Article Text

Abstract
Background A range of questionnaires have been used to assess health-related quality of life (HRQOL) in bronchiectasis. A systematic review was conducted to evaluate their psychometric properties and assess associations between HRQOL and clinical measures.
Methods Five electronic databases were searched. Studies eligible for inclusion were those that investigated the validity of HRQOL questionnaires and/or their association with other outcomes in adults with bronchiectasis. Patients with cystic fibrosis were excluded. The identified questionnaires were assessed for convergent, discriminant and cross-cultural translation validity; missing data, floor and ceiling effects, internal consistency, responsiveness and test-retest reliability. A meta-analysis was conducted to estimate the strength of associations between HRQOL and clinical measures.
Results From 1918 studies identified, 43 studies were included in the systematic review, of which 38 were suitable for the meta-analysis. Nine HRQOL questionnaires were identified, with the most widely used being: St George's Respiratory Questionnaire, Leicester Cough Questionnaire, Quality of Life–Bronchiectasis and Short Form-36. HRQOL questionnaires had moderate to good internal consistency and good test-retest reliability. Only 8 of 18 studies that used translated HRQOL questionnaires reported or referred to the validity of the translated questionnaire. There was a stronger correlation (mean r (95% CI)) between HRQOL and subjective outcome measures, such as dyspnoea (0.55 (0.41 to 0.68)) and fatigue (0.42 (0.23 to 0.58)) compared with objective measures; exercise capacity (−0.41 (−0.54 to −0.24)), FEV1% predicted (−0.31 (−0.40 to −0.23)) and extent of bronchiectasis on CT scan (0.35 (0.03 to 0.61)); all p<0.001.
Conclusions This review supports most HRQOL questionnaires used in bronchiectasis have good psychometric properties. There was a weak to moderate association between HRQOL and objective outcome measures. This suggests that HRQOL questionnaires assess a unique aspect of health not captured by objective measures.
- Bronchiectasis
Statistics from Altmetric.com
Key messages
What is the key question?
Which health-related quality of life questionnaires are used in bronchiectasis and what is the evidence for their validity?
What is the bottom line?
Despite differences in the construct of frequently used questionnaires St George's Respiratory Questionnaire, Leicester Cough Questionnaire and Quality of Life—Bronchiectasis, there is good evidence to support their validity, internal reliability and repeatability.
Why read on?
This article provides an in-depth review of the evidence for the validity of health-related quality of life questionnaires and their association with commonly used clinical outcome parameters; this may help investigators select the most appropriate tool for their purpose.
Introduction
The assessment of health-related quality of life (HRQOL) is important in chronic disease as it evaluates the overall impact on health from the patient’s perspective. HRQOL is defined as ‘the perception of the impact of health on an individual's contentment or satisfaction with life in areas they consider important’.1 Bronchiectasis is a persistent or progressive condition characterised by dilated thick-walled bronchi.2 Symptoms of bronchiectasis include sputum production, cough, haemoptysis, dyspnoea and fatigue, which are worse during exacerbations. HRQOL is impaired in bronchiectasis.3 A range of tools have been used to assess HRQOL in bronchiectasis. These include generic tools such as the Medical Outcomes Study 36-Short Form Health Survey (SF-36), organ-specific tools such as the St George's Respiratory Questionnaire (SGRQ) and Leicester Cough Questionnaire (LCQ) and the condition-specific Quality of Life-Bronchiectasis (QOL-B).4–7 The comparative validity of HRQOL questionnaires used to assess bronchiectasis has not been investigated; such a review may inform investigators and clinicians about the choice of HRQOL questionnaires available and their validity. The aim of this systematic literature review was to evaluate the psychometric properties of questionnaires used to assess HRQOL in bronchiectasis. This included a meta-analysis to assess the associations of HRQOL with other clinical measures.
Methods
Study eligibility criteria
The inclusion criteria were: empirical studies of adult patients (≥18 years old) with bronchiectasis, studies reporting the psychometric properties of generic and disease-specific HRQOL questionnaires, and/or the association of HRQOL with other clinical measures. The diagnosis of bronchiectasis was established using clinical and/or radiological features. The review was limited to studies reporting in English language. Studies investigating acute exacerbations were included if they met the inclusion criteria. Studies investigating mixed populations such as adult/paediatric and non-cystic fibrosis/cystic fibrosis bronchiectasis were included if the findings reported were distinguishable by age/disease category. The exclusion criteria were: diagnosis of cystic fibrosis and review articles (used only to identify further references). Studies using cognitive interview or focus group methodology that did not include HRQOL questionnaires were also excluded.
The psychometric properties considered included convergent and discriminant validity (relationship with other clinical measures according to expectations), internal consistency (Cronbach's α coefficient: extent to which the items of a questionnaire are inter-related), test-retest reliability (repeatability during a clinically stable period), responsiveness (response to change using standardised response mean, SRM), missing data, floor (minimum score) and ceiling (maximum score) effects. The validity of translated HRQOL questionnaires was evaluated by assessing if forward/backward translation, cognitive interviews, internal consistency and reliability were reported.
Search strategy and terms
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and Scottish Intercollegiate Guidelines Network (SIGN) methodology checklist for systematic reviews and meta-analyses were used.8 ,9 The search was conducted in five electronic databases: Embase (1974–2014), Pubmed, Medline (Ovid, 1946–2014), PsycINFO (1806–2014) and Cochrane Library. The keywords for search were: non cystic fibrosis bronchiectasis/bronchiectasis, quality of life/QOL/HRQOL, health status, well-being, daily living, questionnaire, validation/validity, psychology and psychometrics. The search was repeated with additional keywords that included named HRQOL questionnaires identified in the previous search. The date of search was 6 November 2014. The references from all included manuscripts were used to identify further studies. Abstracts with adequate information about study methods and results were considered for inclusion.
Study selection, data extraction and quality assessment
After duplicate references were removed, two reviewers independently assessed the studies (in abstract form) against the inclusion criteria. When there was insufficient information available in the abstract, the full text was reviewed. Discrepancies between the reviewers were resolved through discussion and consensus. Two investigators then extracted data from the selected studies including: author, year of publication, aim of the study, sample size, most common aetiology of bronchiectasis, age, gender, FEV1% predicted, HRQOL questionnaire used and psychometric properties of HRQOL questionnaire including correlation of HRQOL with other clinical measures. Clinical measures used for convergent and discriminant validity of HRQOL included those that assessed symptoms, anxiety, depression, exercise capacity, lung function and other physiological parameters and markers of disease severity and infection/exacerbation. The quality of studies was assessed using a critical appraisal tool developed by Swigris et al1 and modified for bronchiectasis (see online supplementary appendix 1). Where translated questionnaires were used, the translation procedure was assessed by evaluating the included study and related references for forward-backward translation, cognitive interviews, floor and ceiling effects, internal consistency and test-retest reliability.
The minimal clinically important difference (MCID), the smallest change in an HRQOL questionnaire score that is deemed important by patients, was identified if available for patients with bronchiectasis. Studies reporting MCID for questionnaires in other chronic respiratory disorders were presented if data was unavailable for bronchiectasis, following an additional literature search. Responsiveness of the included questionnaires was assessed from randomised-controlled trials returned in our search, by calculating the SRM when possible for the total sample population, and treatment and placebo groups individually. Clinical trials were otherwise excluded from the systematic review unless the primary purpose was to study the psychometric properties of HRQOL questionnaires.
Statistical analysis
Quantitative analysis was performed with Stata V.12.0 (StataCorp LP, Texas, USA) and MetaWin V.2.0 (Baker Hughes, Houston). Internal consistency was reported as Cronbach's α coefficient (acceptable if >0.7) and test-retest reliability as intraclass correlation coefficient (ICC) (moderate if=0.5–0.7 and good if >0.7). Meta-analysis was performed to evaluate the association between HRQOL and clinical measures when data was available from at least two studies. When multiple questionnaires were used to assess HRQOL in the same study, the most relevant questionnaire to bronchiectasis was used in the meta-analysis. When the total score was not available, the mean of the domain scores was used. When the data were repeated in multiple publications, the meta-analysis included the publication with the largest sample size that best met the inclusion criteria.
Correlation coefficients were extracted from the studies when available. The strength of association was categorised as following: weak r<0.4, moderate r=0.4–0.7 and strong r>0.7; significance p<0.05. When only p values and other metrics (t values, Cohen's d, F values, χ2 values) were available, correlation coefficients were obtained according to formulas suggested by Rosenthal et al.10 A detailed description of correlation coefficients and Fisher's Z calculations is given in online supplementary appendix 2. SRMs were calculated when data was available from mean difference in HRQOL scores (pre/post intervention)/SD of the difference (trivial effect <0.20, small effect=0.20–0.50, moderate effect=0.50–0.80 and large effect >0.80). Standard formulae for computing SD were used when values were not directly available.11 Publication bias was assessed using funnel plots and Rosenthal's fail-safe number (Rosenthal's N),12 online supplementary appendix 2.
