
Abstract
Objective
To evaluate the effects of protective and conventional ventilation with or without positive end-expiratory pressure (PEEP), on systemic tumor necrosis factor-α, interleukin-6 levels and pulmonary function during open heart surgery.
Design
Prospective, randomized clinical study.
Setting
Single university hospital.
Patients and participants
Forty-four patients undergoing elective coronary artery bypass grafting surgery with cardiopulmonary bypass.
Interventions
Patients ventilated with (1) protective tidal volumes (6 ml/kg, respiratory rate: 15 breaths/min, PEEP 5 cmH2O, n=15) group PV; (2) conventional tidal volumes (10 ml/kg, respiratory rate: 9 breaths/min, PEEP 5 cmH2O, n=14) group CV+PEEP and (3) conventional tidal volumes (10 ml/kg, respiratory rate: 9 breaths/min, n=15) without PEEP, group CV+ZEEP. Various pulmonary parameters, systemic TNF-α and IL-6 levels were determined throughout the study.
Measurements and results
There were no differences among the groups regarding the systemic TNF- α and IL-6 levels. The plateau airway pressures of group PV were lower than those of groups CV+PEEP (p=0.02) and CV+ZEEP (p=0.001) after cardiopulmonary bypass. The shunt fraction of group PV was significantly lower than that of group CV+ZEEP 24 h after surgery (p<0.05). Oxygenation and the alveolar-arterial oxygen difference were better in both PEEP groups than in group CV+ZEEP 24 h after the operation.
Conclusions
We could not find any evidence that protective mechanical ventilation prevents some of the adverse effects of cardiopulmonary bypass on the lung, nor systemic cytokine levels, postoperative pulmonary function or length of hospitalization.
Similar content being viewed by others


Introduction
In patients with acute lung injury, protective ventilation with tidal volumes (VT) of 6 ml/kg and high positive end-expiratory pressure (PEEP) induces lower cytokine release and less pulmonary injury as compared with conventional VT (10–15 ml/kg) during mechanical ventilation [1]. However, mechanical ventilation with high VT on zero end-expiratory pressure (ZEEP) does not induce cytokine release into the systemic circulation in normal lungs [2]. Cardiopulmonary bypass initiates a systemic inflammatory response syndrome characterized by the activation of complement, neutrophils, endotoxin and the proinflammatory cytokines [3, 4]. The contact of the blood with artificial surfaces and ischemia/reperfusion of the heart and the lungs may be responsible for this syndrome. Inflammation following cardiopulmonary bypass may contribute to the common ‘post-pump syndrome’, which involves various organs, and pulmonary injury is only part of this syndrome [3]. The lungs release proinflammatory cytokines during pulmonary reperfusion in coronary artery bypass grafting (CABG) operations, particularly interleukin (IL)-6, IL-8, IL-10 and polymorphonuclear neutrophils (PMNs) [5].
Pulmonary injury associated with cardiopulmonary bypass is similar to acute respiratory distress syndrome (ARDS) caused by other etiologies. The difference is that the pulmonary injury observed after cardiopulmonary bypass is generally transient and resolves within 24 h. The prevalence of ARDS after cardiopulmonary bypass is quite rare (0.5%), but the mortality is high (91.6%) [6].
Polymorphonuclear neutrophil sequestration caused by cardiopulmonary bypass alone does not result in acute lung injury [7]. A second insult which activates PMNs, such as endotemia or tumor necrosis factor (TNF)-α, is necessary for an overwhelming inflammatory response which leads to pulmonary edema, hypoxemia and ARDS [8]. However whether conventional VT ventilation combined with cardiopulmonary bypass constitutes an additional insult to the lungs remains to be clarified.
We conducted this study to test the hypothesis that ‘conventional VT ventilation is associated with higher cytokine levels compared with protective VT ventilation’ during open heart surgery. In this study we compared systemic TNF-α, IL-6 levels and pulmonary mechanics between the protective (VT 6 ml/kg of ideal body weight on 5 cmH20 PEEP) and conventional mechanical ventilation (VT 10 ml/kg) groups with or without PEEP during and after cardiac surgery.
