Article Text

Abstract
Background Fibred confocal fluorescence microscopy (FCFM) is a novel technology that allows the in vivo assessment and quantification during bronchoscopy of the bronchial wall elastic fibre pattern, alveolar and vessel diameters and thickness of the elastic fibre in the alveolar wall.
Aims To relate these structural characteristics with lung function parameters in healthy subjects, smokers with normal spirometry and patients with chronic obstructive pulmonary disease (COPD).
Methods We performed FCFM in 20 never smokers, 20 smokers with normal spirometry and 23 patients with COPD who required bronchoscopy for clinical reasons. The bronchial wall elastic fibre pattern was classified as lamellar, loose and mixed pattern, and later confirmed pathologically. Airspace dimensions and extra-alveolar vessel diameters were measured. Lung function measurements and pulmonary CT scans were obtained in all participants.
Results Patients with COPD were characterised by a significantly higher prevalence of loose fibre bronchial deposition pattern and larger alveolar diameter which correlated inversely with several lung function parameters (forced expiratory volume in 1 s (FEV1) , FEV1/forced vital capacity ratio, maximum expiratory flow, carbon monoxide transfer factor and carbon monoxide transfer coefficient; p<0.05). Increased alveolar macrophages were demonstrated in active smokers with or without COPD.
Conclusions This is the first FCFM study to describe in vivo microscopic changes in the airways and alveoli of patients with COPD that are related to lung function impairment. These findings open the possibility of assessing the in vivo effects of therapeutic interventions for COPD in future studies.
- Emphysema
Statistics from Altmetric.com
Key messages
What is the key question?
-
Are the relationships between the ex vivo structural changes and lung function that characterise Chronic Obstructive Pulmonary Disease (COPD) reproducible in vivo using a novel endoscopic microscopy view?
What is the bottom line?
-
Fibered confocal fluorescence microscopy (FCFM) is a novel technology that allows the in vivo assessment and quantification during bronchoscopy of the bronchial wall elastic fiber pattern, alveolar and vessel diameters and thickness of elastic fiber in the alveolar wall.
Why to read on?
-
This study shows that patients with COPD have specific structural in vivo abnormalities, such as a higher prevalence of the loose elastin deposition airway pattern and enlarged airspaces, which are significantly related to their lung function; given that FCFM was safe and well tolerated during routine bronchoscopy, these results pave the way for future in vivo structure-function interventional studies in COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a complex disease characterised by small airway fibrosis and parenchymal tissue destruction with loss of lung elastic recoil (emphysema) that leads to gas trapping and progressive airflow limitation,1 as well as by central airway (chronic bronchitis) and pulmonary vasculature changes. These structure–function correlations in COPD were originally described in the late 1970s2 and more recently confirmed using high-resolution CT.3 ,4
Fibred confocal fluorescence microscopy (FCFM) is a new technology that elicits real-time microscopic fluorescence imaging through a thin flexible mini-probe introduced into the 2 mm working channel of a flexible bronchoscope.5 FCFM can provide an in vivo microscopic image of the elastin component of the bronchial wall and the acinus,6–8 as well as the external sheath of the extra-alveolar microvessels.9 Furthermore, FCFM can visualise alveolar macrophages because of their autofluorescent pigments.10 Using FCFM, Thiberville et al5 ,6 described in detail the bronchial wall and acini of both smokers and healthy non-smoker volunteers. More recently, Yick et al11 used this technique to describe bronchial wall changes in asthma and observed novel relationships between the extracellular matrix of the airway wall and lung function in these patients. Although this technique is not able to explore the upper lobes due to the stiffness of the probe, it allows analysis of the elastic network in the small airways of the lower lobes in regions where the alveolar dimension can also be measured.
We hypothesised that FCFM can provide real-time in vivo information of different structural changes that occur in COPD, and that these changes correlate with lung function abnormalities. Accordingly, this study sought to describe the FCFM changes of the bronchi and alveoli in patients with COPD compared with smoker and non-smoker controls and to correlate them with lung function changes.