Results
Study characteristics
Study selection
The search retrieved 1918 publications (see online supplementary table E1). Two additional abstracts and a full manuscript were added manually from searching references.13–15 A PRISMA flow chart illustrates the studies selection process and reasons for exclusion (figure 1). Forty-three studies met the inclusion criteria for systematic review, of which 38 were included in the meta-analysis of associations between HRQOL and other clinical measures. Studies with multiple publications were combined and considered as single publications. Five studies had subjects who overlapped with those in other publications (table 1).
Characteristics of studies included in the literature review

PRISMA flow chart of the literature review and meta-analysis selection process. HRQOL, health-related quality of life.
Overview of included studies and study quality
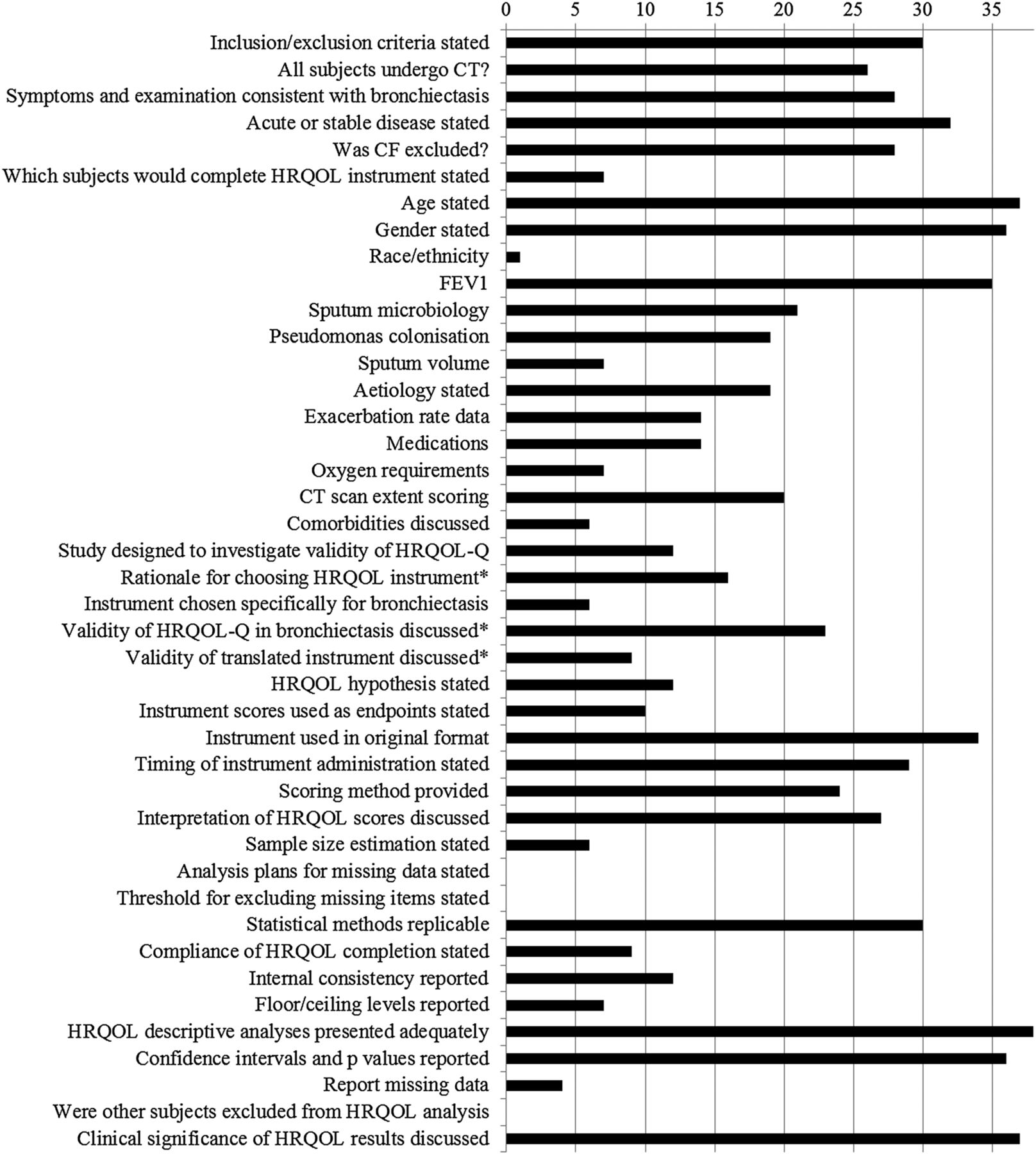
The objectives of the included studies are presented in table 1. All studies were prospective. They all reported cross-sectional findings apart from one,16 while nine studies also included longitudinal findings for the investigation of repeatability of the HRQOL questionnaires.5–7 ,14 ,17–21 Nine studies were published in abstract form (indicated in reference list and online supplementary material). The studies met a mean (SD) of 48 (14) % of the quality criteria; range 17–78% (figure 2). No study met the criteria for all quality domains.

Estimated quality of reporting for included studies. x axis: number of studies meeting each quality criterion (total n=43), y axis: quality criterion item.
Number of total evaluable studies 43 except where indicated as*. CF, cystic fibrosis; CT, computed tomography; HRQOL, health-related quality of life; HRQOL-Q, health-related quality of life questionnaire.
Characteristics of patients
Table 1 presents the clinical characteristics of patients. The studies included a total number of 3727 patients with bronchiectasis (median number of patients with bronchiectasis per study 98, range 6–608). The mean study patient age was 59 (range 43–70) years and 64 (range 37–83) % of the patients were female. Three studies also recruited participants during an exacerbation,22–24 while all remaining studies recruited patients during a clinically stable phase. Eight studies did not report CT scan findings.13 ,14 ,22 ,25–29
HRQOL questionnaires
Overview of HRQOL questionnaires
Seven organ/disease-specific and two generic HRQOL questionnaires were identified in the selected studies (table 1). Fifteen studies administered multiple HRQOL questionnaires. Twenty-seven studies used the SGRQ, nine the LCQ, eight the SF-36, six the QOL-B V. 2.0 or V.3.0, two the Chronic Respiratory Disease Questionnaire, two the generic Euro Quality of Life and one each of the COPD assessment tool (CAT), the 20-Item Sinonasal Outcome Test and the Cough Quality of Life Questionnaire. A description of these HRQOL questionnaires is given in online supplementary appendix 3, including their length, administration and scoring. All questionnaires were originally developed in English. A summary of average HRQOL scores from studies, where available, is presented in online supplementary table E2.
Validity of translated questionnaires
Eighteen studies used a translated HRQOL questionnaire and only eight reported or referenced a validation of the translated questionnaire (see online supplementary appendix 4).
Floor/ceiling effects and missing data
Floor and ceiling effects and missing data were reported for only two HRQOL questionnaires, SGRQ and QOL-B and were relatively small for most total and domain scores (see online supplementary appendix 5).
Internal consistency
Cronbach's α coefficients for the HRQOL questionnaires ranged from moderate to high (table 2). The LCQ had the highest internal consistency (Cronbach's α coefficient 0.91–0.94).14 QOL-B Cronbach's α coefficients ranged from 0.65 to 0.96,6 ,20 ,21 SGRQ from 0.59 to 0.92,5 ,17 ,30 SF-36 from 0.75 to 0.9131 and for CAT it was 0.84.32 The internal consistency of other questionnaires was not reported.
Internal consistency and test-retest reliability of HRQOL questionnaires in non-cystic fibrosis bronchiectasis
Test-retest reliability
Test-retest reliability data were available for SGRQ, QOL-B and LCQ. ICC was moderate to high (table 2). The SGRQ was slightly more repeatable over 2 weeks than the QOL-B (ICC range 0.89–0.97 vs 0.67–0.88, respectively).5 ,6 ,17 ,20 ,21 ,33 The LCQ was highly repeatable over 6 months (ICC=0.96).7
MCID and responsiveness
MCID in bronchiectasis was reported only for the QOL-B questionnaire, range 7–10 units.21 ,33 MCID for HRQOL questionnaires in other chronic respiratory diseases is presented in online supplementary table E3. Twenty randomised-controlled trials included sufficient data to assess responsiveness; there was a wide range of SRMs from trivial to large (see online supplementary table E4).
Discriminant ability of HRQOL questionnaires
SGRQ was able to discriminate between subjects based on the severity of dyspnoea5 ,30 and wheeze,5 sputum volume,17 ,30 CT scan extent of bronchiectasis,34 exacerbation frequency,5 ,30 ,35 sputum colonisation by Pseudomonas aeruginosa,30 history of haemoptysis in the past year21 and the bronchiectasis severity index.35 SGRQ total scores were able to discriminate FEV1% categories.30 There were conflicting data for the discriminative ability of the QOL-B based on FEV1%. The number of QOL-B domains reported in studies as able to discriminate patients on the basis of FEV1% ranged from one to all eight domains.6 ,21 ,33 QOL-B was however able to discriminate between patients according to CT scan extent of bronchiectasis and sputum Pseudomonas aeruginosa and Haemophilus influenza colonisation.21
Associations between HRQOL and clinical measures: a meta-analysis
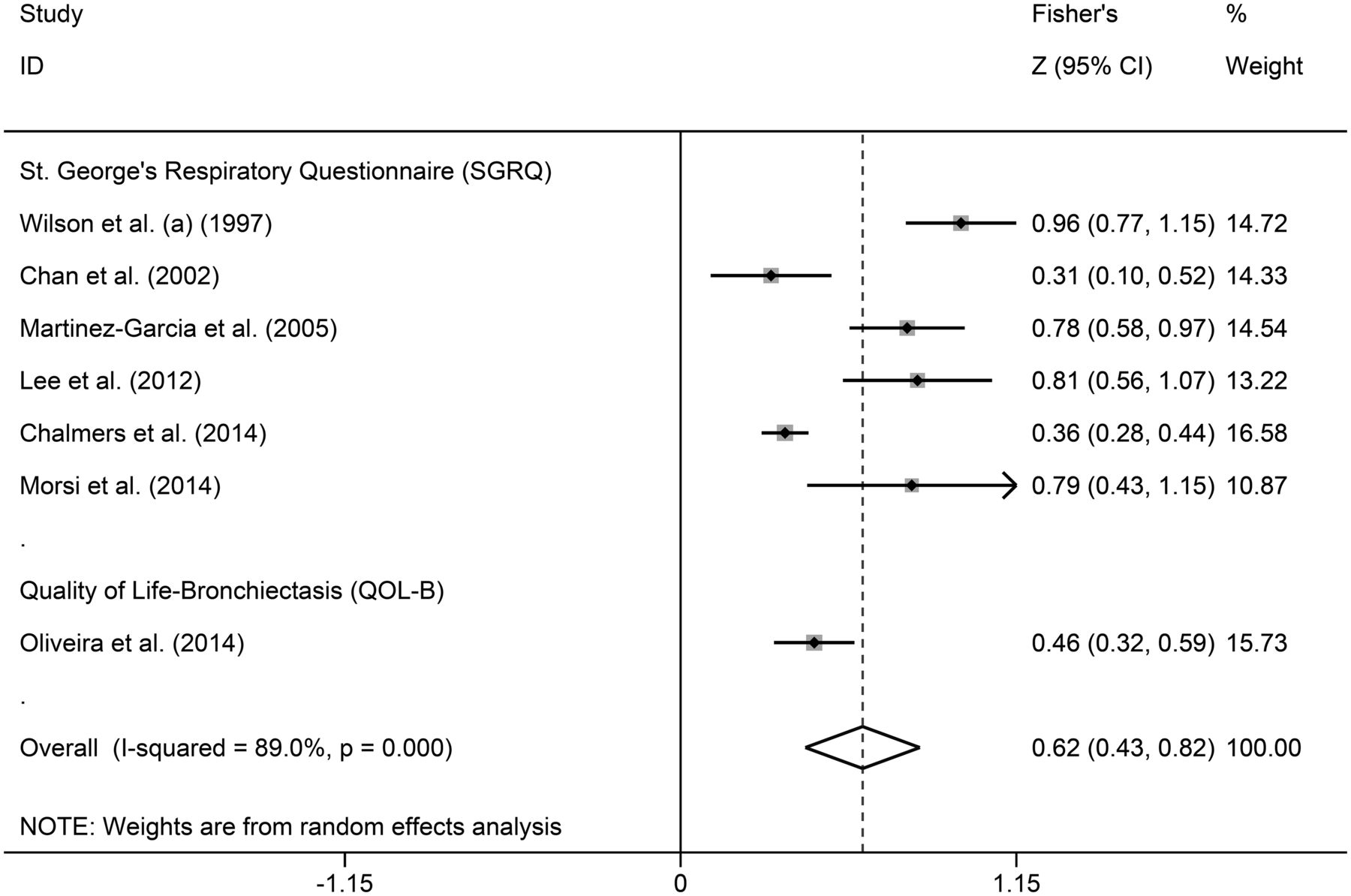
The associations between HRQOL and other clinical measures (convergent/discriminant validity) reported in studies were evaluated in a meta-analysis (table 3). The associations for clinical measures where only single studies were available are presented in online supplementary table E5. A wide range of associations between HRQOL and clinical measures were reported (see figures 3⇓⇓–6 and online supplementary figures E1–E14). The strongest associations of HRQOL were with dyspnoea (figure 3) and fatigue (see online supplementary figure E2) and for objective measures with exercise capacity (figure 4), where there were moderate correlations. The association with cough was r=0.56 with a p value approaching significance (p=0.06, only two studies), figure 5. There was a weak association between HRQOL and sputum volume (see online supplementary figure E4) and microbiological colonisation (see online supplementary figure E13), lung function (see figure 6 and online supplementary figure E11), exacerbation rate (see online supplementary figure E10) and extent of bronchiectasis on CT scans (see online supplementary figure E6). The association between HRQOL questionnaires ranged from weak to strong (see online supplementary appendix 6).
Meta-analysis: correlations reported for health-related quality of life with clinical measures

Forest plot for the correlation between health-related quality of life and dyspnoea.
Measurements of dyspnoea used: Medical Research Council (MRC) scale (Wilson et al, 1997; Martinez-Garcia et al, 2005; Lee et al, 2012; Chalmers et al, 2014; Oliveira et al, 2014), 12-point Borg scale (Chan et al, 2002) and dyspnoea-12 (Morsi et al, 2014).
Zero line: is illustrated to indicate the direction of association. A fisher’s z value >0 indicates positive association between the two variables. A fisher’s z value <0 indicates negative association between the two variables.
High score = poor health-related quality of life. Dashed line: represents the overall meta-analytic mean Z.
Arrow: indicates confidence interval limit.
Weight was calculated using the inverse variance weight formula [weight=i/sqrt(n-3)].

Forest plot for the correlation between health-related quality of life and exercise capacity.
Measurements of exercise capacity used: 6-minute walk test for all studies apart from one that used incremental shuttle walk test (Wilson et al, 1997) and another that used both (Lee et al, 2010). High score = poor health-related quality of life.
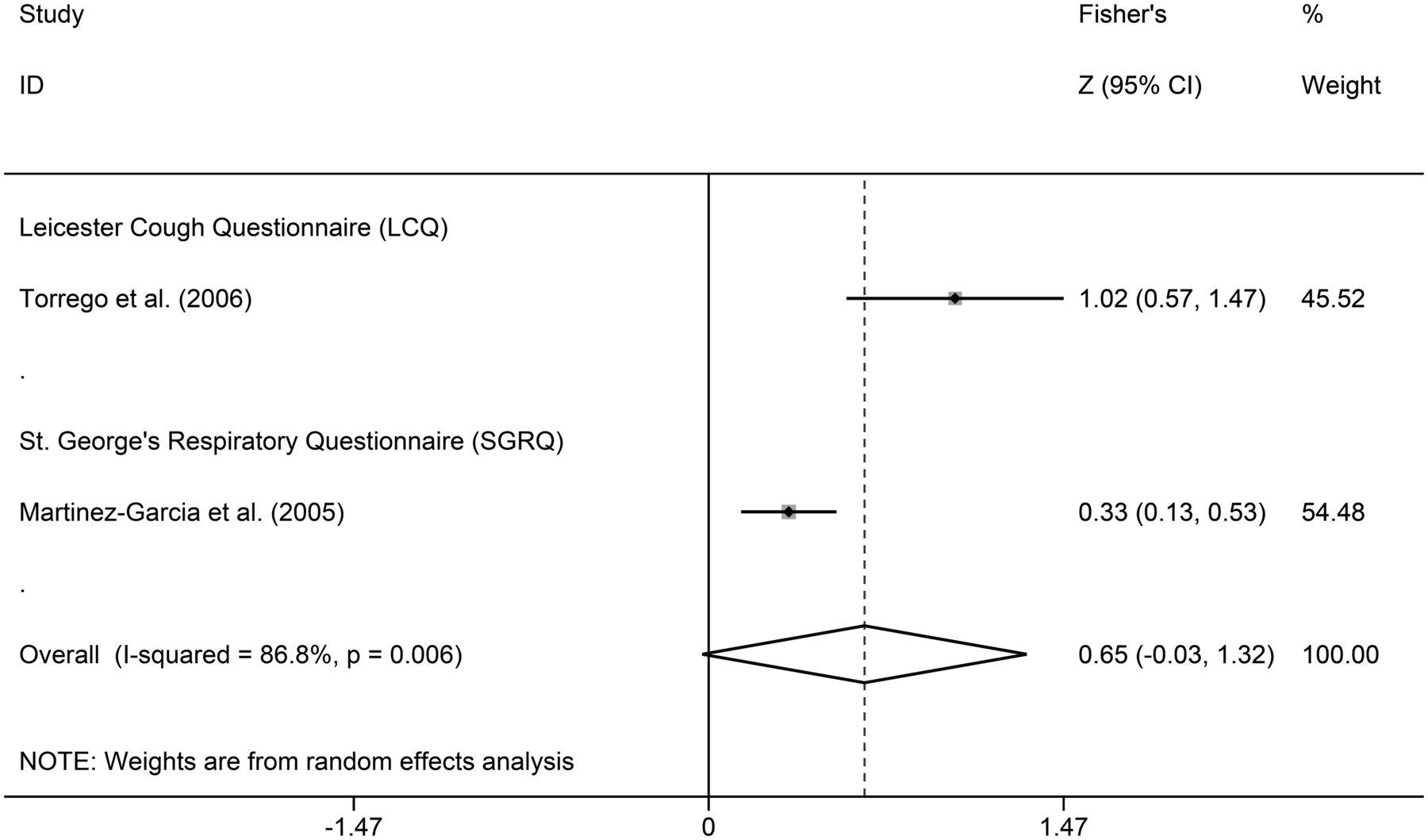
Forest plot for the correlation between health-related quality of life and cough.
Measurements of cough used: cough reflex sensitivity to capsaicin (Torrego et al, 2006) and patient-reported cough frequency (Martinez-Garcia et al, 2005). High score = poor health-related quality of life.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for the correlation between health-related quality of life and FEV1% predicted. High score = poor health-related quality of life.
Analysis of publication bias and heterogeneity
Publication bias was assessed with a funnel plot for FEV1% predicted and exercise capacity, as these were parameters with >10 studies available (see online supplementary figures E15 and E16). FEV1% resembled a symmetric image, suggesting no publication bias. Exercise capacity funnel had slight asymmetry suggesting possibility of publication bias. However, this was not confirmed with Enger's test (p=0.189).