Materials and methods
After ethics committee approval and completion of written informed consent forms, 44 patients undergoing CABG operations between November 2001 and August 2002 with cardiopulmonary bypass were enrolled in the study. Exclusion criteria included acute infections, pre-existing pulmonary disease, left ventricular ejection fraction less than 40%, myocardial infarction within 1 month, re-operation, coagulopathy, unstable angina pectoris and renal failure.
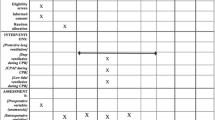
Following the anesthesia induction, patients were randomized to receive volume-controlled ventilation (Servo ventilator 900 C; Siemens, Solna, Sweden) with (1) protective VT of 6 ml/kg on 5 cmH2O PEEP; respiratory rate 15 breaths/min (group PV), (2) conventional VT of 10 ml/kg on 5 cmH2O PEEP; respiratory rate 9 breaths/min (group CV+PEEP) or (3) conventional VT of 10 ml/kg on ZEEP; respiratory rate 9 breaths/min (group CV+ZEEP). The inspiratory/expiratory ratio was 1:2 in all groups.
After premedication all the patients received 6 l/min oxygen via face-mask. Anesthesia involved high dose fentanyl citrate. Following induction with midazolam and vecuronium, anesthesia was maintained with midazolam infusion, pancuronium boluses and an oxygen-air mixture of 50%. A 7 Fr thermodilution catheter (Edwards Lifesciences, Irvine, CA, USA) was introduced via the right internal jugular vein for hemodynamic measurements and blood sampling. Cardiac output was measured by the thermodilution technique, averaging the results of three cold injections (10 ml 5% dextrose at 4°C), using a Siemens monitor (SC 7000, Stockholm, Sweden).
Cardiopulmonary bypass was instituted using a roller pump (Jostra, Lund, Sweden) and membrane oxygenator (Dideco, Mirandola, Italy). The pump was primed with 1000 ml of lactated Ringer’s solution and 500 ml of gelatin solution (Gelofusin, B. Braun, Melsungen, Germany) to achieve a hematocrit level of 20–25%, heparin 50 mg, cefazolin 1 g, sodium bicarbonate 100 mmol, 0.5 g/kg mannitol 20%; no blood products were used. The lungs were not ventilated and the endotracheal tube was open to atmospheric pressure during cardiopulmonary bypass. All the patients were cooled to 32°C. The pump flow rates were maintained at 2.4–2.6 l/min per m2 and 2 l/min per m2 during normothermia and hypothermia, respectively.
Before discontinuation of cardiopulmonary bypass, the lungs were inflated manually up to 40 cmH2O peak airway pressure for 20 s and the ventilation was started with an FIO2 of 0.6 then reduced to 0.5. Corticosteroids, antifibrinolytic agents or aprotinin were not used and no ultrafiltration technique was employed throughout the study. Heparin was neutralized with protamine chloride added to 50 ml of 5% dextrose. Protamine was infused in 15 min in a 1 mg:1 mg ratio to achieve an activated clotting time of 80–120 s. Protamine was administered into the right atrium via a central venous catheter. Red blood cells were transfused to achieve a hemoglobin level of about 9.5 g/dl. Both red blood cells and protamine were given following the first blood sampling for cytokine analysis after cardiopulmonary bypass. None of the patients received platelet and fresh frozen plasma transfusions during the study. The left internal thoracic artery was used and the left pleura was routinely opened in all patients.
Arterial and mixed venous blood were drawn and analyzed (EML 505, Radiometer, Kopenhagen) 15 min after induction of anesthesia (time A), 2 h after cardiopulmonary bypass—the sternum was closed—(time B) and 24 h after surgery (time C) to determine oxygenation, alveolar-arterial oxygen gradient, arterial CO2 and the shunt [9] levels. Alpha-stat technique was employed to evaluate the blood gases during cardiopulmonary bypass. Pulmonary vascular resistance, oxygen consumption (VO2) and delivery (DO2) index calculations [10] were made at times A, B and C.