Methods
Study design
This was a prospective non-interventional controlled study that invited consecutive patients undergoing fibreoptic bronchoscopy for a clinical indication, mostly haemoptysis and/or lung mass on the chest x-ray or CT scan. The study was conducted at Son Espases University Hospital where the patients were recruited over 14 months ending in July 2013.
Study population
We studied 23 patients with a diagnosis of COPD according to the Global Initiative for Chronic Lung Disease (GOLD),1 20 smokers (according to the definition of the Centers for Disease Control and Prevention12) and 20 non-smoker controls, both with normal lung function. Those who had smoked at least 100 cigarettes in their entire life were considered as smokers, and those who smoked cigarettes every day or some days were considered to be current smokers.12 Patients with a history of asthma, bronchiectasis or any suspicion of lung infection and/or patients with a contraindication for bronchoscopy according to international recommendations were excluded.13 Patients with COPD were receiving treatment according to the GOLD recommendations.1
Characterisation of participants
All patients underwent clinical history (including age, gender and smoking history) and pulmonary function measurements including forced spirometry, static lung volumes and carbon monoxide transfer factor (Tlco) performed according to international guidelines.14 Reference values were those of a Mediterranean population.15
CT scan analysis
Chest CT scans were also obtained in all patients in parallel with the study for clinical reasons. It was later re-analysed by an experienced radiologist involved in the study. The presence of emphysema was determined quantitatively as the percentage of low attenuation areas below −950 Hounsfield units (%LLA) using proprietary software (Philips Medical System), with 1% LLA as a threshold for the presence of emphysema as previously described,16 and qualitatively using the so called ‘total emphysema score’ as previously described.17 ,18
Bronchoscopy
Fibreoptic bronchoscopy (Pentax, EB-1570 K, Tokyo, Japan) was performed under intravenous conscious sedation (midazolam 3–7 mg, alfentanil 500 µg). Nasal oxygen supply was provided if needed to maintain oxygen saturation ≥90% with complete monitoring of the patient during the procedure.
Fibred confocal fluorescence microscopy (FCFM)
FCFM was performed with the Cellvizio system F-400 (Cellvizio LUNG, Mauna Kea Technologies, Paris, France) with a laser wavelength 488 nm using a confocal mini-probe (AlveoFlex, Mauna Kea Technologies) as previously described by Thiberville et al.6 Briefly, the confocal mini-probe (1.4 mm in diameter) was introduced through the working channel of the fibreoptic bronchoscope and advanced gently until reaching the lung alveoli (see below). Images of the bronchial wall of the main, lobar and distal bronchi as well as the alveolar space were continuously recorded for later off-line analysis. Images provided by the FCFM probes scan a 600 µm diameter surface with a lateral resolution of 5 µm and a depth below the bronchial surface of 0–50 µm. To compare FCFM images with pathological findings, a standard bronchial biopsy was taken in the same carina as the one where the image had been taken in a subgroup of participants, always in the second or third bronchial level (subsegmentary carina). Immediately after collection the biopsy specimen was fixed in 4% buffered formaldehyde and embedded in paraffin for later standard pathological analysis. At least three different bronchial and alveolar areas were explored in each patient. Because the stiffness of the probe made it difficult to explore adequately the upper lobes, all explored areas were in the lower lobes of the lung.
Image analysis
Morphometric analysis of the proximal bronchial wall and alveolar space was performed using the software provided by the FCFM manufacturer (MedViewer1.1.1; Mauna Kea Technologies) which allows quantification of the bronchial and alveolar wall fluorescence intensity, airspace dimensions (including alveoli and ducts), thickness of elastic fibre in the alveolar wall and extra-alveolar vessel diameter.6 ,7 The distribution of elastic fibres in the bronchial wall was classified as lamellar, loose and mixed pattern according to its orientation, as previously described,11 and it was later confirmed by pathological examination. Fluorescence intensity was quantified using the MedViewer Signal Quantification Toolbox as previously described,6 ,7 and the ratio between the alveolar/bronchial wall fluorescence intensity (ABI) was calculated.6
Statistical analysis
The results are presented as mean±SD unless otherwise stated. Comparisons between groups were performed using the χ2, Mann–Whitney or Kruskal–Wallis tests, as appropriate. The Spearman correlation coefficient test was used to investigate structure–function relationships of interest. MedCalc V.9.2.1.0 (Ostend, Belgium) was used for all analyses.
