Article Text

Abstract
Background The care of infants with recurrent wheezing relies largely on clinical assessment. The lung clearance index (LCI), a measure of ventilation inhomogeneity, is a sensitive marker of early airway disease in children with cystic fibrosis, but its utility has not been explored in infants with recurrent wheezing.
Objective To assess ventilation inhomogeneity using LCI among infants with a history of recurrent wheezing compared with healthy controls.
Methods This is a case–control study, including 37 infants with recurrent wheezing recruited from outpatient clinics, and 113 healthy infants from a longitudinal birth cohort, the Canadian Healthy Infant Longitudinal Development study. All infants, at a time of clinical stability, underwent functional assessment including multiple breath washout, forced expiratory flows and body plethysmography.
Results LCI z-score values among infants with recurrent wheeze were 0.84 units (95% CI 0.41 to 1.26) higher than healthy infants (mean (95% CI): 0.26 (−0.11 to 0.63) vs −0.58 (−0.79 to 0.36), p<0.001)). Nineteen percent of recurrently wheezing infants had LCI values that were above the upper limit of normal (>1.64 z-scores). Elevated exhaled nitric oxide, but not symptoms, was associated with abnormal LCI values in infants with recurrent wheeze (p=0.05).
Conclusions Ventilation inhomogeneity is present in clinically stable infants with recurrent wheezing.
- asthma
- paediatric asthma
- lung physiology
- respiratory measurement
Statistics from Altmetric.com
Key messages
What is the key question?
Does infant lung function as reported in lung clearance index (LCI) measured from multiple breath washout improve the phenotyping of infants who have a history of severe wheezing disorders?
What is the bottom line?
LCI is elevated in a clinical cohort of infants referred for recurrent wheezing disorders suggesting persistent ventilation inhomogeneity. Elevated LCI was associated with an elevated exhaled nitric oxide and may represent an endotype of infant asthma that could not be distinguished using clinical characteristics alone.
Why read on?
Infants with severe wheezing illnesses represent a heterogeneous group of patients. Improved phenotyping using objective measures of lung function may improve our understanding of infant wheezing disorders and trajectories to chronic airway diseases.
Introduction
Asthma is the most common chronic disease of childhood. Most adults with chronic asthma trace their onset of symptoms to the preschool period. Longitudinal general population cohort studies report reduced lung function (measured by spirometry) by school age in subjects who have asthma symptoms that continue into adulthood when compared with healthy subjects.1 2 Among cohorts of children with mild to moderate asthma, these changes are more profound; nearly half had evidence of reduced lung growth in childhood, and almost a quarter had evidence of fixed obstruction by early adulthood meeting Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria for chronic obstructive pulmonary disease.3 It is unclear how early in life these lung growth changes manifest. Studies in high-risk groups, such as infants born to mothers with asthma, suggest that these decrements in lung function measurements may be present at 1 month of age in infants destined to develop asthma by school age.1 4 5 Epidemiological surveys also suggest an infantile-onset, persistent wheeze endotype that is highly associated with atopy and occurs in up to 5% of the population.6 7 Studies in clinical cohorts similarly describe a severe infant asthma endotype characterised by abnormal chest X-rays indicating pulmonary distention or atelectasis,8 which may be a sequelae of persistent airway obstruction. The site of airway obstruction is likely in the distal small airways in infants. This supposition is supported by endobronchial studies that report the absence of airway wall thickening and inflammation in the central airways9 and is consistent with findings in adults that cite the small airways as the primary site of airway inflammation.10
Previous studies in infants with wheezing disorders have focused on flow measurements that in older children may be less sensitive to changes in the small airways.11 12 The lung clearance index (LCI), a parameter derived from the multiple breath washout (MBW) test, assesses overall ventilation homogeneity and is thought to be sensitive to changes in the peripheral airways. Higher LCI values reflect greater ventilation inhomogeneity and thus worse lung disease. Limited data suggest that LCI is elevated in school-age children and adults with asthma13 even when spirometry is in the normal range.14–16 To our knowledge, there are no studies of LCI in a clinical cohort of infants with recurrent wheezing (RW) disorders.