Airway pressures (plateau, peak and mean airway pressures), expiratory minute volume, total PEEP (intrinsic PEEP + extrinsic PEEP) and VT values were obtained from the ventilator’s own display and recorded at times A and B. Intrinsic PEEP level was determined with the end-expiratory occlusion technique. Dynamic and static lung compliances were measured using the standard formula [7] at times A and B. Successive arterial blood samples for cytokine levels were taken (A) after induction of anesthesia and (B) 15 min, (C) 1 h and (D) 2 h after cardiopulmonary bypass. For cytokine analysis blood samples were collected into the non-pyrogenic, sterile Falcon tubes ( Bender Medsystems Diagnostics, Vienna, Austria). Serum was separated by cold centrifugation of the blood at 1500 g for 10 min and stored at –70oC. Serum IL-6 and TNF-α were measured using enzyme-linked immunosorbent assay kits obtained from Bender Medsystems Diagnostics (Vienna, Austria). These analyses were carried out on the same day in a blinded fashion. There was no cross-reactivity among the measured variables. The detected IL-6 and TNF-α levels of healthy blood donors ranged between 1.4 and 14.1 pg/ml, and 5 and 66 pg/ml, respectively, with the kits we used.
Forced vital capacity, forced expiratory volume in 1 s and forced expiratory flow during the middle half of the forced vital capacity values measured (Vitalograph Spirometer, Lameris, The Netherlands) before the operation and postoperative 7th day were recorded.
All the values are reported as means (± SD). One-way ANOVA and post hoc Bonferonni tests were used to compare means between the groups. As the cytokine distribution was not normal and the power analysis of the groups for the multivariate tests revealed low levels (60%), non-parametric Friedman test was applied to evaluate the cytokine changes between the groups. The cytokine levels are reported as median and interquartile range. Comparisons between variables were carried out using the Pearson correlation test. A p value of 0.05 or less was considered significant. Unistat version 5.0 (Unistat, UK) for windows was used for the statistical analysis.
Results
The groups were similar in demographic data, preoperative cardiac medications, aortic cross-clamp and cardiopulmonary bypass times (Table 1). There was no difference among the groups in respect to preoperative and postoperative respiratory function tests (Table 2).
Hemodynamic evaluation (cardiac index, mean systemic, pulmonary artery, central venous and pulmonary wedge pressures, heart rate, systemic vascular resistance, DO2 and VO2 indexes) did not reveal significant differences among the groups throughout the study. The pulmonary vascular resistance index was significantly lower at the end of the study in group PV (46±19 dyn.sec.cm-5.m-2) compared to CV+PEEP (61±27 dyn.sec.cm-5.m-2) and CV+ZEEP groups (58±24 dyn.sec.cm-5.m-2).
The plateau airway pressure values of group PV were significantly lower than both groups CV+PEEP and CV+ZEEP after cardiopulmonary bypass (p=0.02 and p=0.001, respectively). Oxygenation was better in both group PV and group CV+PEEP as compared to group CV+ZEEP at time C (p=0.03 and p=0.05, respectively). The alveolar-arterial oxygen gradient values of group CV+ZEEP were significantly higher than the other groups after surgery and the shunt fraction of group PV was significantly lower than group CV+ZEEP at time C (p<0.05; Table 3).
There were no differences among the groups regarding the serum TNF-α and IL-6 levels throughout the study (Figs. 1 and 2). There was a considerable variation in the levels of these proinflammatory cytokines after cardiopulmonary bypass. No positive correlation was found among the aortic cross-clamp, bypass times and cytokine levels of the groups.

Systemic tumor necrosis factor-α levels. PV protective mechanical ventilation group, CV+PEEP conventional mechanical ventilation group with PEEP, CV+ZEEP conventional mechanical ventilation group without PEEP, A after induction of anesthesia, B 15 min after CPB, C 1 h after CPB, D 2 h after CPB. Cytokine levels are expressed as median (inner line), 25/75 percentiles (box) and 10/90 percentiles (whisker) and the values out of these ranges (x)

Systemic interleukin-6 levels (see Fig 1 for abbreviations)
Total operative fluid balance (782±517 ml in group PV, 628±340 ml in group CV+PEEP and 603±497 ml in group CV+ZEEP) and red blood cell transfusion (2.3±0.9 units in group PV, 2.3±1.4 units in group CV+PEEP and 1.9±0.5 units in group CV+ZEEP) were not different among the groups.
Intubation times (9.9±1 h in group PV, 10±1.4 h in group CV+PEEP and 9.9±1.5 h in group CV+ZEEP) were similar and none of the patients required reintubation. There was no difference among the groups regarding the hospitalization period (6.7±0.7 days in group PV, 7.3±1.2 days in group CV+PEEP and 7.3±0.9 days in group CV+ZEEP). Two patients in group CV+ZEEP experienced bronchospasm, atelectasis and hypoxia following extubation and, as a result, prolonged intensive care unit (4 days) and hospitalization periods (10 days each). None of the patients participating in this study died.
Discussion
The main findings of this study are (1) similar levels for both cytokines among the groups were observed following cardiopulmonary bypass, (2) protective mechanical ventilation did not provide better postoperative pulmonary functions or a shorter hospitalization period compared to conventional ventilation strategies.
Cardiopulmonary bypass may cause a greater pulmonary inflammatory response than the systemic one due to the endothelial and epithelial injury [11]. Complement activation during cardiopulmonary bypass results in neutrophil sequestration and subsequent activation in the alveolar vasculature. Adherence of activated neutrophils to the endothelium and subsequent release of active biological mediators such as elastase and myeloperoxidase may lead to diffuse pulmonary injury and accumulation of extravascular lung water [3]. This inflammatory response has been shown to be amplified with a second insult such as endotoxin translocation [12]. However, pulmonary dysfunction during cardiac surgery is not only caused by extracorporeal circulation. Protamine used to neutralize heparin, surgical trauma, ischemia/reperfusion injury, thrombin activation, transfusion of blood products and different anesthetic techniques are other factors responsible for the inflammatory response [13].
Cardiopulmonary bypass also changes the bronchoalveolar tree structure by inducing atelectasis [11]. Atelectasis lasting 1 h has been shown to facilitate proinflammatory cytokine production by alveolar macrophages [14]. Mechanical ventilation modulates the activation of PMNs in the lungs, which may lead to a systemic inflammatory response and increased alveolar capillary permeability [15, 16]. Both inflammatory products (cytokines, platelet activating-factor, thromboxanes, prostaglandins) and mechanical forces are responsible for the lung damage that occurs during mechanical ventilation [17]. To our knowledge a clinical study in the English language literature to evaluate the effects of protective and conventional ventilation strategies on systemic cytokine levels after cardiac surgery is lacking.
Cytokines are believed to play a major role in the pathophysiology of acute inflammation associated with cardiac surgery. Excessive cytokine levels may result in exaggerated systemic inflammation and a greater secondary injury. Cardiopulmonary bypass causes a significant amount of complement and cytokine release including TNF-α, which is an important neutrophil activator [18]. This cytokine’s production begins during cardiopulmonary bypass, reaches a peak 2–4 h after termination of this, then begins to fall rapidly whereas IL-6 gradually decreases in the following 24 h [19, 20]. In an experimental study, increased systemic TNF-α levels have been shown following an injurious mechanical ventilation strategy lasting 1 h [21]. Evidence from these data and switching to weaning modes early are the rationale for the timing of the cytokine sampling in our study.
As well as the lungs, the myocardium also releases cytokines such as TNF-α [22] and IL-6 [23], which are believed to be involved in the systemic inflammation induced by extracorporeal circulation. As the heart is perfused only by a small percentage (5–10%) of the whole body cardiac output, this amount does not significantly change the systemic cytokine levels. Furthermore, two studies have shown that TNF-α and IL-6 levels measured from pulmonary vein and systemic artery after cardiopulmonary bypass were similar [24, 25]. In this study, despite the wide range of systemic TNF-α and IL-6 levels observed, there was no significant difference among the groups. The cytokine release pattern observed in our study is correlated with the other studies performed during cardiac surgery [24, 26]. The reason for the individual variation in TNF-α and IL-6 levels might be due to the effect of ischemia in the lungs. Ricard et al. [27] observed the same discrepancy in an ischemic animal lung model. TNF-α gene polymorphism which influences the inflammatory response following cardiac surgery may also explain the individual differences [28].