Results
Study population
Table 1 summarises the main demographic and clinical characteristics of the participants. The patients with COPD were mostly men and were slightly older than the controls. Cumulative smoking exposure (pack-years) was higher in the patients with COPD than in the smoker controls, but the proportion of current smokers was higher in the latter (table 1). By design, lung function was normal in the controls whereas patients with COPD had moderate to severe airflow limitation and reduced Tlco (table 1). Eleven patients with COPD (48%) were on a scheduled combination of inhaled corticosteroids (ICS) and long-acting β2 agonists (LABA), two patients (9%) were on LABA only and 12 were on long-acting muscarinic antagonists with or without LABA/ICS. Nineteen patients (82.6%) with COPD and eight patients (40%) had CT emphysematous changes with statistically significant differences between both groups, whereas none of the non-smokers had evidence of emphysema (table 1). The extent of emphysema was significantly higher in the patients with COPD than in the smoker group both by visual scoring methods and quantitatively (p=0.001 and p = 0.012, respectively).
Demographic, clinical, functional and radiological characteristics of participants
FCFM was performed in all participants without complications during or after the procedure. The duration of FCFM during the bronchoscopy ranged from 5 to 10 min in each participant. Indication for bronchoscopy on each patient is listed in the online supplementary table S1.
Patterns of bronchial wall elastin fibre distribution
As shown in figure 1, using FCFM we recognised the three previously described11 patterns of bronchial wall fibre distribution (lamellar, loose and mixed patterns). The lamellar pattern was characterised by a linear and parallel bronchial thick fibre orientation (figure 1A), in the loose pattern the fibres were thin and non-specifically orientated (figure 1C) and the mixed pattern showed a combination of the two (figure 1E). These FCFM patterns were later confirmed pathologically in bronchial biopsies obtained from five patients with COPD, three smokers and three non-smokers (figure 1). The bronchial wall pattern could not be analysed because of poor image quality in one patient with COPD (4.3%), two smokers (10%) and one non-smoker (5%). With this caveat in mind, the lamellar and mixed patterns accounted for the majority of available observations and were distributed relatively homogeneously between the groups, averaging 40–45% (figure 2). By contrast, the loose pattern was rare in non-smokers and smokers with normal lung function (5%), but its prevalence was more than three times higher (17%) in patients with COPD (figure 2). Lung function variables did not differ significantly according to bronchial elastin fibre pattern (table 2).
Relation between the different patterns of distribution of airway elastin fibres detected by FCFM (see figure 2) and lung function in the studied subjects
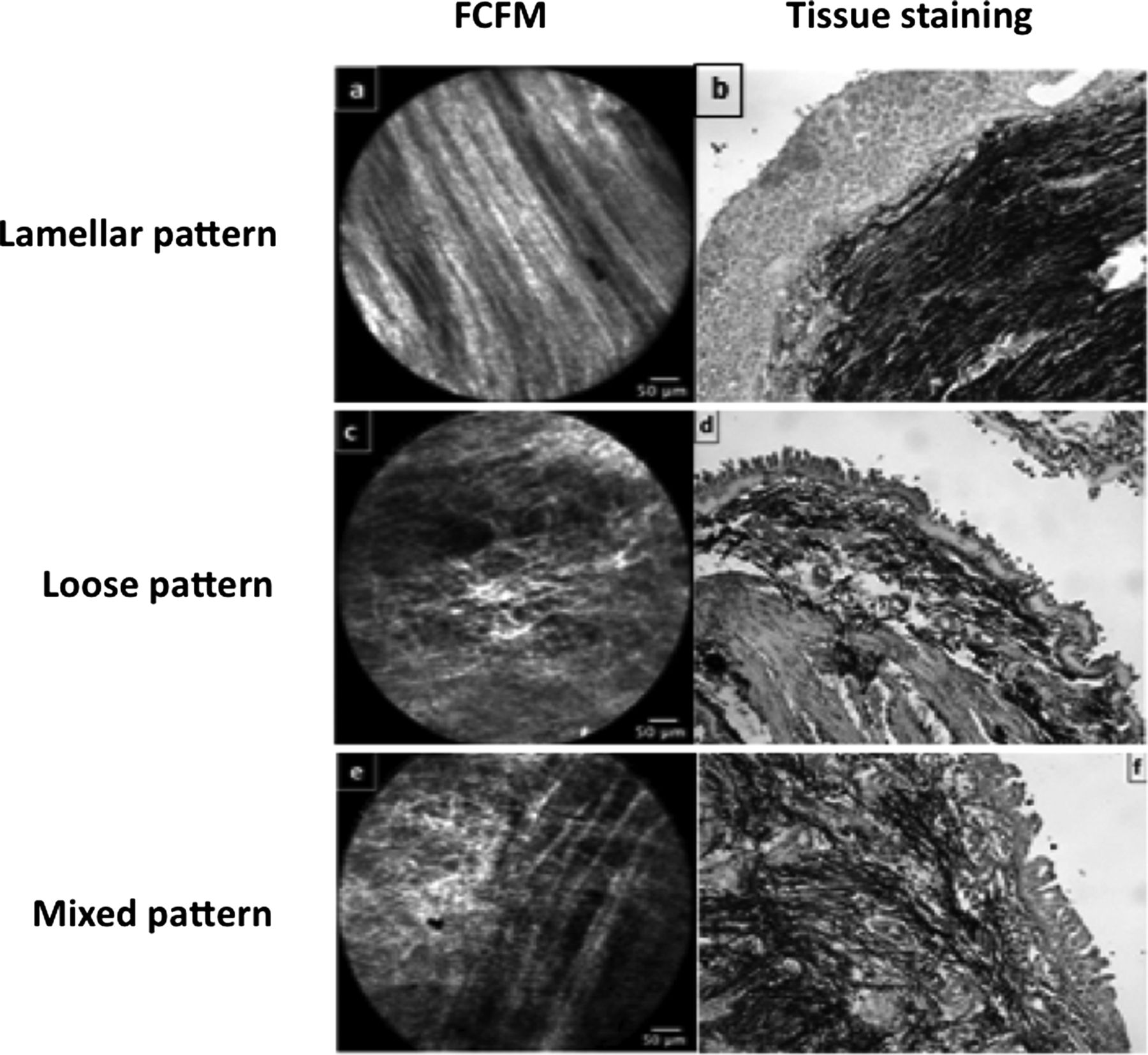
Morphological patterns of bronchial wall elastic fibre distribution by fibred confocal fluorescence microscopy (FCFM) and their corresponding pathological images (H&E stain followed by Elastica-van Gieson elastin fibres stain). For further explanations, see text.

Relative frequency distribution of the three fibred confocal fluorescence microscopy (FCFM) patterns observed in the three groups of participants. For further explanations, see text.
Alveolar measurements
Using FCFM, there is an abrupt transition between airways (figure 1) and alveolar space images (figure 3). Table 3 shows the alveolar diameter, alveolar elastic fibre thickness and extra-alveolar vessel diameter of each of the three groups studied. The alveolar diameter was significantly larger in the patients with COPD, but the alveolar elastic fibre thickness and ABI ratio were similar in the three groups. Extra-alveolar vessels tended to be smaller in patients with COPD, but the differences failed to reach statistical significance. In the patients with COPD, the drug treatment taken had no significant correlation with the extra-alveolar vessel diameter or with other FCFM measurements (p>0.05).
Morphometric alveolar parameters by study group

Fibred confocal fluorescence microscopy (FCFM) images of the alveolar space obtained in patients with chronic obstructive pulmonary disease. For further explanations, see text.
Alveolar macrophages
Alveolar macrophages were clearly visible (figure 3) in eight patients with COPD (35%) and in 14 smokers with normal spirometry (70%), all of them current smokers. By contrast, macrophages could not be identified in former smokers except for one never smoker control (5%).
