Article Text

Abstract
Introduction Asthma attacks are responsible for considerable morbidity and may be fatal. We aimed to identify and weight risk factors for asthma attacks in children (5–12 years) in order to inform and prioritise care.
Methods We systematically searched six databases (May 2016; updated with forward citations January 2017) with no language/date restrictions. Two reviewers independently selected studies for inclusion, assessed study quality and extracted data. Heterogeneity precluded meta-analysis. Weighting was undertaken by an Expert Panel who independently assessed each variable for degree of risk and confidence in the assessment (based on study quality and size, effect sizes, biological plausibility and consistency of results) and then achieved consensus by discussion. Assessments were finally presented, discussed and agreed at a multidisciplinary workshop.
Results From 16 109 records, we included 68 papers (28 cohort; 4 case-control; 36 cross-sectional studies). Previous asthma attacks were associated with greatly increased risk of attack (ORs between 2.0 and 4.1). Persistent symptoms (ORs between 1.4 and 7.8) and poor access to care (ORs between 1.2 and 2.3) were associated with moderately/greatly increased risk. A moderately increased risk was associated with suboptimal drug regimen, comorbid atopic/allergic disease, African-American ethnicity (USA), poverty and vitamin D deficiency. Environmental tobacco smoke exposure, younger age, obesity and low parental education were associated with slightly increased risk.
Discussion Assessment of the clinical and demographic features identified in this review may help clinicians to focus risk reduction management on the high-risk child. Population level factors may be used by health service planners and policymakers to target healthcare initiatives.
Trial registration number CRD42016037464.
- Paediatric asthma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
What are the factors that could enable clinicians and healthcare services to ‘spot the child’ (5–12 years) with asthma who is at increased risk of a severe asthma attack (requiring systemic steroids or hospital care)?
What is the bottom line?
The ‘at-risk’ picture that emerges is of a child with persistent symptoms who has had previous attacks and is on a suboptimal treatment regimen, especially if they have poor access to healthcare services or other risk factors including comorbid atopic/allergic diseases, vitamin D deficiency, living in poverty and being of African-American ethnicity.
Why read on?
This systematic review identifies risk factors and, based on the consensus view of an Expert Panel, weights the factors to enable parents, clinicians and healthcare services to target evidence-based management on children with asthma at most risk of having a severe attack.
Introduction
Asthma is the most common long-term condition in children, with European prevalence rates among 6–7 year-olds ranging from 5% in Albania to 21% in the UK.1 Asthma is responsible for substantial morbidity, resulting in 2.8 million school days lost annually in the UK,2 many involving time off work for parents/carers.3 In the UK, more than 25 000 children are admitted annually with an asthma attack.4 Frequent attacks affect the quality of life of children and their parents, are associated with accelerated loss of lung function5 and may be fatal.
Asthma guidelines recommend that monitoring should include regular assessment both of current symptom control and future risk of an attack.6 7 Objective assessment of symptoms may be achieved with questionnaires validated in children (eg, Paediatric Asthma Control Questionnaire8; Childhood Asthma Control Test9) or morbidity scores (eg, Royal College of Physicians three questions10) but no evidence-based tools exist for informing assessment of future risk in children.
Guidelines list factors associated with an increased risk of attacks,6 including a recent history of severe attacks, poor symptom control, allergic sensitisation, comorbid rhinitis, exposure to environmental tobacco smoke (ETS), high use of reliever medication, poor adherence to controller medication, obesity, eosinophilia, elevated FENO, psychosocial problems and impaired spirometry. The relative contribution of these factors to increased risk, and how they may be used to stratify risk is not clear; clarifying this issue has been identified as a research priority.7
We were commissioned by Asthma UK to undertake a systematic review to identify factors associated with the risk of attacks in children aged 5–12 years with asthma and, based on the consensus view of a multidisciplinary Expert Panel, to weight their importance and the strength of the underpinning evidence to inform risk stratification.
Methods
The systematic review is registered with PROSPERO (CRD42016037464); the protocol is published.11 We followed Cochrane methodology12 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting standards.13
Search strategy
We searched MEDLINE, EMBASE, CINAHL, AMED, PsycINFO and CENTRAL in May 2016: with no language or date restrictions, identified unpublished and in-progress studies from ClinicalTrials.gov and the ISRCTN registry (https://www.isrctn.com), undertook forward and backward citation checks. The search strategy was structured to include terms for ‘Asthma’ and ‘Exacerbations/Attacks’ and ‘Risk factors/Predictors’.11 (Online supplementary table S1 gives detailed search strategies.) We contacted experts in the field for potentially relevant papers and anticipated risk factors to ensure we captured all likely predictors.
Supplemental material
Selection of studies
After initial deduplication and sift of obviously irrelevant titles (NT, SM, SMcL, AudB), two reviewers (NT, SM or AudB and SMcL or HP) independently screened titles/abstracts of papers identified. Two reviewers (AudB and SMcL) screened the full text of potentially eligible studies against review criteria. At each stage, disagreements were resolved by team discussion with advice from the study Steering Group (the grant holders and other members of the ARC group).
Inclusion and exclusion criteria
The focus of the review was to identify factors that increased a child’s propensity to asthma attacks. Definitions6 7 14 and key decisions regarding operationalising the inclusion/exclusion criteria are detailed in table 1. We used the American Thoracic Society/European Respiratory Society Task Force14 definition of severe asthma attacks: asthma symptoms and/or airway obstruction outside the normal variation for the patient necessitating a short course of oral corticosteroids and/or hospitalisation/emergency department use. The population included were children aged 5–12 years with a doctor diagnosis of asthma. Studies with a wider range of ages (eg, 3–18 years) were included if children aged 5–12 were reported separately or if more than 50% of the children were within this age range.
Criteria for the search strategy and rules devised to operationalise inclusion/exclusion criteria
Quality assessment
We assessed study quality using Newcastle-Ottawa Scale for cohort, case-control and cross-sectional study designs.15
Data extraction
We extracted details of study design, setting, population, methods, risk factors, definition of asthma and attacks, quality assessment, statistical analyses and results relevant to our objectives using a piloted form, modified from the Cochrane Effective Practice and Organisation of Care data collection form.16 We contacted authors to clarify unclear or missing data.
Quality assessment and data extraction were conducted by AudB or SMcL and one of eight reviewers (JFK, MW, HB, VD, SS, MP, HKZ or ED) trained to undertake independent duplicate quality assessment and data extraction. Disagreements in quality assessment were independently verified and arbitrated by the principal investigator (HP) who also checked the data presented in the tables.
The results for each risk factor were entered onto a table (online supplementary table S2), in order to facilitate weighting. Within each factor, the results were listed from strongest to weakest study design (ie, cohort, case-control, then cross-sectional) and then ranked by study quality (quality assessment score).
Supplemental material
Data synthesis: risk factor weighting
We anticipated that clinical and statistical heterogeneity of data would preclude formal meta-analyses. We therefore convened an Expert Panel (selected to provide a range of perspectives from among senior clinical academics of the Asthma UK Centre for Applied Research and the research team) comprising a general practitioner (GP) (HP), three respiratory paediatricians (JYP, JH, MS) and two researchers with a public health background (AudB, JFK), to make weighting decisions by reviewing the ORs and CIs, or other relevant statistics, as presented for each risk factor in online supplementary table S2. The Panel also had access to the full-text papers. The experts initially worked independently, and then met to reach consensus on weighting. In methodology analogous to the grading of recommendations in which both outcomes and quality of evidence are assessed, there were two decisions to be made:
What is the risk associated with each factor? Following discussion, thresholds for the risk weighting based on the majority of ORs for each factor were agreed (see table 2). The risk factor weighting ranged from ‘no’, ‘slightly’, ‘moderately’ or ‘greatly’ increased risk of future attack.
How confident is this estimate of risk? The Expert Panel based the confidence assessment on the following criteria: the number of studies, study design (cohort, case-control and cross-sectional), quality of studies included (Newcastle-Ottawa Scale), consistency of the results and the biological plausibility of the factors’ effect on risk of future attacks to determine the confidence with which the estimates were made. Assessments were rated as ‘highly’, ‘moderately’, ‘slightly’ confident or ‘inconclusive/insufficient evidence’.
Thresholds for weighting risk factors
At the consensus meeting, each factor was considered in turn and all available data taken into account when reaching the decision on risk and confidence. Any subsequent discussion was carried out by email.
Data synthesis: overarching risk
Risk factors for which there was sufficient evidence to reach a consensus decision on weighting and confidence in the assessment based on the decisions reached during Expert Panel discussion were illustrated on a bubble plot. The position of the bubble denotes the weighting of the risk factor and the size of the bubble indicates confidence in the estimate.
End-of-project workshop
An end-of-project videoconference (to allow UK-wide participation) workshop was held in January 2017, in which the researchers and the members of the Expert Panel were joined by a multidisciplinary group (n=18: including medical/nursing professionals from primary and secondary care, health service researchers, patient and public involvement (PPI) members) who reviewed and helped interpret the findings. In addition to the weighting table, data on each factor were presented to the workshop as Forest plots (online supplementary table S3) and the bubble plot constructed to visually display the overall results. Each risk factor was discussed, the weighting assessment reviewed and agreed, and the implications considered from the perspective of the different stakeholders.
Supplemental material
Patient and public involvement
Two parents of children with asthma (recruited from the Asthma UK Centre for Applied Research PPI Group) were involved throughout the study. In addition, representatives of Asthma UK attended the end-of-project workshop.
Updating prior to publication
In order to update the review prior to publication, we undertook forward citation on all included studies (January 2017). Pursuing references from included studies is an efficient approach to updating systematic reviews as it is unlikely that relevant papers will have been published without citing at least one of the included studies.17
Results
Search results
The searches yielded 21 963 records. Figure 1 (PRISMA diagram) gives details of the search and selection process. After deduplication and title/abstracts screening, 209 papers remained for full-text review of which 45 were included. Forward and backward citations yielded 23 additional papers; thus, 68 studies were included in the final analysis.
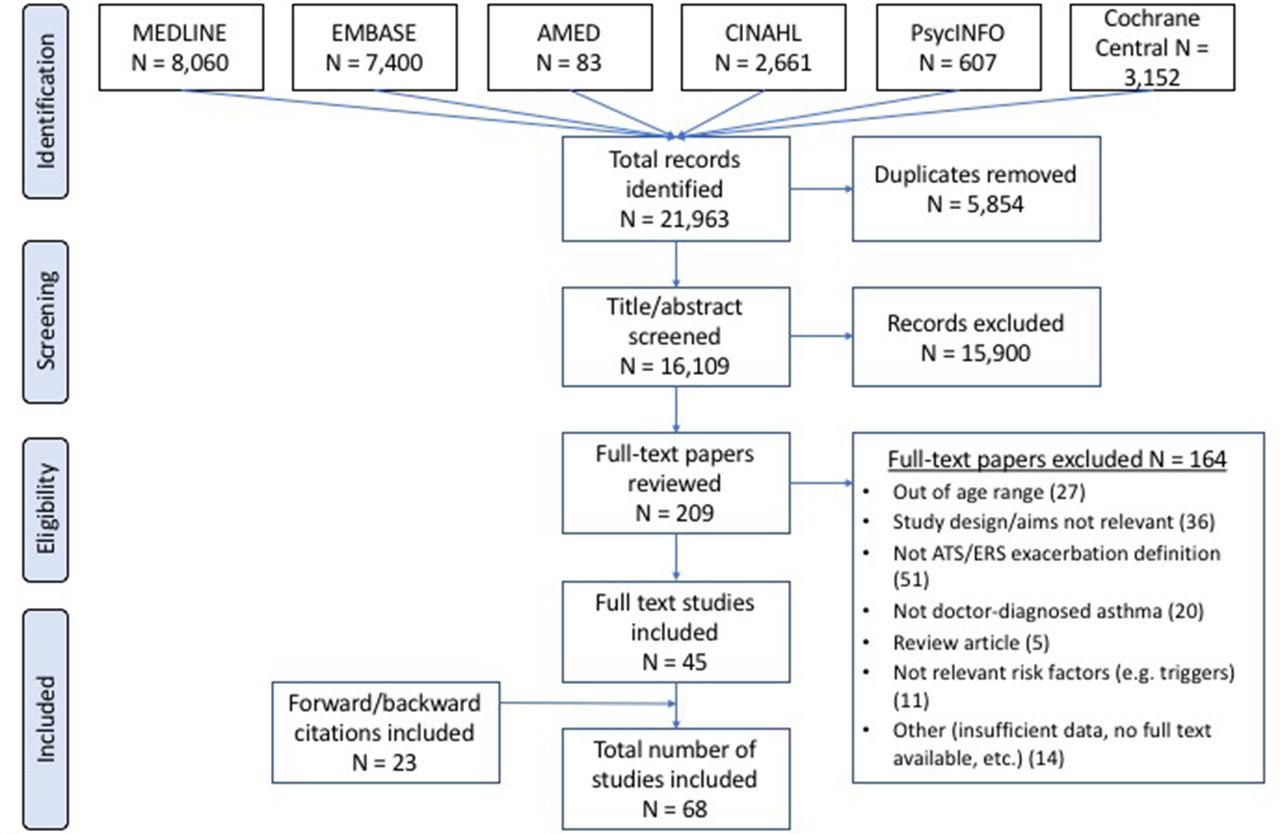
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. ATS, American Thoracic Society; ERS, European Respiratory Society.
Characteristics of studies
Of the 68 studies, 28 were cohort,18–47 4 were case-control48–51 and 36 were cross-sectional studies.52–85 Study size varied markedly from 38 participants with severe asthma in a study from the Netherlands20 to 6.7 million participants in a US census-based study.77 The studies came from 10 countries: 53 were based in the USA,18 19 21–24 27 28 30–46 49 51–54 57–61 63 65 66 68 70 71 73 74 76–78 80–84 86 5 in the Netherlands,20 29 47 48 64 3 in Puerto Rico,50 55 56 2 in Canada,26 62 and 1 each in Brazil,75 Chile,72 Costa Rica,69 France,67 Trinidad79 and the UK.25 Publication dates ranged from 199374 to 2017.18
The studies were heterogeneous on most characteristics, including population size, recruitment strategy, definitions of risk factors and attacks, and analytical approaches (confirming our decision that meta-analysis was not appropriate). Figure 2 shows how key variables are illustrated in the Forest plots.

Key variables and key to Forest plots. ED, emergency department.
Study quality varied (figures 3–6; online supplementary table S2). Most studies adjusted for at least age and gender, though 10 studies did not report adjusting for any potential confounders, reducing their quality score.28 45 47 62 67 79 81 83–85

Greatly increased risk: evidence for risk factors and weighting decisions. Note: The scale on all the Forest plots has been curtailed at an OR of 8 to enable comparison between the plots for the different factors. If the CIs are very wide, and the upper limit extends beyond the plot this is indicated with a line with an arrow. (95% CIs are given in online supplementary table S2 if required.) ED, emergency department.

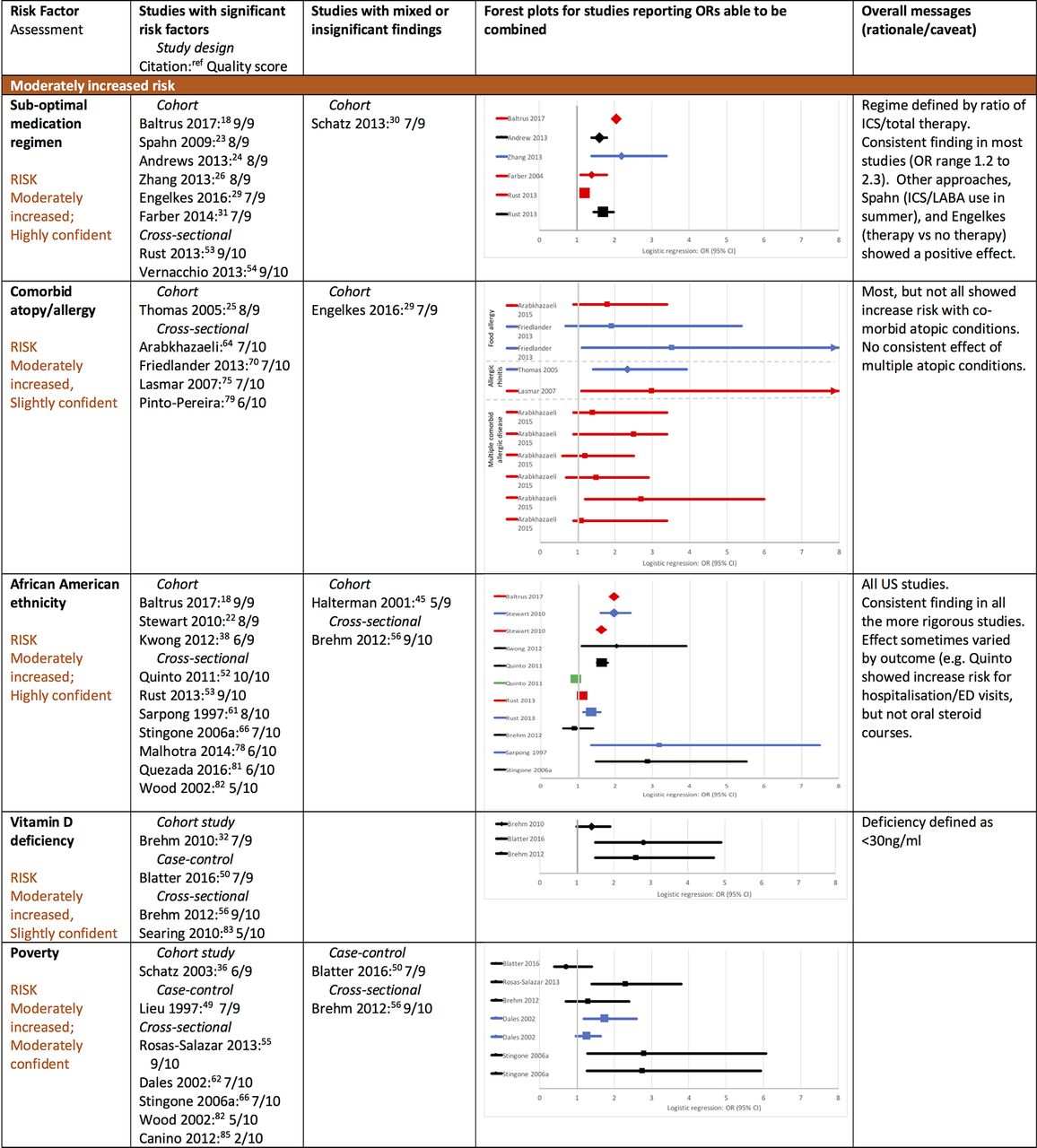
Moderately increased risk: evidence for risk factors and weighting decisions. Note: The scale on all the Forest plots has been curtailed at an OR of 8 to enable comparison between the plots for the different factors. If the CIs are very wide, and the upper limit extends beyond the plot this is indicated with a line with an arrow. (95% CIs are given in online supplementary table S2 if required.) ED, emergency department; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist.

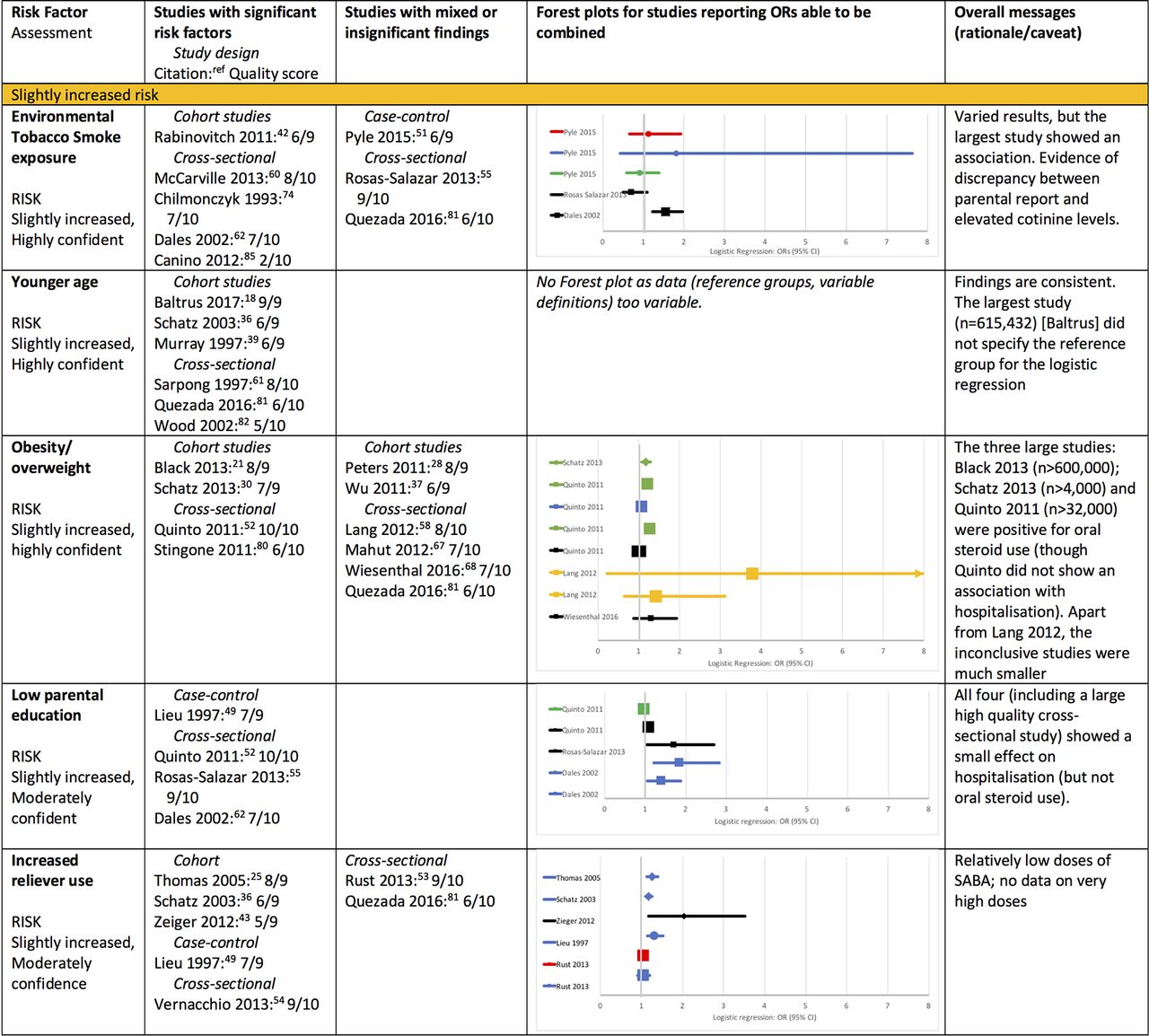
Slightly increased risk: evidence for risk factors and weighting decisions. Note: The scale on all the Forest plots has been curtailed at an OR of 8 to enable comparison between the plots for the different factors. If the CIs are very wide, and the upper limit extends beyond the plot this is indicated with a line with an arrow. (95% CIs are given in online supplementary table S2 if required.) SABA, short-acting beta2 agonist.

No increased risk, confounded and inconclusive factors: evidence for weighting decision. Note: The scale on all the Forest plots has been curtailed at an OR of 8 to enable comparison between the plots for the different factors. If the CIs are very wide, and the upper limit extends beyond the plot this is indicated with a line with an arrow. (95% CIs are given in online supplementary table S2 if required).
Overview of results
There were 33 risk factors identified, covering asthma disease status, medication use, allergy/atopy, social context, care and services, environment, and demography. Online supplementary table S2 is the full weighting table containing detailed information about populations studied, definitions used and analyses performed grouped by risk factor. Online supplementary table S3 summarises the data for each risk factor (including Forest plots of ORs where there were sufficient data) and the rationale for the weighting decisions. Figures 3–6 summarise the two detailed supplementary tables including simplified Forest plots. The text below synthesises the findings and weighting for each risk factor.
The overarching risk assessment is illustrated in a bubble plot (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of risk factors and weighting. ETS, environmental tobacco smoke; ICS, inhaled corticosteroid; SABA, short-acting beta2agonist.
Greatly or moderately/greatly increased risk of attacks (figure 3)
Previous attacks (n=11)
Previous attacks were consistently associated with a greatly increased risk of future attacks (ORs between 2.0 and 4.1).25 27 29 35–37 43 44 69 81 84 Due to the consistency of findings and quality of the studies the Panel was highly confident in this assessment (figure 3).
Poor control and/or persistent symptoms (n=11)
Ten studies had at least one significant result demonstrating that poor control or persistent symptoms identified a child at moderately/greatly increased risk of future attacks (ORs between 1.4 and 7.8).20 27 38 41 49 62 65 69 75 85 The exception was a small (n=165), short duration (3 months) cohort study of moderate quality which showed no association.45 The Panel was highly confident in this assessment. Persistent symptoms of any severity (as opposed to intermittent symptoms) were associated with greater risk.27 38 45 65 69
Poor access to healthcare (n=5)
Five studies examined access to healthcare defined by insurance status. Four demonstrated that poor access to healthcare was associated with a moderately/greatly increased risk of attacks.61 65 82 85 A small cohort study of moderate quality demonstrated no increased risk in children with or without Medicaid (a US social welfare programme).45 The Panel was moderately confident in this assessment. The studies were all US based with participants from deprived inner-city populations: one study controlled for ethnicity and poverty.65
Moderately increased risk of attacks
Suboptimal drug regimen (n=9)
Five of the seven studies that examined high reliever (short-acting beta2 agonist (SABA)) use showed a positive association with risk of attacks.25 36 43 49 54 The increased risk was judged to be slight (ORs between 1.2 and 1.3 in the three larger studies25 36 49), though none of the studies assessed very high levels of SABA use (figure 4).
Paradoxically, controller medication use was associated with an increased risk of attacks, as clinicians followed guideline recommendations and prescribed inhaled corticosteroids to children with poor control and previous exacerbations (‘confounding by indication’). Sixteen studies were included in this category: nine were suggestive of confounding by indication,25 29 48 50 53 55 56 59 81 four demonstrated fewer exacerbations with controller use18 35 36 84 and three showed no effect.31 65 69
The most sensitive marker of moderately increased risk was the ratio of controller-to-total medication. Suboptimal regimens were typically defined (in accordance with Healthcare Effectiveness Data and Information Set criteria86) as a ratio of the number of prescriptions for controller medication to total number of prescriptions for asthma medication <0.5. Six of seven studies that used this marker showed a significant relationship between a suboptimal regimen and asthma attacks (ORs between 1.2 and 2.318 24 26 31 53 54). In other approaches, two large, high-quality cohort studies showed an association with use of regular medication and fewer attacks.23 29 Thus, the Panel considered that a suboptimal regimen was associated with moderately increased risk, and were highly confident in their assessment.
Comorbid atopic/allergic diseases (n=6)
Two large, high-quality cohort studies analysed primary care records from the UK25 and the Netherlands.29 The UK study found comorbid allergic rhinitis increased the odds of hospitalisation by 2.3 (95% CI 1.4 to 3.9),25 whereas the Netherlands study found no increased risk of attacks in children with comorbid eczema (RR 0.8, 95% CI 0.4 to 1.4), allergic rhinitis (RR 0.8, 95% CI 0.5 to 1.2) or conjunctivitis (RR 1.4, 95% CI 0.7 to 2.7) compared with no comorbid allergic disease.29
The remaining four cross-sectional studies all demonstrated at least one positive association between comorbid atopic/allergic conditions and risk of attacks though CIs were wide.64 70 75 79 The Panel concluded that that there was a moderately increased risk of attacks with comorbid atopic/allergic disease, but they were only slightly confident in this assessment.
African-American ethnicity (n=12)
Twelve US-based studies examined the association between African-American ethnicity/‘race’ and the risk of attacks.18 22 38 45 52 53 56 61 65 78 81 82 Of the 12 studies, 10 reported at least one significant result demonstrating an increased risk of attacks in African-Americans compared with white or ‘non-black’ children (ORs between 1.6 and 4.1).18 22 38 52 53 61 65 78 81 82 The exceptions were a study that assessed the impact of African ancestry in a Puerto Rican population,56 and a small cohort study.45
Six of these studies demonstrated that the increased risk in African-Americans persisted after controlling for deprivation and/or poverty,60 65 area of residence,61 healthcare provision22 38 53 61 65 or parental education.52 Two studies compared risk in Black and Hispanic populations22 52: the risk was considerably less in Hispanic populations. Overall, the Panel was highly confident that African-American ethnicity was associated with moderately increased risk of asthma attacks.
Vitamin D deficiency (n=4)
Three small studies showed a significant association between vitamin D insufficiency (vitamin D <30 ng/mL) and acute attacks (ORs between 2.2 and 2.8),50 56 83 though a larger (n=1024) cohort study found only a borderline effect (OR 1.4, 95% CI 1.0 to 1.9).32 Thus, the Panel was slightly confident that vitamin D deficiency was associated with a moderately increased risk of attacks.
Poverty (n=9)
Nine studies examined the effects of poverty (variously defined as annual family income <US$15 000; <US$20 000; <US$40 000; receiving benefits) on risk of attacks in children with asthma. Seven studies had at least one positive association between risk of attacks and poverty level (ORs between 1.4 and 2.8).30 49 55 62 65 82 85 The exceptions were two small Puerto Rican studies.50 56 The Panel was moderately confident that poverty moderately increased risk of attacks.
Slightly increased risk of attacks
ETS exposure (n=8)
Five studies found at least one positive association between ETS exposure and asthma attacks.42 60 62 74 85 One high-quality cross-sectional study highlighted that the association between cotinine levels and risk of attack was lost when parent report was used to estimate ETS.60 Of note, the three negative studies relied on parental report.51 55 82 The Panel was highly confident that ETS exposure was associated with a slightly increased risk of asthma attack (figure 5).
Younger age (n=6)
All six of the studies that examined the effect of age on risk of asthma attacks found that younger children (within the 5–12 age range) were more likely to have an attack.18 36 39 61 81 82 The ORs ranged from 0.8 to 1.0 (indicating slightly decreased risk as age increased); the Panel was highly confident of this.
Overweight/obesity (n=10)
Four studies (including three very large high-quality studies) showed a significant, though small association between overweight or obesity and increased risk of attacks.21 30 52 80 The Panel was highly confident that there was a slightly increased risk of an attack in overweight or obese children.
Low parental education (n=4)
All four studies,49 52 55 62 including one large, high-quality cross-sectional study,52 showed slightly increased risk of attacks in children of families with low parental education level (ORs between 1.1 and 1.9). The Panel was moderately confident in this assessment.
No effect on risk of attacks
Gender (n=14)
Two studies found girls at an increased risk of attacks,52 53 and three found boys at increased risk18 60 65; the other nine studies showed no gender difference.29 36 38 45 61 62 77 81 85 Thus, the Panel was highly confident that the child’s gender had no effect on risk of attacks (figure 6).
Hispanic population (n=9)
Overall, the findings in the US Hispanic population were inconsistent; with the majority of studies demonstrating no increased risk,38 60 63 or inconsistent risk across the outcome measures used.52 Four studies showed a small increased risk18 22 82 (one with very wide CIs65) and one showed a reduced risk of emergency department visits.53 The Panel thus concluded that overall there was no increased risk, but their confidence in this assessment was only moderate.
Urban residence/proximity to major roads (n=6)
One case-control study showed a small increased risk of attacks in children living very close to a major road.50 The other five studies45 53 57 61 73 were negative including two large, high-quality cross-sectional studies, which controlled for a broad range of confounders.53 57 The Panel was slightly confident in their assessment of no effect.
Confounded by severity
Controller medication use, nebuliser use, ownership of written asthma action plans and routine asthma reviews were all associated with increased risk of attacks and were considered by the panel to be confounded by severity. (For details see online supplementary tables S2 and S3).
Insufficient evidence to draw a conclusion
For 12 factors we found inconclusive/insufficient evidence to draw a conclusion. These are listed at the end of figure 6; details about why the data were considered to be inconclusive/insufficient are provided in online supplementary table S3, with full description of all the studies in online supplementary table S2.
Discussion
Main findings
This systematic review aimed to identify factors which would identify children aged 5–12 years with asthma who are at increased risk of acute attacks. The child who had a history of previous attacks and persistent asthma symptoms was at greatly increased risk of a future attack, especially if they had poor access to care. Other key markers of moderately increased risk were a suboptimal drug regimen, comorbid atopic/allergic disease, African-American ethnicity, poverty and vitamin D deficiency. Younger age, exposure to ETS, being overweight and low parental education were associated with a slightly increased risk, but gender, urban residence and Hispanic ethnicity were not associated with increased risk.
Strengths and limitations
Despite our wide-ranging search strategies, we may not have identified all significant risk factors. Nevertheless, we identified papers related to almost all the predictors suggested by guidelines and experts in the field, lending face validity to our findings. The main omissions were that preterm delivery and eosinophilia were suggested, but not investigated as risk factors in any of the studies that we identified. That an additional 23 studies were found during forward and backward citations demonstrates the challenge in developing a comprehensive, but manageable, search strategy in such a broad area. There were some factors about which we found very little evidence and were thus unable to reach a conclusion (eg, comorbidities, parental health, FENO testing); lack of evidence, however, does not mean they are not significant factors. We excluded factors not available in routine clinical practice (eg, novel biomarkers87) which means that our conclusions are immediately transferable to contemporary clinical practice. The overweight of data from the USA (78% of studies included) limits the generalisability of the evidence for some factors (eg, ethnicity, poverty, access to healthcare) which may not be directly transferrable to other healthcare contexts.
The heterogeneity of the studies in terms of definitions of attacks (hospitalisations, emergency department visits, unscheduled GP care, oral steroids courses), thresholds applied to predictors (eg, definitions of persistent/severe symptoms, income levels associated with poverty, objective or reported assessment of ETS), duration of follow-up, provenance of data (collected for research or routine data) as well as study design and analysis precluded meta-analysis. To reduce potential subjectivity, we adopted a rigorous approach to weighting the factors using an Expert Panel’s consensus to define initial weightings and a multidisciplinary end-of-project workshop at which the findings were discussed, refined and agreed. This breadth of internationally recognised professional experience (although all UK based) assisted the interpretation of our findings and lends credibility to our conclusions.
Implications for parents and clinical practice
Our findings suggest that it is possible to identify the ‘high-risk’ child with asthma. The factors associated with moderately or greatly increased risk are easily identifiable in routine practice. For example: a history of acute attacks, persistent troublesome symptoms, frequency of prescription requests and comorbid atopic/allergic conditions are recommended components of regular reviews,6 7 88 and knowledge of the social context is a core component of family medicine practice.89 90
Identifying that their child is ‘at-risk’ enables parents to take decisions about modifying risk, such as reducing exposure to ETS, and reconsidering the necessity for controller treatment against their concern about harms of regular medication.91 Clinicians alerted to the ‘at-risk’ child can target care, specifically instituting evidence-based management (regular controllers6 7; supported self-management92) to reduce risk.
Implications for healthcare systems and policymakers
Poor access to care and living in poverty were important risk factors that should be targeted by policymakers and health service planners to reduce risk of acute attacks in children living in high-risk populations. At a public health level, strategies for reducing smoking93 and targeting the growing epidemic of obesity in children21 will also contribute to reducing risk. In the USA, people from African-American communities living in deprived communities are at particular risk.
Implications for future research
Formal prognostic modelling is needed to validate the risk factors identified in this review,94 and future research should assess whether risk assessment based on these factors improves outcomes when used prospectively in routine clinical practice. Nearly three-quarters of the studies in this review were performed in a US setting. Research is needed to understand the impact of variables such as poverty, urban/rural living, ethnicity and different rates of state/private/no medical insurance in other contexts.
Conclusion
It is possible with the information available in routine clinical practice to identify a child who is at increased risk of an acute attack. Many of the risk factors are potentially modifiable by parents acting to eliminate ETS or adhere to regular controller medication, by clinicians offering evidence-based treatment and self-management support, by healthcare systems ensuring equitable access to care and by policy initiatives addressing social deprivation and the public health challenges of smoking and obesity.
Acknowledgments
We thank Marshall Dozier (Academic Support Librarian) for
help with the search strategy, and Dr John Blakey for practical advice in the early stages.
References
Footnotes
Contributors HP led the development of the protocol, securing of funding, study administration, expert panel, workshop and writing of the paper. AS, SJ, AB, JH and MS contributed to the development of the protocol. SJ provided statistical advice. AudB and SMcL undertook the screening, data extraction and presentation of results. HP, JYP, JH, MS, AudB and JFK formed the expert panel. All authors contributed to the interpretation of the findings. AudB wrote the initial draft of the paper with SMcL and HP, to which all the authors contributed. HP is the study guarantor.
Funding This research was supported by Asthma UK (Ref: AUK-SR-2015-01), with contributions from the Asthma UK Centre for Applied Research (AUK-AC-2012-01). AS is supported by the Farr Institute which is funded by a consortium of funders headed by the MRC.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are provided in the manuscript and online supplementary tables.
Collaborators The ARC group members: Helen Benson; Steve Cunningham; Victoria Dalgliesh; Gwyneth Davies; Melissa Goodbourn; Susan Grieve; Jonathan Grigg; Hayley K Zislis; Erin McDonnell; Susan Morrow; Meagan Peterson; Daniel Russell; Jurgen Schwarze; San Selveindran; Nara Tagiyeva; Mike Thomas; Marissa Ware; Andrew Wilson.