Normothermia or moderate hypothermia did not cause different cytokine responses during coronary bypass surgery [26]. It has been shown that a longer cardiopulmonary bypass time coincides with a greater proinflammatory cytokine response [24], however in our study we could not find a positive correlation between the aortic cross-clamp, cardiopulmonary bypass times and cytokine levels. Autologous whole blood transfusion has also been shown to induce cytokine release whereas autologous blood components have not [29]. We only transfused red blood cells if necessary following the first sampling for systemic cytokine levels. Ketamine attenuates the IL-6 response after open heart surgery, whereas volatile anesthetics promote gene expression of proinflammatory cytokines in alveolar leukocytes [30, 31]. Neither ketamine nor the volatile agents were used in our study.
In animal lung injury models, cytokine response to injurious ventilatory strategies is conflicting. Tremblay and co-workers demonstrated that isolated, unperfused rat lungs, whether or not exposed to previous injury, ventilated for 2 h with injurious ventilatory strategies released large amounts of inflammatory cytokines (TNF-α, IL-6, IL-1β) into the bronchoalveolar fluid [32]. In a similar rat lung model using the same ventilatory strategies Ricard et al. [27] failed to show increased TNF-α and IL-6 levels in the lungs and systemic circulation, despite ventilator-induced lung injury. In a human ARDS study, Ranieri et al. found increased levels of bronchoalveolar lavage fluid and serum proinflammatory cytokines (TNF-α, IL-6) in response to injurious ventilatory strategies and protective mechanical ventilation strategy attenuated this cytokine response [1]. In our study the lungs may not have been injured by ischemia induced by cardiopulmonary bypass, so the release of systemic proinflammatory cytokines during conventional mechanical ventilation was not significantly different from that during protective ventilation.
Another reason why serum cytokine levels were not lower in the PEEP groups, as would be expected, may be that the levels we used were not high enough. However, in coronary bypass surgery higher levels of PEEP are mostly undesirable due to the difficulties experienced during the internal thoracic artery dissection, and the fear of arterial graft compression when the chest is closed. Furthermore, an experimental study has shown that the use of PEEP in the physiological range 3–4 cmH2O may prevent lung injury by minimizing inflammation caused by ventilation [33]. Another explanation for the similar cytokine response among the groups may be the lower peak and plateau airway pressures of the patients participating in this study. Data from previous studies have shown that plateau airway pressures less than 32 cmH2O may not contribute to stretch-induced lung injury during mechanical ventilation [34].
Changes in the alveolar-arterial oxygen gradient, intrapulmonary shunt, pulmonary compliance and pulmonary vascular resistance are indicators of the pulmonary dysfunction that occurs after cardiopulmonary bypass [35]. A 40% decrease in dynamic compliance within the first 4 h and a 40% increase in alveolar-arterial oxygen gradient within the first 24 h after cardiac surgery have been observed [36]. In our study, the increase in alveolar-arterial oxygen gradient within the first 24 h was about 50% in group CV+ZEEP and the increase was less significant in the other groups, 30 and 23%, respectively, in groups PV and CV+PEEP. Taking the similar systemic cytokine levels among the groups into account, all the findings seem to be correlated with the effects of PEEP instead of proinflammatory cytokines.
The study has some limitations. The wide range of systemic cytokine levels observed in this study suggest that a larger patient population and blood sampling on a frequent basis and for a prolonged period would have yielded more reliable cytokine levels. Another limitation is that the systemic cytokine levels do not exactly reflect the bronchoalveolar fluid cytokine levels. These results are not sufficient to predict whether conventional or protective VT affect pulmonary cytokine levels in open heart surgery.
In conclusion, we could not find any evidence that protective ventilation (6 ml/kg VT) with PEEP (5 cmH2O) provides lower systemic cytokine levels, better postoperative pulmonary function and a shorter hospitalization period compared to conventional mechanical ventilation.