Structure–function correlations
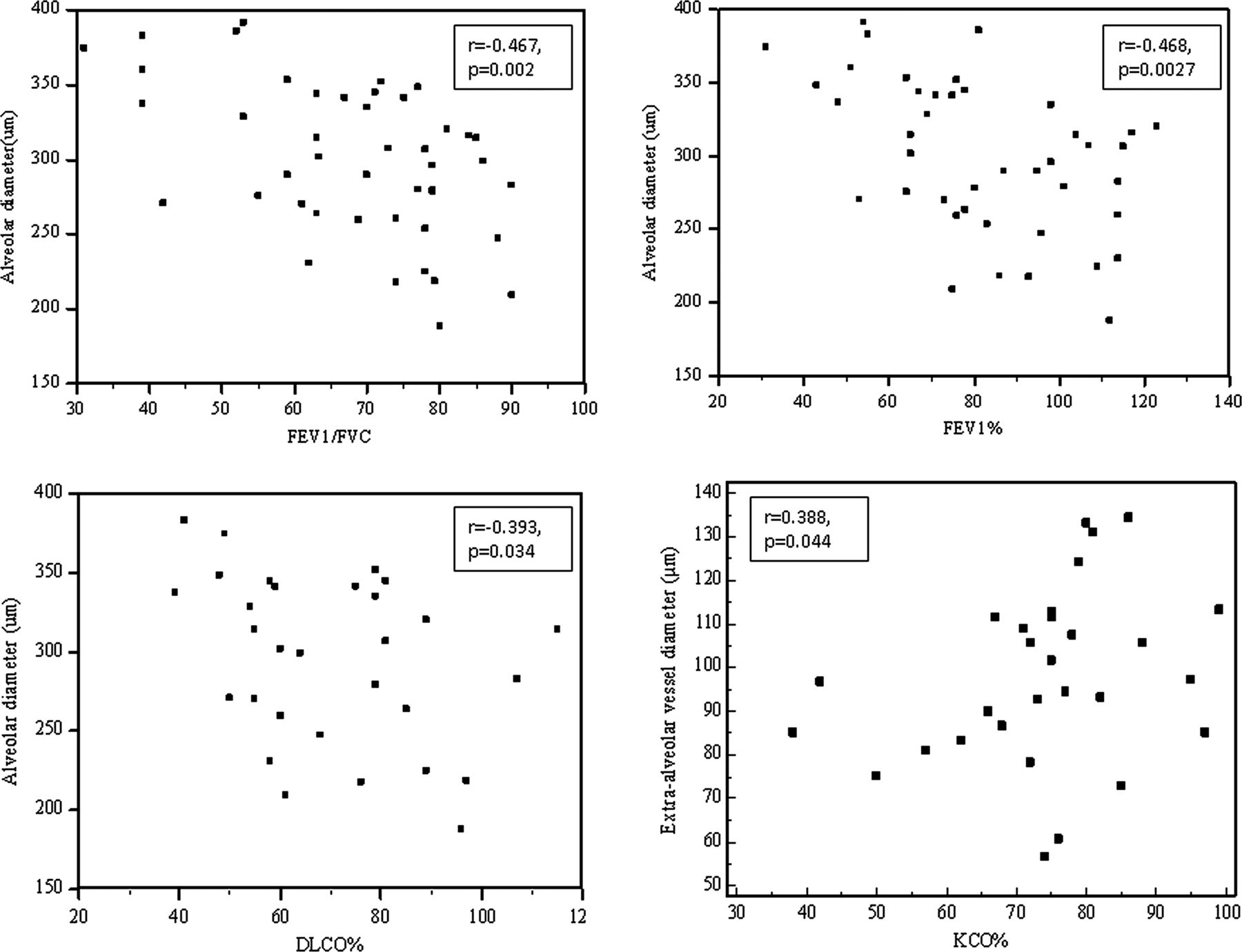
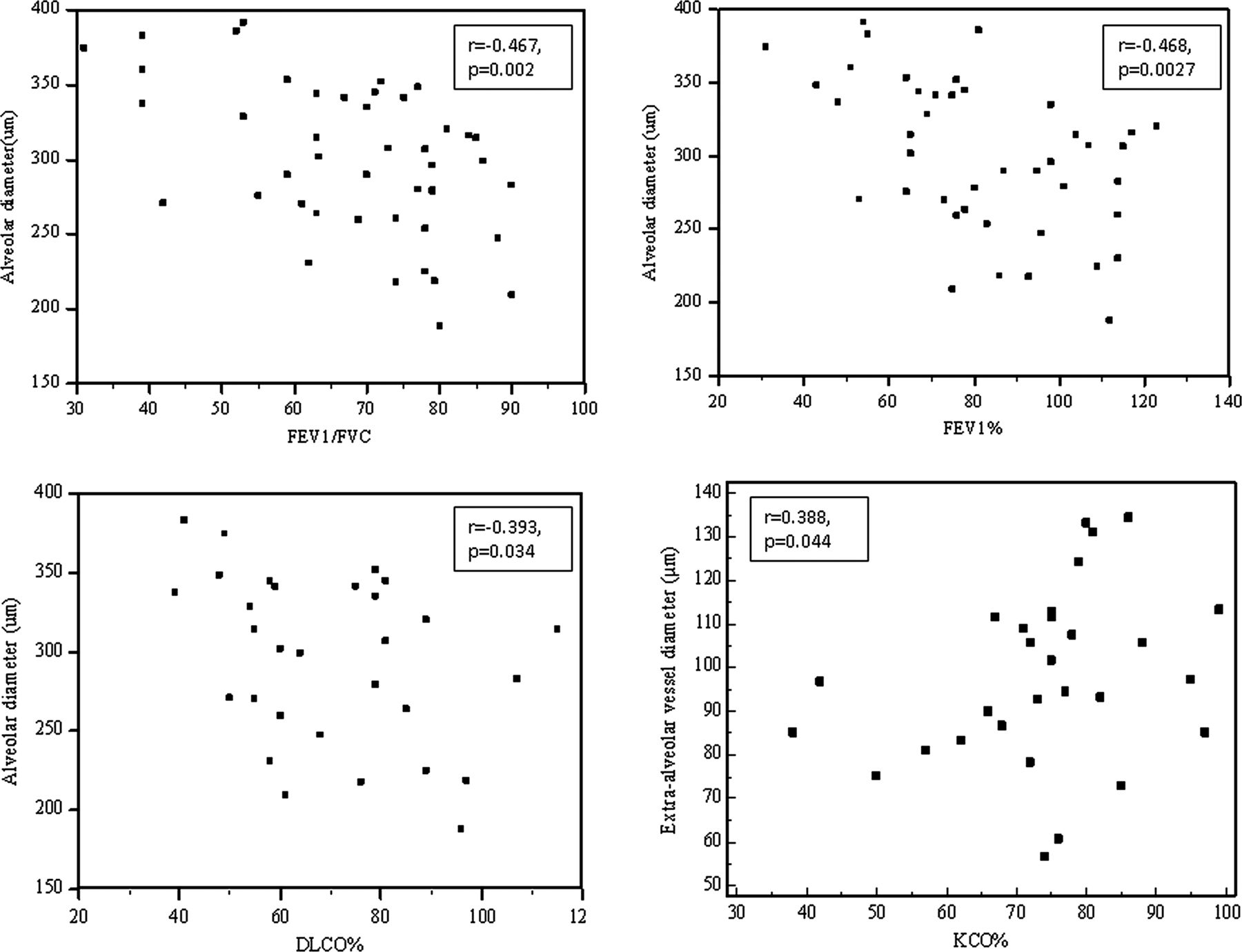
Figure 4 shows the structure–function correlations observed in all participants. The alveolar diameter was inversely related to measures of airflow limitation such as the forced expiratory volume in 1 s (FEV1) both in absolute values and expressed as a percentage of reference (r=−0.338, p=0.033 and r=−0.468, p=0.0027, respectively), maximum expiratory flow (MEF) percentage of predicted (r=−0.405, p=0.014), the FEV1/forced vital capacity (FVC) ratio (r=−0.467, p=0.002), as well as Tlco (r=−0.393, p=0.034). Additionally, we observed a significant direct correlation between the extra-alveolar vessel diameter and the carbon monoxide transfer coefficient (Kco) as a percentage of reference (r=0.388, p=0.044). Other FCFM morphometric parameters (such as the ABI ratio or alveolar elastic fibre thickness) were not related to lung function measures.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlations between fibred confocal fluorescence microscopy (FCFM) morphometric measurements and several lung function parameters. For further explanations, see text. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; Kco, carbon monoxide transfer coefficient; Tlco, carbon monoxide lung transfer factor.
Discussion
This is the first study to use FCFM to describe airway and alveolar abnormalities in patients with COPD in vivo and to relate them to lung function measurements. It also shows that this technique can be routinely performed during bronchoscopy with excellent tolerability and safety. Overall, these results pave the way for future studies investigating the in vivo effects of therapeutic interventions in COPD.
Previous studies
Cosio et al2 were the first to describe in the late 1970s the structure–function relationships in smokers. This and other histological and experimental studies19 ,20 firmly established that emphysema is associated with enlarged airspaces and narrower capillaries with loss of capillary density. Much more recently, Salaün et al21 used FCFM in an animal model of elastase-induced emphysema and confirmed in vivo a significantly increased alveolar maximal diameter with larger intercapillary distance in emphysematous animals. Finally, Newton et al22 used FCFM in 38 patients with different parenchymal lung diseases (and four healthy non-smokers) and reported increased alveolar diameter in those with emphysema.
Interpretation of results
The main results of this study show that: (1) patients with COPD tend to have a higher prevalence of the loose elastin deposition airway pattern (figures 1 and 2); (2) airspace dimension (including alveoli and ducts) is significantly larger (and the extra-alveolar vessel diameter tended to be smaller) in COPD (table 3); and (3) there are significant correlations between structure (by FCFM) and function (figure 4). These are discussed separately below.
Thiberville et al7 described five different FCFM airway patterns in healthy subjects and demonstrated that they varied according to the generation of the bronchial tree imaged. Our samples and images were always captured from subsegmental bronchi. Yick et al11 reported three different patterns of bronchial elastic fibres (later confirmed histologically) in patients with asthma and showed that the lamellar pattern was associated with lower FEV1 values (percentage of reference). In our study we found that the loose pattern was more prevalent in patients with COPD than in controls (figure 2). This is in keeping with previous histological observations by Black et al23 of elastic fibre destruction in the alveoli and the small airways in COPD. These structural abnormalities, however, were not related to any of the lung function parameters assessed (table 2), probably reflecting the fact that the central airways contribute less to functional derangement in COPD than the periphery of the lung, as discussed below.
Our observation of increased alveolar size is also in keeping with previous pathological2 ,19 ,20 and FCFM21 ,22 studies in emphysema. Likewise, the narrower extra-alveolar vessels observed in COPD can also be explained by the stretching over the enlarged alveoli which characterises the emphysematous lung.19 The observed variability in alveolar elastic fibre thickness and the ABI ratio is probably due to the intrinsic fluorescence variations of the elastic fibres among the subjects, either in the bronchial or alveolar walls.6 Moreover, the variability in thickness of the alveolar elastic fibres in the COPD group could also be explained by the remodelling process accompanying this disease, previously pointed out by Vlahovic et al,24 as both the loss and new synthesis of elastin fibres occurred in the emphysematous regions. Finally, the medications prescribed for the patients with COPD did not affect the morphological measurement. This could be due to reduced bronchial vascular reactivity in COPD and the insensitivity of the vasculature to the acute effect of inhalation therapy.25 ,26
The loss of elastic recoil and the destruction of alveolar attachments that maintain the patency of small airways are well-known determinants of airflow limitation in emphysema.27 ,28 Recently, Yablonskiy et al29 studied the morphological changes associated with emphysema using 3He diffusion MRI; they found evidence of alveolar destruction in emphysematous lungs which correlated with diffusion defects. In keeping with this, we observed a significant correlation between the alveolar diameter (an in vivo surrogate marker of the extent of emphysema) and the severity of airflow limitation expressed by FEV1 (%) and the FEV1/FVC ratio. Of interest, too, was the observed inverse correlation between the Tlco and the vascular diameter, probably reflecting the well-established relationship between the former and the degree of emphysema present.2 Furthermore, MEF (%), a measurement of small airway disease, was inversely correlated with alveolar diameter, which is consistent on the one hand with the previous explanation27 ,28 and, on the other hand, with the findings of Black et al23 that destruction of elastic fibres also involved the small airway in COPD leading to its obstruction.
Interestingly, our measurements of mean alveolar dimensions in patients with COPD, smokers and non-smokers (table 2) are consistent with measurements of mean linear intercept (Lm). Moreover, they fall well within the range of Lm reported in normal lungs using microCT,30 which suggests that our measurements were obtained in regions of COPD lungs with very little emphysematous destruction, a fact that has been confirmed by CT scan analysis. This supports the hypothesis that bronchiolar destruction begins before the onset of emphysematous destruction in COPD.30 ,31 The correlations between FCFM measurements and the extend of emphysema in both smokers and COPD patients are shown in the online supplementary tables S2 and S3.
Finally, numerous previous studies have reported increased macrophage numbers in bronchoalveolar lavage and surgical lung specimens in smokers.32 ,33 Our results confirm these observations and others using FCFM,7 since alveolar macrophages were easily detectable in vivo in current smokers, with or without COPD (figure 3). This is probably due to their high content of tobacco tar which acts as an exogenous fluorophore.10 It is unclear from our data why one non-smoker subject had visible alveolar macrophages using FCFM, but environmental exposures such as passive smoking might have contributed.34
Clinical implications
Our study is a pilot descriptive study without direct clinical implications, but at least two can be envisaged. First, it shows that FCFM can be used safely and with excellent tolerability during routine bronchoscopic examination. Second, and more importantly, it opens a new way potentially to assess microscopically the impact of therapeutic interventions in the lung of patients with COPD in vivo which, of course, requires further research. Further, we assume that FCFM, as a minimally invasive tool, could be used to validate the novel microstructural biomarkers of emphysema found with hyperpolarised gas diffusion MRI29 ,35 in future studies.
Study limitations
The present study has some limitations. First, we used different mini-probes with potentially different fluorescent properties in different participants. To address this issue we expressed the results as the ABI ratio following previous recommendations.6 Second, measurement of the different parameters was performed on captured videos taken during spontaneous breathing, so alveolar diameter measurements were the average of several respiratory cycles, also as previously published.6 Third, owing to the stiffness of the mini-probe used, we were not able to reach the upper lung lobes so only the lower lobes were studied with FCFM; this may not reflect the maximal extent of emphysematous changes which is known to predominate in the upper lung zones. The fact that control groups were studied in a similar way partly addresses this limitation.
Conclusions
COPD is characterised by microscopic changes in the airways and parenchyma that can be detected in vivo by FCFM and that relate to clinically relevant measurements of lung function. These findings open new possibilities for the in vivo assessment of therapeutic interventions in COPD.
Acknowledgments
The authors thank the participants for their willingness to contribute to medical research and the nursing staff of our institution (Maria Angels Noguera and Rocío Martinez) for the excellent technical contribution. BGC also would like to thank Professor Manuel Cosio and Professor Marina Saetta for their useful comments and encouraging support on life and research. The authors would also like to thank one of the co-authors, Dr Bernado Togores, for his long life dedicated to lung physiology and teaching.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors BGC and AK: designed the protocol, acquired and analysed the data and prepared the manuscript. HS, FF and JS: data acquisition and analysis. CG: pathological analysis. ML and AR: patient recruitment and sample processing. BT: lung function tests; JP: analysis of emphysema in CT scans; AA: data analysis and manuscript preparation.
-
Funding The study was supported in part by grants from the Spanish Society of Respiratory Medicine (Separ), Conselleria de Economia and Conselleria de Salud de las Islas Baleares.
-
Competing interests HS was granted by the University of Alexandria and Ministry of Higher Education of Egypt as member of ParOwn (the Partnership and Ownership initiative).
-
Patient consent Obtained.
-
Ethics approval The study protocol was approved by the local Ethics Committee (number IB1097/08).
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves