Article Text

Statistics from Altmetric.com
Answer
From the question on page 138
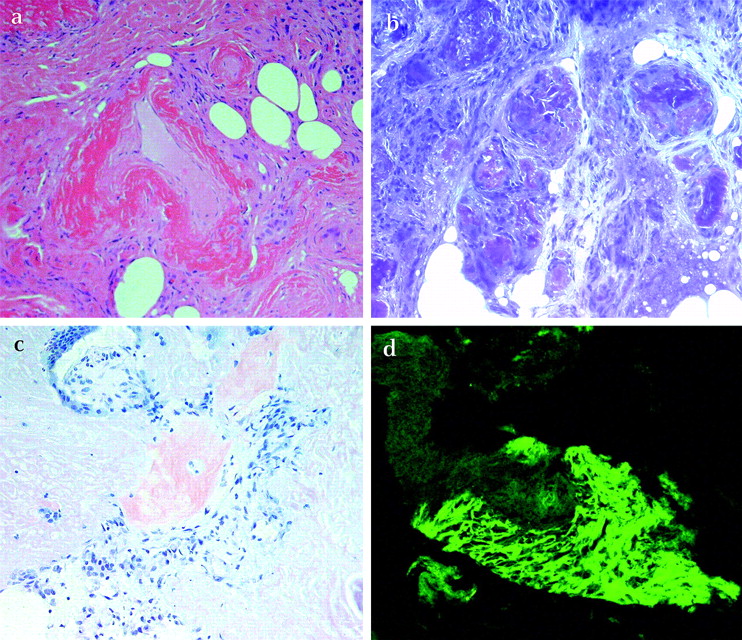
Immunohistochemical stains for crystal violet, congo red and thioflavine T were positive (figure 1), with no significant staining for transthyretin or amyloid A. Multiple myeloma screening, including bone marrow biopsy, was unremarkable. Given the abundance of plasma cells on biopsy and absence of underlying chronic disease, the diagnosis of primary mediastinal amyloid was made. The patient is currently receiving cyclophosphamide and dexamethasone under the care of the Haematology unit. While immunohistochemical staining for amyloid A protein was negative, secondary amyloidosis (eg, due to multiple myeloma) remains significantly more common than primary amyloidosis. The patient continues to undergo regular clinical and biochemical review (including serum and urine protein eletrophoresis) during treatment. No evidence of myeloma or other systemic disease has been noted during 11 months of follow-up since the original diagnosis of primary amyoidosis was made.
{kind=link}
Pathology of endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) specimen. (a) H&E—amyloid demonstrated by brightly eosinophilic (red) material outlining a blood vessel; (b) Crystal Violet—positive metachromatic staining of amyloid (deep purple); (c) Congo Red—weak staining of amyloid tissue (pink); (d) Amyloid fluorescence following staining with Thioflavine T.
Discussion
Amyloidosis is a heterogenous group of diseases associated with extracellular tissue deposition of insoluble protein fibrils, which can be primary or secondary. Primary amyloid tumours of intrathoracic nodes are extremely rare.1
The radiological appearance of amyloid is non-specific. Intrathoracic nodal amyloid has been reported to be positive on [18F]FDG positron emission tomography (PET) in patients with secondary amyloidosis2 3 though findings for primary amyloidosis have not previously been described.
Mediastinoscopy is the “gold standard” diagnostic approach for intrathoracic nodal amyloidoma given that the firm-to-hard consistency of amyloid deposits poses sampling difficulties. However, it requires general anaesthesia, with mortality and major morbidity rates of 0.2% and 2%, respectively.4 5 Diagnosis may be made using less invasive procedures, with Hiller et al describing mediastinal amyloid successfully diagnosed by percutaneous needle biopsy.1 Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is an effective, minimally invasive and safe method for assessing intrathoracic lymphadenopathy for suspected malignancies6 and possibly benign diseases, including sarcoidosis.6 This is the first case of primary amyloidoma of intrathoracic lymph nodes diagnosed by EBUS-TBNA.
In summary, we present a rare case of primary amyloidoma as the cause of intrathoracic lymphadenopathy with intense FDG activity on PET. Our case once again confirms the value of EBUS-TBNA in the diagnosis of intrathoracic lymphadenopathy.
Linked Articles
- Pulmonary puzzle