References
Ranieri VM, Suter PM, Tortorella C, De Tullio R, Dayer JM, Brienza A, Bruno F, Slutsky AS (1999) Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA 282:54–61
Wrigge H, Zinserling J, Stüber F, von Spiegel T, Hering R, Wetegrove S, Hoeft A, Putensen C (2000) Effects of mechanical ventilation on release of cytokines into systemic circulation in patients with normal pulmonary function. Anesthesiology 93:1413–1417
Butler J, Rocker GM, Westaby S (1993) Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg 55:552–559
Wan S, LeClerc JL, Vincent JL (1997) Inflammatory response to cardiopulmonary bypass: mechanisms involved and possible therapeutic strategies. Chest 112:676–692
Massoudy P, Zahler S, Becker BF, Braun SL, Barankay A, Meisner H (2001) Evidence for inflammatory responses of the lungs during coronary artery bypass grafting with cardiopulmonary bypass. Chest 119:31–36
Asimakopoulos G, Taylor KM, Smith PL, Ratnatunga CP (1999) Prevalence of acute respiratory distress syndrome after cardiac surgery. J Thorac Cardiovasc Surg 117:620–621
Picone A, Lutz C, Finck C, Carney D, Gatto LA, Paskanik A, Searles B, Snyder K, Neiman G (1999) Multiple sequential insults cause post-pump syndrome. Ann Thorac Surg 67:978–985
Gamble JR, Harlan JM, Klebonoff SJ, Vadas MA (1985) Stimulation of the adherence of neutrophils to umbilical vein endothelium by human recombinant tumor necrosis factor. Proc Natl Acad Sci USA 82:8667–8671
Chaney MA, Nikolov MP, Blakeman BP, Bakhos M (2000) Protective ventilation attenuates postoperative pulmonary dysfunction in patients undergoing cardiopulmonary bypass. J Cardiothorac Vasc Anesth 14:514–518
Reich DL, Moskowitz DM, Kaplan JA (1999) Hemodynamic monitoring. In: Kaplan JA (ed) Cardiac anesthesia. Saunders, Philadelphia, pp 321–358
Kotani N, Hashimoto H, Sessler DI, Muraoka M, Wang JS, O’ Connor MF, Matsuki A (2000) Cardiopulmonary bypass produces greater pulmonary than systemic proinflammatory cytokines. Anesth Analg 90:1039–1045
Cox CM, Ascione R, Cohen AM, Davies M, Ryder IG, Angelini GD (2000) Effect of cardiopulmonary bypass on pulmonary gas exchange: a prospective randomized study. Ann Thorac Surg 69:140–145
Jerrold HL, Kenichi AT (2003) Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg 75:S715–720
Kisala JM, Ayala A, Stephan RN, Chaudry IH (1993) A model of pulmonary atelectasis in rats: activation of alveolar macrophage and cytokine release. Am J Physiol 264:R610–614
Slutsky AS, Tremblay LN (1998) Multiple system organ failure: is mechanical ventilation a contributing factor? Am J Respir Crit Care Med 157:1721–1725
Zhang H, Downey GP, Suter PM, Slutsky AS, Ranieri VM (2002) Conventional mechanical ventilation is associated with bronchoalveolar lavage-induced activation of polymorphonuclear leukocytes: a possible mechanism to explain the systemic consequences of ventilatory-induced lung injury in patients with ARDS. Anesthesiology 97:1426–1433
Slutsky AS (1999) Lung injury caused by mechanical ventilation. Chest 116:S9–15
Tonz M, Mihaljevic T, von Segesser LK, Fehr J, Schmid ER, Turina MI (1995) Acute lung injury during cardiopulmonary bypass. Are the neutrophils responsible? Chest 108:1551–1556
Wan S, Marchant A, DeSmet JM, Antoine M, Zhang H, Vachiery JL, Goldman M, Vincent JL, LeClerc JL (1996) Human cytokine responses to cardiac transplantation and coronary artery bypass grafting. J Thorac Cardiovasc Surg 111:469–477
Royston D (1997) The inflammatory response and extracorporeal circulation. J Cardiothorac Vasc Anesth 11:341–354
Takata M, Abe J, Tanaka H, Kitano Y, Doi S, Kohsaka T, Miyasaka K (1997) Intraalveolar expression of tumor necrosis factor—alpha gene during conventional and high-frequency ventilation. Am J Respir Crit Care Med 156:272–279
Meldrum DR, Cleveland JC Jr, Cain BS, Meng X, Harken AH (1998) Increased myocardial TNF-alpha in a crystalloid perfused model of cardiac ischemia-reperfusion injury. Ann Thorac Surg 65:439–443
Wan S, DeSmet JM, Barvais L, Goldstein M, Vincent JL, LeClerc JL (1996) Myocardium is a major source of proinflammatory cytokines in patients undergoing cardiopulmonary bypass. J Thorac Cardiovasc Surg 112:806–811
Hennein HA, Ebba H, Rodriguez JL, Merrick SH, Keith FM, Bronstein MH, Leung JM, Mangano DT, Greenfield JL (1994) Relationship of the proinflammatory cytokines to myocardial ischemia and dysfunction after uncomplicated coronary revascularization. J Thorac Cardiovasc Surg 108:626–635
Kawahito K, Kawakami M, Fujiwara T, Murata S, Yamaguchi A, Mizuhara A, Adachi H, Ino T (1995) Proinflammatory cytokine levels in patients undergoing cardiopulmonary bypass. Does lung reperfusion influence the release of cytokines? ASAIO J 41:M775–778
Honore PM, Jacquet LM, Beale RJ (2001) Effects of normothermia versus hypothermia on extravascular lung water and serum cytokines during cardiopulmonary bypass: a randomized, controlled trial. Crit Care Med 29:1903–1909
Ricard JD, Dreyfuss D, Saumon G (2001) Production of inflammatory cytokines in ventilator-induced lung injury: a reappraisal. Am J Respir Crit Care Med 163:1176–1180
Schroeder S, Borger N, Wrigge H, Welz A, Putensen C, Hoeft A, Stuber F (2003) A tumor necrosis factor gene polymorphism influences the inflammatory response after cardiac operation. Ann Thorac Surg 75:534–537
Frietsch T, Fessler H, Kirschfink M, Nebe T, Waschke KF, Lorentz A (2001) Immune response to autologous transfusion in healthy volunteers: WB versus packed RBCs and FFP. Transfusion 41:470–476
Roytblat L, Talmor D, Rochinsky M, Greemberg L, Pekar A, Appelbaum A, Gurman GM, Shapira Y, Duvdenani A (1998) Ketamine attenuates the interleukin-6 response after cardiopulmonary bypass. Anesth Analg 87:266–271
Kotani N, Takahashi S, Sessler DI, Hashiba H, Kubota T, Hashimoto H, Matsuki A (1999) Volatile anesthetics augment expression of proinflammatory cytokines in rat alveolar macrophages during mechanical ventilation. Anesthesiology 91:187–197
Tremblay L, Valenza F, Ribeiro SP, Li J, Slutsky AS (1997) Injurious ventilatory strategies increase cytokines and c-fos m-RNA expression in an isolated rat lung model. J Clin Invest 99:944–952
Naik AS, Kallapur SG, Bachurski CJ, Jobe AH, Michna J, Kramer BW, Ikegami M (2001) Effects of ventilation with different positive end-expiratory pressures on cytokine expression in the preterm lamb lung. Am J Respir Crit Care Med 164:494–498
Tobin MJ (2000) Culmination of an era in research on the acute respiratory distress syndrome (editorial comment). N Engl J Med 342:1360–1361
Asimakopoulos G, Smith PL, Ratnatunga CP, Taylor KM (1999) Lung injury and acute respiratory distress syndrome after cardiopulmonary bypass. Ann Thorac Surg 68:1107–1115
Gott JP, Cooper WA, Schmidt FE Jr, Brown WM 3rd, Wright CE, Merlino JD, Fortenberry JD, Clark WS, Guyton RA (1998) Modifying risk for extracorporeal circulation: trial of four antiinflammatory strategies. Ann Thorac Surg 66:747–754
Author information
Authors and Affiliations
Corresponding author
Additional information
This research is partially supported by Fresenius—Kabi and Aventis Pharma.
Rights and permissions
About this article
Cite this article
Koner, O., Celebi, S., Balci, H. et al. Effects of protective and conventional mechanical ventilation on pulmonary function and systemic cytokine release after cardiopulmonary bypass. Intensive Care Med 30, 620–626 (2004). https://doi.org/10.1007/s00134-003-2104-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-2104-5