Discussion
This is the first systematic review of the psychometric properties of HRQOL questionnaires used to assess bronchiectasis. The review included 43 studies that investigated 3727 patients and identified nine HRQOL questionnaires. For the assessment of the questionnaires, we used criteria recommended by the Food and Drug Administration guidelines.36 Our systematic review suggests that the identified questionnaires have generally good internal consistency, test-retest reliability and convergent validity. The SGRQ was the most widely studied questionnaire. This questionnaire was initially developed for COPD and asthma, but has subsequently been validated and used in a wide range of respiratory disorders. The next most commonly used tool was the LCQ, which was initially developed for patients with chronic cough, but has been validated in patients with bronchiectasis. The QOL-B, a recently published questionnaire, was the only questionnaire developed specifically for bronchiectasis.
We identified some relatively small differences in the psychometric properties between HRQOL questionnaires. The internal consistency was good for all questionnaires; the Cronbach's α coefficient was highest for LCQ. The test-retest reliability was high for the LCQ and SGRQ domains and variable for the QOL-B domain, ranging from moderate to good. The convergent validity was also variable for the clinical measures studied. The association with exercise capacity was marginally better with the SGRQ and LCQ questionnaires compared with QOL-B. The association between HRQOL with FEV1 was generally weak, irrespective of the questionnaire administered. The association with symptoms of dyspnoea was stronger with SGRQ compared with QOL-B. It is possible that the differences identified in the psychometric properties of questionnaires may reflect differences in the study population, disease characteristics and study methods. Studies that directly compare HRQOL questionnaires are needed to establish similarities and differences between questionnaires with greater confidence.
The responsiveness, MCID and translation validity of HRQOL questionnaires were also investigated. Based on randomised controlled trials, SRMs were variable. The MCID has only been reported for one HRQOL questionnaire in patients with bronchiectasis (QOL-B);33 ,37 further studies are needed to establish MCID of other widely used questionnaires. Many studies used translated HRQOL questionnaires. While there were good examples of translated HRQOL questionnaire validity in bronchiectasis, there were many studies where this procedure was either not conducted or reported. It is essential that HRQOL questionnaires are translated and validated using well recognised and standardised procedures to ensure that they are appropriately adapted to accommodate cultural differences.38
The assessment of convergent validity demonstrated a stronger relationship of HRQOL with subjective outcome measures compared with objective measures. The strongest association of HRQOL was with respiratory symptoms. The review also highlights a potentially important association between HRQOL and fatigue. Fatigue is a recognised symptom of bronchiectasis but its mechanism is poorly understood.27 There was a poor association between HRQOL and frequency of acute exacerbations. This may be because most studies assessed HRQOL during a clinically stable phase. The best identified association among objective measures was with exercise capacity, such as the 6-min walk test. This is not surprising, since exercise capacity is more likely to relate to functional ability than other objective outcome measures. Our findings highlight the discordance between patient-reported outcome measures and physiological measures, such as FEV1, and are consistent with findings for other chronic respiratory disorders, such as COPD.39 This suggests that HRQOL questionnaires assess a unique dimension of health, which is distinct from that assessed by objective measures. HRQOL measures should ideally complement objective clinical measures in the assessment of bronchiectasis.
There are some limitations with our systematic review. Our review is susceptible to publication bias (positive findings are more likely to be published compared with negative findings) and time lag bias (inability to identify ongoing or unpublished studies), as any review article. We did not contact the study authors to retrieve unpublished data, which may lead to overinterpretation of associations between HRQOL and clinical measures; this applies particularly to studies published in abstract form. We chose to limit the review to those studies specifically evaluating the psychometric properties of HRQOL questionnaires and associations with clinical measures. For the purpose of analysis, we grouped clinical measures together. We therefore may have underestimated important associations due to the heterogeneity of clinical outcome measures. We used the average of HRQOL domain scores when total scores were not reported. Other potential sources for heterogeneity were differences in inclusion/exclusion criteria, population and disease aetiology. The quality of HRQOL data and its reporting varied between studies. We assessed the quality of studies with a modified version of a tool developed by Swigris et al1 as this was the most comprehensive and relevant for our purpose. The included studies met an average 48% of the quality criteria assessed, which is similar to a systematic review of HRQOL in idiopathic pulmonary fibrosis.1 A greater proportion of studies met the quality criteria relating to description of patient demographics, the reporting of major clinical outcome measures of bronchiectasis and the analysis of HRQOL data. Fewer studies met the criteria for reporting details of the administration of the HRQOL questionnaires, floor/ceiling effects and missing data. It is therefore possible that the quality of studies and data-reporting may have compromised some of our findings. A greater clarity for HRQOL data-reporting is required in future studies including reporting of the rationale for choosing a particular instrument, mode of administration, details of missing data and sample size estimates. The questionnaires identified in this review have been in use for variable lengths of time. It is likely that this may have impacted on the availability of evidence.
Our review highlights the questionnaire options available. SGRQ is a good choice for a research study if extensive experience of use of an HRQOL questionnaire is important. SGRQ also has good psychometric validity and the strongest association with dyspnoea. Its disadvantage is that it is a long questionnaire and potentially may not be as responsive to change as disease-specific tools; this requires further study. LCQ is brief, well validated in bronchiectasis and may be particularly advantageous if cough is the symptom of primary focus. QOL-B is the only disease-specific questionnaire and has good psychometric properties. The disadvantage of QOL-B is that it is relatively long and does not have a total score that would simplify interpretation of data. SF-36 may be useful in comparative studies that include non-pulmonary disorders, as it is a generic tool. It is however a relatively long questionnaire and is not as extensively validated in bronchiectasis as some of the alternatives. There is a need for briefer tools with simplified scoring (ideally inclusive of a total score) for use in the clinical and research settings. The bronchiectasis severity index is one such example, although not a measure of HRQOL.35
In conclusion, HRQOL questionnaires used in bronchiectasis have generally good psychometric properties. There are some differences between questionnaires in their association with clinical measures. Investigators should select questionnaires for their study based on the ease of administration and the questionnaire's correlation with the primary health domain under investigation. More research is needed to investigate longitudinal changes in HRQOL and establish MCID of instruments.
Acknowledgments
The authors thank Mr A Drongitis for his assistance in screening papers for inclusion.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Konstantinos Fragkos at @costasfrangos
Contributors Conception: AS, RG, SSB; Study design: all authors; Data collection: AS, KCF; Analysis and interpretation: all authors; Writing of the manuscript: AS, SSB; Revision and approval of the manuscript: all authors.
Competing interests None of the authors has a financial relationship with a commercial entity that has an interest in the subject of this manuscript. AS is completing a PhD that was financially supported by Greek State Scholarships Foundation (IKY). SSB is a developer of HRQOL tools. RW and MRL were co-authors of studies included in the review.
Provenance and peer review Not commissioned; externally peer reviewed.