Article Text

Statistics from Altmetric.com
- Non-small cell lung cancer
- lung cancer chemotherapy
- thoracic surgery
- bronchiectasis
- interstitial fibrosis
- lung cancer
- small cell lung cancer
- bronchoscopy
- mesothelioma
Clinical presentation
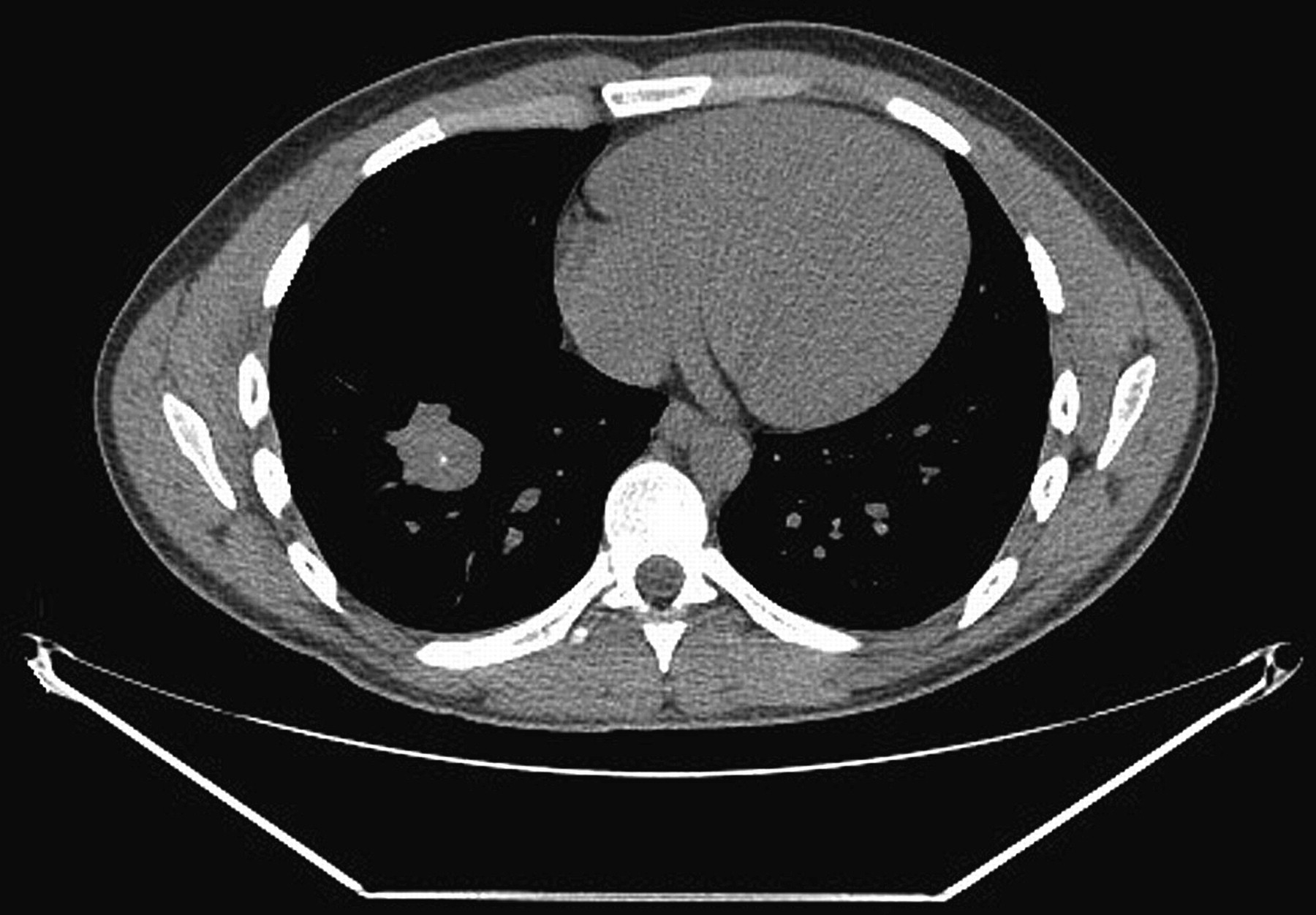
A 19-year-old student who had never smoked presented with a 6-month history of cough, wheeze, sputum production and generalised fatigue. His exercise tolerance was unaffected and he continued to play rugby competitively. He had a history of childhood asthma and received treatment with inhaled salbutamol with no effect. A chest x-ray revealed a round density at the base of the right lung. A CT chest was performed (figure 1) and subsequently a 68Ga-DOTATATE (1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid-d-Phe(1),Tyr(3)-octreotate) PET-CT (positron emission tomography-CT) was arranged, demonstrating that the mass had a maximum standardised uptake value of 6.6 (figure 2). He was referred for a right lower lobectomy. Histological evaluation of the lobectomy specimen demonstrated bland spindle cell proliferation with a prominent inflammatory infiltrate. Immunohistochemical staining was positive for vimentin, smooth muscle actin and cytokeratin AE1/AE3, and negative for desmin, caldesmon, calponin, ALK1 and CD34.

CT scan of chest showing a 3.3 cm lobulated irregular mass located centrally and inferiorly in the lower lobe of the right lung. This contains some central calcifications, but no cavitation.

68Ga-DOTATATE (1,4,7,10-tetraazacyclododecane-N I, N II, N III-tetraacetic acid (D)-Phe 1-Tyr 3-octreotide) positron emission tomography-CT showing focal high uptake with a maximum standardised uptake value of 6.6 and no uptake elsewhere.
Question
What is the diagnosis?
See page 469 for the answer
Answer
From the question on page 468
Examination of the surgical specimen demonstrated pathological and immunohistochemical features (figures 3 and 4) consistent with an inflammatory myofibroblastic tumour (IMT). IMTs are rare (reported incidence of 1% of all lung masses1), but are the most common primary pulmonary tumour in children. Symptoms depend on location of the mass and up to 50% may be asymptomatic. Five-year survival after diagnosis is 91.3%,2 but the recurrence rate following resection is 4% and there may be a small risk of malignant sarcomatous transformation.2 Debate is ongoing as to the pathogenesis of the lesions3 but postulated mechanisms include initial insult due to viral infection leading to an uncontrolled aberrant inflammatory response. Both typical and atypical carcinoid tumours show positive uptake with somatostatin receptor scintigraphy, and was an important differential diagnosis in this case. PET somatostatin ligands such as 68Ga-DOTATATE and 68 Ga-DOTATOC (1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid-d-Phe(1),Tyr(3)-octreotide) have been shown to be superior to conventional agents such as 111 In-diethylenetri- amine pentaacetic acid (DTPA) octreotide. In particular both typical and atypical carcinoid tumours are recognised to demonstrate uptake with 68Ga-DOTATATE,4 and 18F-fluoro-2-deoxy-d-glucose (FDG) uptake has been shown to correlate with a grade of pulmonary neuroendocrine tumours with typical carcinoids showing high uptake of 68Ga- DOTATATE but often low 18F-FDG accumulation. Higher grade tumours have less 68Ga-DOTATATE uptake but are more consistently positive with 18F-FDG.5 This report demonstrates that IMTs may also show uptake on 68Ga DOTATATE scans, giving rise to the hypothesis that IMTs express somatostatin receptors, which has been recently confirmed on immunohistochemistry.3 Although somatostatin receptors have a wide distribution, being expressed on many different cell types, high receptor density is only typically found in neuroendocrine tumours. Surprisingly, our case showed avid IMT accumulation of 68Ga-DOTATATE in contrast to other reports which showed weak uptake with 111In-DTPA, octreoscan and 68Ga-DOTATOC.3 4 There was also internal calcification, a feature often seen in pulmonary carcinoids but not previously described in IMTs. According to the WHO classification of lung tumours, IMT is a subgroup of the ‘inflammatory pseudotumours’ the histological hallmark of which is a bland spindle cell proliferation arranged in fascicles. A prominent inflammatory infiltrate containing plasma cells, histiocytes and lymphocytes is seen and occasionally Tuton type giant cells. The immunohistochemical features of these tumours comprise positivity for vimentin and smooth muscle actin and rarely desmin (in this case negative). Cytokeratins AE1/AE3 are positive in only 30% of cases and ALK1 in about 40%.6 Interestingly, in this case immunohistochemical staining for somatostatin was negative (figure 5), raising questions about the relative sensitivity and specificity of currently available radiolabelled ligands and immunohistochemical markers. IMTs should be considered in the differential diagnosis of young patients with pulmonary lesions that demonstrate uptake on 68Ga-DOTATATE scans.

Inflammatory myofibroblastic tumour: well circumscribed proliferation of bland spindle shaped cells arranged in bundles, with heavy plasma cell infiltration. No atypical mitotic activity or necrosis (H&E stain, magnification 100×).

Immunohistochemical staining of specimen showing spindle cells with strong positivity for actin (smooth muscle actin, 40×).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining for somatostatin was negative.
Footnotes
Funding NN is an MRC Clinical Research Training Fellow. SMJ is a Wellcome Trust Senior Fellow in Clinical Science. This work was undertaken at the University College London Hospital/University College London which received a proportion of funding from the Department of Health's National Institute for Health Research Biomedical Research Centres funding scheme (SMJ, NN).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves