Article Text

Statistics from Altmetric.com
Clinical presentation
A 46-year-old man of Ethiopian origin was admitted to hospital in 2008 for investigation of cough, increasing dyspnoea and weight loss over several weeks. He was known to be HIV positive. He had a history of several opportunistic infections, including Cryptosporidium diarrhoea, tuberculosis, Mycobacterium avium complex and Pseudomonas pneumonia. He had also been treated in 2005 for visceral leishmaniasis with liposomal amphotericin. His prescribed medication included trimethoprim–suxamethoxazole, clarithromycin, efarinez, lamivudine, zidovudine and folic acid. His compliance with highly active antiretroviral therapy (HAART) was known to be poor.
On physical examination he was afebrile. Aside from moderate tachypnoea (24 respirations/min), his vital signs were normal. General examination showed cachexia and marked parotid swelling. The abdomen was non-tender with hepatosplenomegaly. Cardiac/respiratory examination was normal.
Laboratory testing revealed a normal haemoglobin level (14.4 g/dl), leucopenia (total white cell count 1.46×109/l; neutrophils 1.0×109/l, lymphocytes 0.3×109/l, eosinophils 0.1×109/l) and thrombocytopenia (113×1012/l). CD4 count was 34×106 cells/l. Other blood tests were within the normal range, except for hypoalbuminaemia and elevated liver enzymes in a cholestatic pattern.
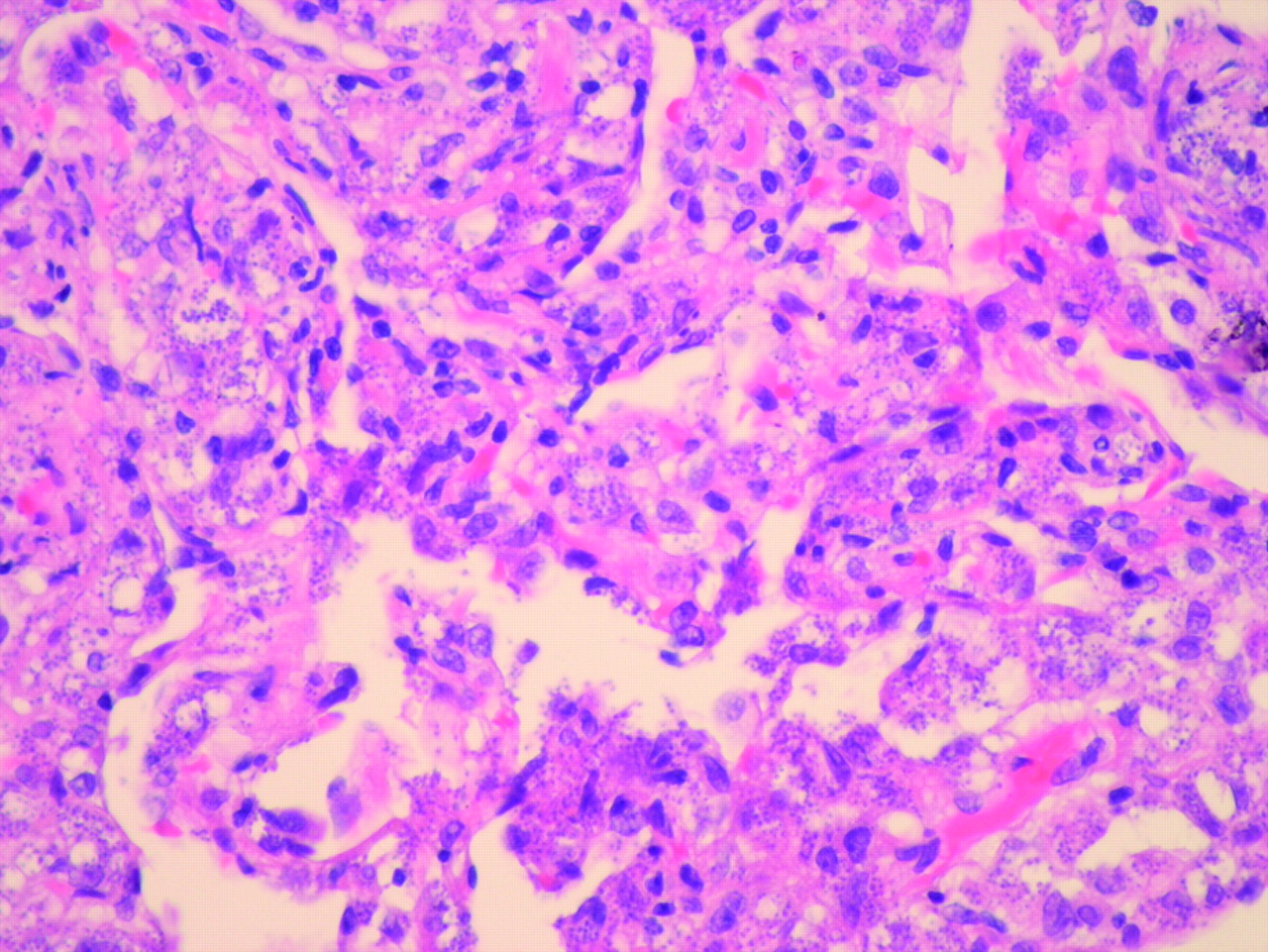
On admission to our institution, the chest radiograph showed diffuse bilateral airspace opacities mainly in the left upper and right lower lobes (Supplementary fig 1 online). CT scan of the thorax performed elsewhere 1 month prior to his admission showed peripheral pulmonary consolidation throughout the left lung and bilateral areas of ground-glass opacities (Supplementary fig 2). Massive hepatosplenomegaly was noted (Supplementary fig 3). A transbronchial biopsy was performed (figs 1 and 2).

Transbronchial biopsy: the lung parenchyma is heavily infiltrated with mononuclear cells containing a large number of small purple/blue staining structures (H&E stain ×40 magnification).

{kind=link}
{kind=link}
Transbronchial biopsy: as fig 1, but at higher magnification (H&E stain ×100 magnification with oil immersion).
Question
What is the diagnosis?
Answer
The transbronchial biopsy showed large numbers of mononuclear cells in both bronchial and parenchymal tissue. The mononuclear cells were heavily parasitised with Leishmania amastigotes (figs 1 and 2). No granulomas were seen. Leishmania spp. were also identified in a parotid aspirate (Supplementary fig 4). Stains and cultures were negative for bacteria, fungi, mycobacteria, Pneumocystis jirovecii and cytomegalovirus.
Leishmaniasis is usually spread through sandfly bites, although direct human–human transmission may occur via needle sharing.1 2 The Leishmania parasite resides free in the sandfly digestive tract in the proamastigote form. Upon entering the human host, the parasite is taken up by macrophages where it transforms to the obligate intracellular amastigote stage. Depending on the leishmaniasis species, macrophage traffic patterns and host immunity, the infection may remain localised in the skin (cutaneous leishmaniasis) or may disseminate systemically (visceral leishmaniasis or kala-azar as in this case). The typical systemic spread is throughout the reticuloendothelial system (bone marrow, spleen and liver) although any organ may be affected. Pulmonary involvement with kala-azar is uncommon, with very few cases reported.3 Diagnosis is usually made by biopsy of the affected organs, although microbiological, serological and PCR techniques exist. Visceral leishmaniasis is treated with pentavalent antimony compounds or amphotericin B.4
Patients with advanced HIV disease frequently present with respiratory illness, and the differential diagnosis is extremely wide.5 Asymptomatic hepatosplenomegaly is a common feature in patients with HIV, although in this clinical context its presence narrows the differential somewhat to cytomegalovirus, toxoplasmosis, leishmaniasis, schistosomiasis, endemic mycoses, M avium complex, miliary tuberculosis and HIV-associated lymphoma. The previous treatment for leishmaniasis was a “red-herring” since the parasite is difficult to eradicate completely and may recur, especially in immunosuppressed patients.1
Footnotes
Patient consent Obtained.
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
▸ Additional figures are published online only at http://thorax.bmj.com/content/vol65/issue1
Linked Articles
- Airwaves