Article Text

Statistics from Altmetric.com
A 51-year-old woman presented to the chest clinic with history of progressive dyspnoea and dry cough for 8 weeks. Her past medical history was remarkable for sleeve gastrectomy 3 months ago, which resulted in loss of three stones. She also reported migraines for which she had an implanted occipital nerve stimulator and had undergone hysterectomy with bilateral salpingo-oophorectomy 18 months ago. Other history included hypothyroidism, hypertension and depression. Her medications were Hormone Replacement Therapy (HRT), Nifedipine, Losartan, Levothyroxine, Lansoprazole, Simvastatin and Fluoxetine. She had smoked for 3 years in her 20s, no more than 3–5 cigarettes per day and had no noteworthy occupational exposure. She had a family history of maternal myelodysplasia and paternal cerebral malignancy.
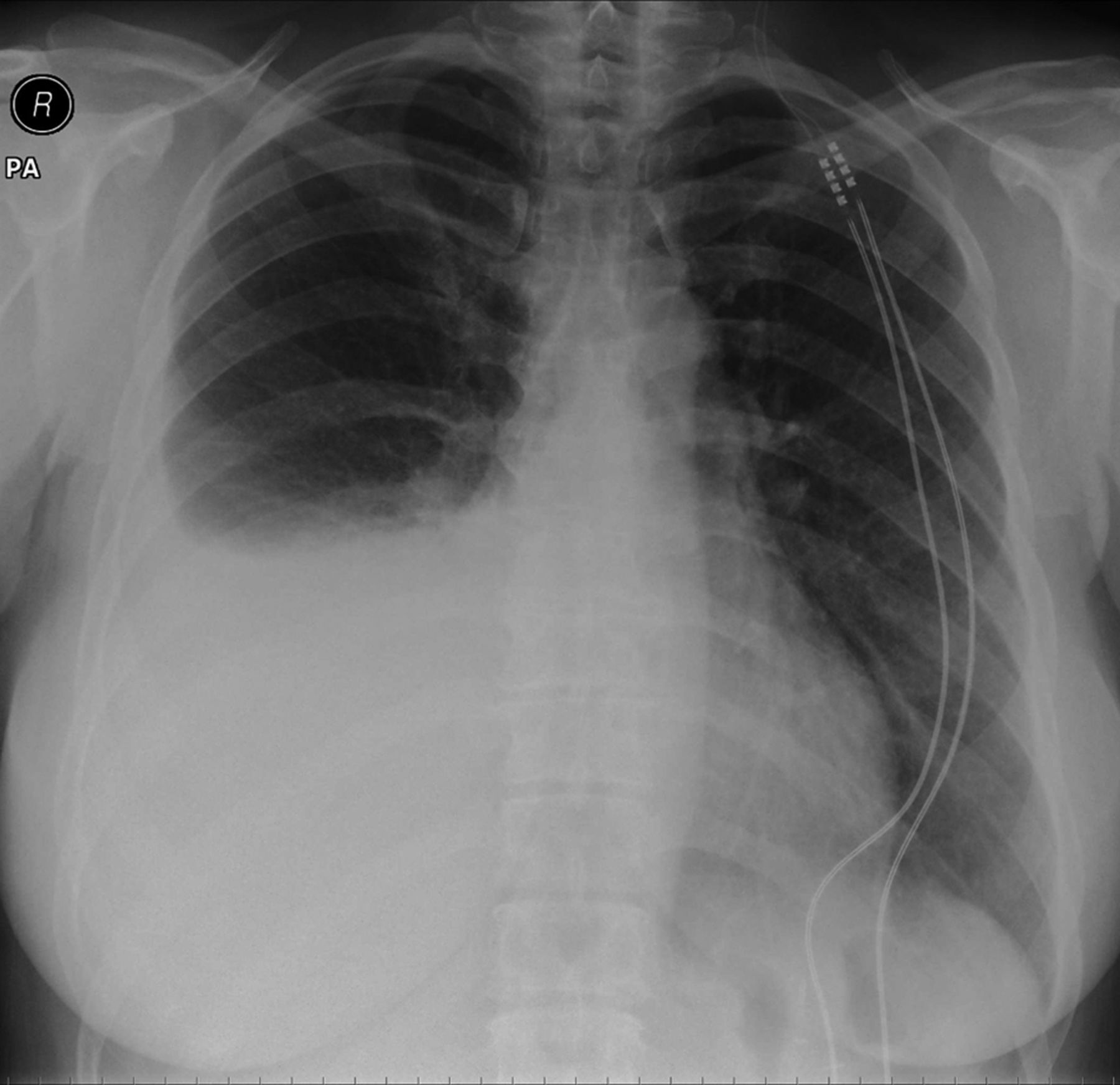
Examination revealed right-sided thoracic dullness and reduced breath sounds. Blood results were unremarkable. A chest radiograph was performed confirming a right-sided effusion (figure 1); therapeutic aspiration demonstrated a chylous effusion. The pleural fluid showed haemosiderin-laden macrophages on cytological examination and there was no microbiological growth. The effusion recurred within 2 weeks and intercostal drainage was performed. A contrast-enhanced CT of her thorax was performed with retrospective high resolution reconstructions to investigate the cause of the effusion (figure 2).

Posterior-anterior chest radiograph.

{kind=link}
{kind=link}
Axial high resolution CT reconstruction of contrast enhanced images—1 mm on high spatial resolution algorithm.
Question
What is the diagnosis?
Answer
The CT demonstrates multiple, bilateral, small thin-walled pulmonary cysts, the right pleural drain and a small volume of pleural air. The differential of these appearances includes lymphangioleiomyomatosis (LAM), Langerhans’ cell histiocytosis and early centrilobular emphysema. Given the clinical scenario, the appearances are highly suggestive of LAM. Radiologically, the appearance and distribution of the cystic air spaces supports this. The diagnosis was confirmed by lung biopsy taken at the time of surgery, performed to ligate the thoracic duct and resolve the recurrent chylous effusions. On direct questioning the symptom onset was probably shortly after commencing HRT, raising the possibility that this reactivated quiescent disease. The patient has been referred for further management to the national LAM centre in Nottingham.
LAM is a progressive lung disease of insidious onset, typically affecting women between 30–49 years of age.1 The presentation is with chronic cough, pneumothorax or chylothorax. Progressive dyspnoea develops as the disease evolves. Diagnosis is frequently delayed as symptoms mimic many common respiratory conditions. However, high resolution CT appearances are fairly typical and lead to the correct diagnosis in 80% of cases.2 Frequently lung biopsy is not required with a supportive clinical history and imaging. LAM is microscopically characterised by non-malignant smooth muscle cell proliferation in the lungs with progressive obstruction of lymphatic vessels and small airways.3 Other organ involvement is not uncommon, with renal amyloidosis, lymphangiomyomata and chylous ascites all reported.
There are two forms of LAM; sporadic and tuberous sclerosis complex-associated. No other risk factors have been identified. The prevalence of the sporadic form of the disease is thought to be 30–50 000 worldwide.
There are currently no effective treatments for LAM, and a supportive approach is taken. Lung transplantation is considered when forced expiratory volume in 1 second approaches 30% predicted.2 The median survival is ∼15 years from the onset of symptoms.
Footnotes
-
Contributors All contributors were involved in the care of the patient. MM suspected the diagnosis from the imaging.
-
Funding None.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves