisation to 12 months of follow-up. The health economic questionnaire used in the study is available of the ECTU website (http://www.clinicaltrials.ed.ac.uk). Unit costs will reflect a mixture of approaches including activity-based analyses of resource consumption for specific rehabilitation interventions alongside average per diem inpatient costs calculated on a specialty-specific basis using the Scottish Health Service Costs system. Endpoints for health effects will include survival times and quality-adjusted survival times. Quality-adjusted survival times per life years will be calculated for all randomised patients using the HRQoL measures. These within trial analyses will be integrated into a decision model of long-term costs and health effects. We propose to use a Monte-Carlo microsimulation model. Base case analysis, using the intention-to-treat results, and sensitivity analysis will be conducted by varying key model parameters and critical assumptions over plausible ranges/distributions. The decision model will also permit the analysis of cost-effectiveness conditional on prespecified patient subgroups to allow for heterogeneity in the case mix of patients receiving intensive care and their baseline condition at ICU discharge. A full description of the proposed analysis can be found in the full protocol on the RECOVER page of the ECTU website (http://www.clinicaltrials.ed.ac.uk).
Research governance
The trial will be carried out under the principle of the International Conference for Harmonisation of Good Clinical Practice guidelines. Specifically, the research sponsors' (Edinburgh University/Lothian Health Board) guidelines for adverse event reporting policy and Standard Operating Procedures will be followed. These are consistent with adverse event reporting guidelines from the National Research Ethics Service for safety reporting in research other than clinical trials of investigational medicinal products. A monitoring plan will be agreed with the sponsor early in the trial.
Ethics
The trial has received a favourable ethical opinion by the Scotland A Research Ethics Committee (Ref 10/MRE00/18) and is approved by the NHS Lothian R&D department (Ref 2010/R/AN/02).
Trial management
The trial will be managed by a Trial Management Group and overseen by a Trial Steering Group, which includes an independent Chairman, two independent clinical specialists, and a lay representative. A Data Monitoring and Safety Committee will monitor the progress, quality and safety of the trial. The membership of these committees is available on the RECOVER page of the ECTU website (http://www.clinicaltrials.ed.ac.uk). The trial registration number is ISRCTN: 09412438 and the trial is registered on the NIHR Clinical Research Network (Critical Care portfolio; number 8849).
Related studies
RECOVER is part of a programme of work exploring rehabilitation needs and intervention strategies following critical illness. Two other studies (RELINQUISH study and EATEN study) will sample cases enrolled in the trial.
The RELINQUISH study (REcovery following critical illness: a Longitudinal Qualitative exploration of perceived healthcare and Support needs among survivors; developing timely interventions after Hospital discharge; NIHR portfolio number 9986) will invite up to 24 participants enrolled in the RECOVER trial to each take part in four interviews over the 12 months following ICU discharge. Purposive sampling will be used to enrol equal numbers from each of the RECOVER groups with representation from relevant subgroups according to age, gender, duration of mechanical ventilation, ward discharge destination, occupational status and level of social support. The study aims are to examine the ways in which perceived healthcare and support needs change over time, to assess the extent to which these needs are currently met by formal and informal community-based resources, to identify potential service improvements for survivors of critical illness throughout the recovery process following discharge into the community and to explore the impact of the RECOVER intervention upon the perceived healthcare and support needs of survivors following discharge into the community. RELINQUISH is funded by the Health Services Research Unit of NHS Lothian; the PI is Dr Pam Ramsay (coinvestigator for the RECOVER trial).
The EATEN study (An Exploration of the bArriers to nutritional intake after inTENsive care; NIHR portfolio number 10631) will invite up to 17 participants in the RECOVER study to participate in sequential hospital based interviews and field work, followed by an interview 3 months following ICU discharge. The study will explore the barriers to achieving nutritional recovery during this period of recovery and is funded as part of a dietetic PhD Fellowship for Judith Merriweather (coinvestigator for the RECOVER trial) by the Chief Scientist's Office, Scotland.
References
Footnotes
To cite: Walsh TS, Salisbury LG, Boyd J, et al. A randomised controlled trial evaluating a rehabilitation complex intervention for patients following intensive care discharge: the RECOVER study. BMJ Open 2012;2:e001475. doi:10.1136/bmjopen-2012-001475
Contributors The following is taken from the submitted manuscript. The initials refer to the listed co-authors: TSW, LGS, PR, JM and GH conceived the project and completed pilot and feasibility work. Specialist clinical input to protocol design was provided by TSW and SJM (critical care perspective), LGS (physiotherapy/rehabilitation), PR and JZR (nursing) and JM (dietetics). Statistical advice was provided by GDM and SL and the health economic evaluation designed by JF. The qualitative studies were conceived and designed by PR, GH and JZR. The inflammatory biomarker substudy was designed by TSW and DMG. Advice on health service reorganisation aspects was provided by SJM and GH. Advice on psychological outcomes and interventions was provided by AH and JZR. JB is trial manager. All authors contributed to the design of the final protocol and set-up of the trial.
Funding Funded by the Chief Scientists Office, Scotland (grant number CZH/4/53). Additional funding has been provided through the Edinburgh Critical Care Research Group.
Competing interests None.
Ethics approval Ethics approval was provided by Scotland A REC.
Provenance and peer review Not commissioned; internally peer reviewed.