A key limitation of previous studies describing lung function in infants with airway disease has been the lack of healthy control (HC) data.17 In this study, we prospectively collected HC data from the general population enrolled in the Canadian Healthy Infant Longitudinal Development (CHILD) study. Using a case–control design, the purpose of the current study was to explore the use of LCI as a tool to objectively phenotype lung function in a clinical cohort of infants with a history of RW who were free from exacerbation and compared them with HC from the CHILD study. We hypothesised that LCI would be elevated in RW infants compared with HC. Finally, we sought to assess the strength of the association between LCI values and clinical features of disease, as well as other physiological measures of lung function including forced expiratory flows, lung volumes and inflammation including exhaled nitric oxide.
Methods
We designed a case–control study in which infants with RW (cases) were compared with healthy infants (controls) (see online supplementary for details).
Supplementary file 1
HC infants
Healthy asymptomatic subjects participating in a general-population birth cohort, the CHILD study, were included in this sub-study of infant lung function18 (see online supplementary for details).
Infants with RW
Infants and young children aged 4–36 months with RW were recruited between June 2008 and March 2015 from the asthma clinic at the Hospital for Sick Children, a regional referral centre for severe asthma.
All studies were approved by the Hospital for Sick Children Research Ethics Board (REB # 1000011761 for Healthy Infants and REB # 1000008533 for Wheezy Infants). Written consent was obtained from parents of all subjects.
Study visits
Each child was at their baseline respiratory state of health and a minimum of 4 weeks following resolution of any acute respiratory exacerbations.
Lung function measurements
Infants were sedated with chloral hydrate (60–100 mg/kg), and lung function measurements were performed during quiet sleep in the supine position. The sequence of testing was standardised: MBW testing, followed by body plethysmography and finally forced expiratory flows using the raised volume rapid thoracoabdominal compression (RVRTC) technique.19
Multiple breath washout
MBW tests were performed using a face mask (Silkomed, Benson Medical Industries, Markham, Ontario, Canada) of appropriate size (online supplementary) sealed with therapeutic putty (Air Putty, Sammons Preston Canada, Mississauga, Ontario, Canada). A mass spectrometer (AMIS 2000; Innovision ApS, Odense, Denmark) was used with a gas mixture of sulfur hexafluoride/helium as previously described.20
Plethysmography and RVRTC
Functional residual capacity (FRCpleth) was measured by body plethysmography (nSpire Infant Pulmonary Lab, Longmont, Colorado, USA) according to American Thoracic Society (ATS)/ European Respiratory Society (ERS) guidelines.21 Forced expiratory volumes (such as FVC and forced expiratory volume in 0.5 s (FEV0.5)) and forced expiratory flow between 25% and 75% of vital capacity (FEF25–75) were measured using the RVRTC technique according to ATS/ERS guidelines.22
Exhaled nitric oxide
Exhaled nitric oxide (FENO) was measured during tidal breathing using an online chemoluminiscent analyser (CLD 88sp FENO analyser, EcoMedics AG, Duernten, Switzerland) and analysed according to ATS/ERS recommendations.23 Due to the known effects of flow on nitric oxide levels, studies in infants have reported nitric oxide levels (FENO) adjusted for minute ventilation and height.24
Statistical analysis
Subjects’ demographics were presented as median (range) for continuous variables or frequency (percentage) for categorical variables. Height and weight measurements were converted to centiles using WHO growth charts (WHO 2006) for infants and preschool children.25 Comparisons between RW and HC were performed using two-sample t tests or Mann-Whitney U tests where appropriate for continuous variables and Fisher’s exact tests for categorical variables.
The primary objective of this study was to determine whether LCI, measured from MBW, is elevated in infants with a history of wheezing disorders during remission compared with locally recruited HC. LCI values decrease in HC with age (during infancy and preschool) and with increasing height. We found that our HC had an offset in z-score values (see online supplementary); therefore, when comparing between RW and HC, we analysed the raw LCI values using a multiple linear regression model adjusted for age and height. Estimated difference and its associated 95% Confident Interval (CI) were derived from the linear regression models. We also converted LCI values to z-scores based on published reference equations26 and compared between the two groups using unadjusted linear regression model.
We also investigated other pulmonary function measures. Specifically, the RVRTC parameters and FRCpleth were also converted to z-scores based on published reference equations27 28 and compared between two groups using unadjusted linear regression models. The MBW, RVRTC and FRCpleth parameters were normally distributed and therefore were presented as mean (SD). However, the FENO values were not normally distributed and therefore reported as geometric mean values.29 In addition, when comparing between RW and HC, FENO values were adjusted for minute ventilation and height using multiple linear regression as recommended in previous publications.24 Lower limit of normal and upper limit of normal (ULN) were defined as −1.64 and 1.64 z-score, respectively.
Given the age and size difference between the RW and HC, a sensitivity analysis was conducted by matching cases and controls by the following factors: age, height, gender and ethnicity. Comparisons of the pulmonary function parameters between the two groups were repeated based on the fully matched case–control data.
To assess the strength of the association between the pulmonary function parameters and clinical characteristics within the RW group, Spearman correlation coefficients were calculated. All statistical analyses were performed using SAS V.9.4. Statistical significance was set at p<0.05. All statistical analyses were based on available data, and missing data were not imputed.
Based on previous studies of LCI in children with asthma,14 16 17 we expected a 0.6–1.0 z-score difference between RW and HC in LCI as our primary outcome. Given a sample size of 35 RW and 110 HC, we would be able to detect a 0.6 z-score difference with 80% power and 0.7 z-score difference with 90% power at 0.05 significance level.
Results
MBW measures were obtained from 37 RW and 113 HC. Children with RW already had several wheezing episodes prior to referral and were older than HC participants from the CHILD study who were recruited at birth (p<0.001) (table 1). However, the two groups had similar length and weight z-scores according to WHO standards. Paired measures of MBW and RVRTC were obtained in a subcohort with 59 HC and 24 RW infants. This subcohort was similar to the full cohort for all clinical and demographic characteristics.
Baseline anthropometrics of participants
The RW infants had multiple risk factors for asthma. The majority had at least one parent with asthma (22/37; 59%) and parental cigarette smoking (17/37; 46%). These patients reflect the referral bias of the clinic and represent a more severe form of infant wheezing than what is reported among preschool children with RW in the general population. Accordingly, they experienced a high degree of morbidity: 32 (86%) had visited an emergency department for asthma on multiple occasions (average of five visits), 19 (51%) had been hospitalised for asthma and 7 (19%) had been admitted to the paediatric intensive care unit. Consequently, most were on a moderate dose (>200 µg) of inhaled steroids on a regular basis (table 2).
Clinical characteristics of infants with recurrent wheeze (RW) and healthy controls (HC)
As to our primary hypothesis, LCI was on average significantly elevated in RW children compared with our own HC. We also found that our HC population had LCI, FEF25-75 and FRCpleth z-score values that significantly differed from the published reference populations (online supplementary table E1). We therefore examined both age and length adjusted LCI value differences as well as z-score differences between groups. After age and length adjustment, LCI was elevated by 0.48 units (95% CI 0.18 to 0.77) and 0.84 z-scores (95% CI 0.41 to 1.26) in RW infants compared with HC (table 3, figure 1, left panel). Given the age and size difference between the two groups, a sensitivity analysis was conducted by matching the two groups individually according to their age, height, gender and ethnicity. The matched subgroup was identical to the overall group for all other demographics, and similar results were found (online supplementary table E2); only LCI remained significantly elevated between RW and HC.
Infant pulmonary function parameters in healthy infants and those with RW

Left panel: estimated mean and 95% CI of LCI z-score in HC (n=113) and RW (n=37) subjects. Right panel: percentage of subjects with abnormal LCI z-score in HC and RW groups. HC, healthy controls; LCI, lung clearance index; RW, recurrent wheezers.
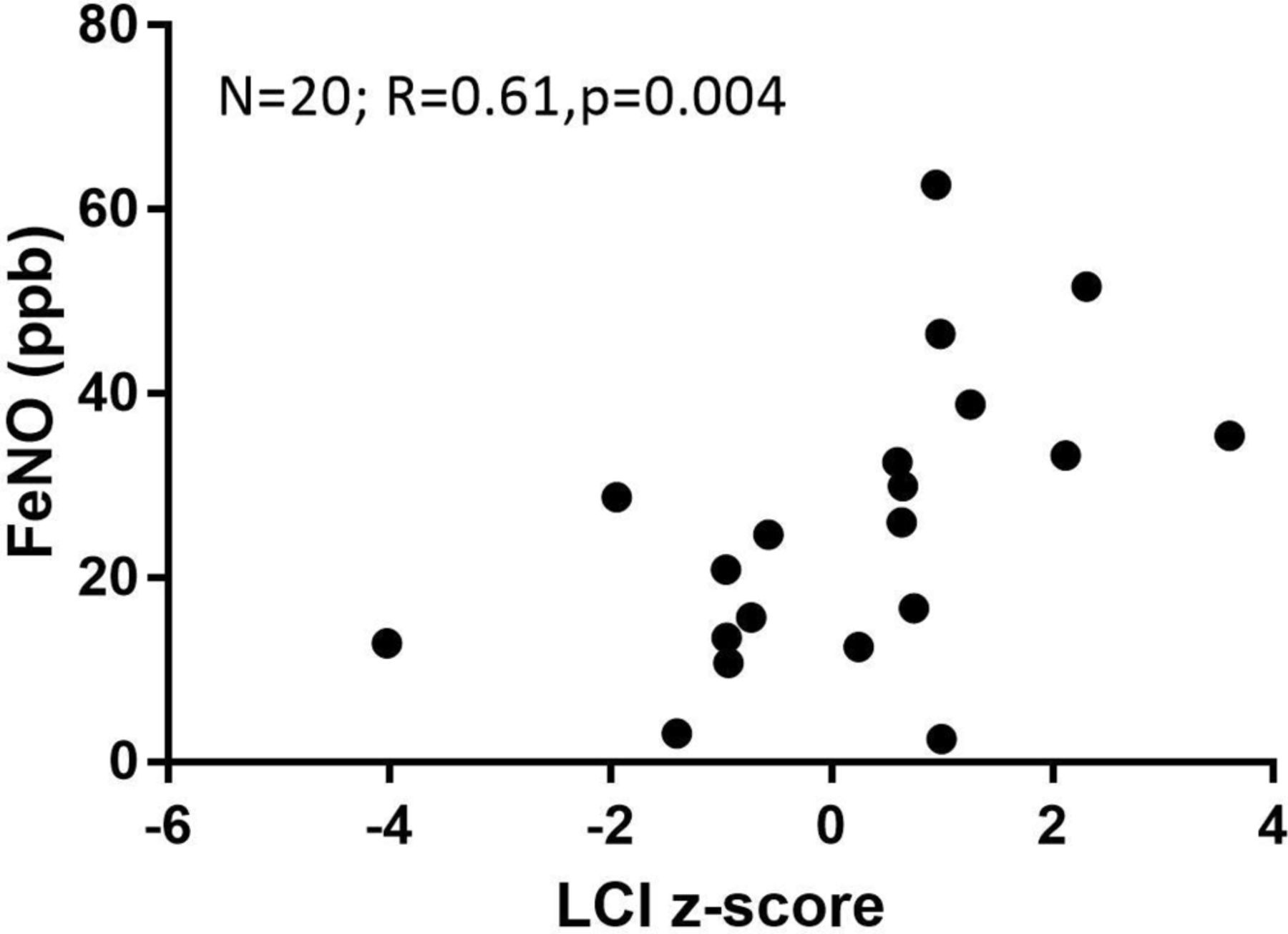
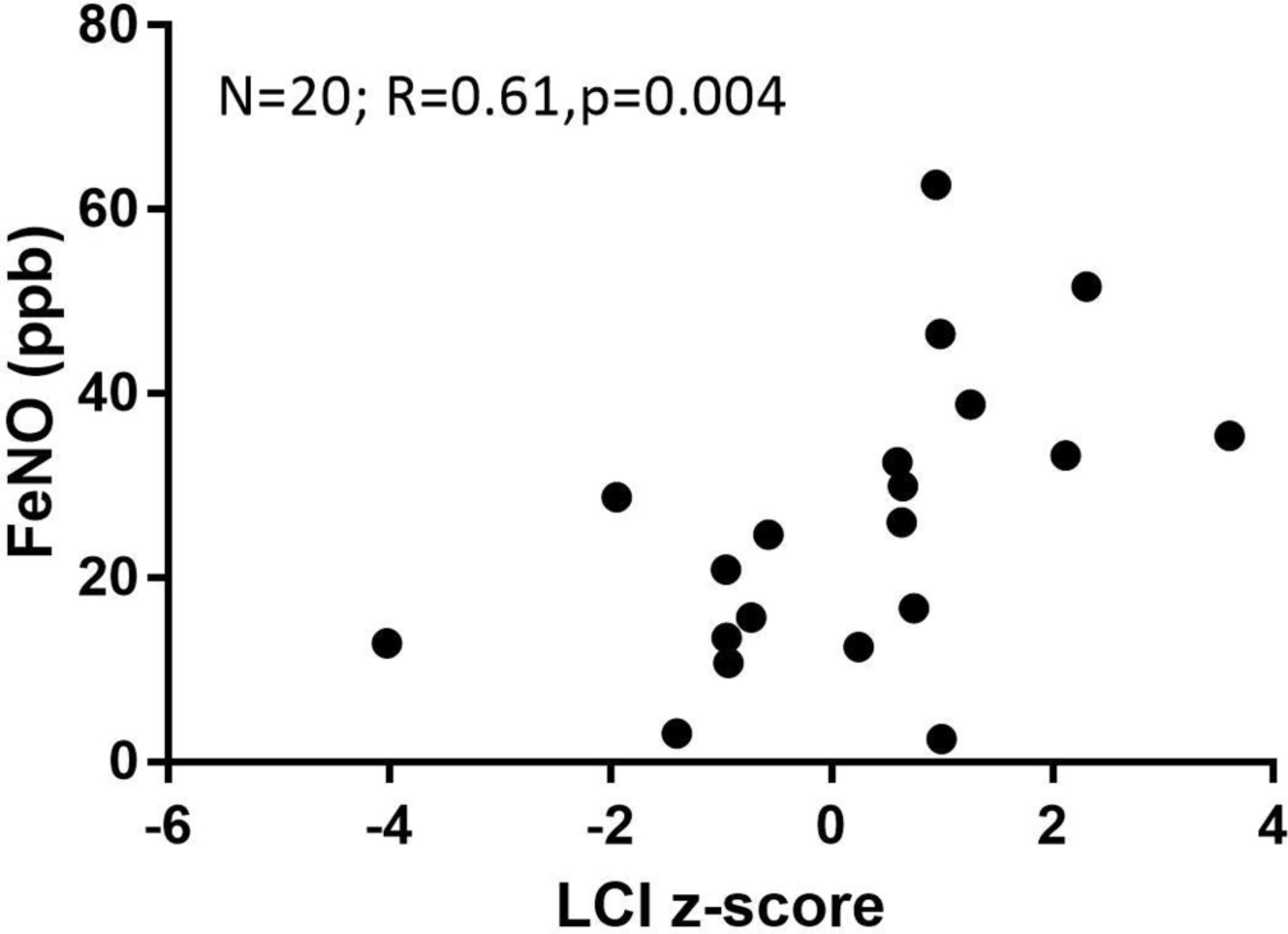
Airway inflammation, as measured by FENO, was increased in this group of treated asymptomatic RW infants compared with our HC (p<0.05). Furthermore, we found that LCI values significantly correlated with FENO (Spearman correlation coefficient R=0.61, p=0.004, figure 2).
{kind=link}
{kind=link}
Correlation between FENO and LCI values in infants with recurrent wheeze. Spearman correlation R=0.61, p=0.004. LCI, lung clearance index.
At the individual level, 7 (19%) of 37 infants with RW had an abnormal LCI value (>1.64 z-scores). Clinical factors were similar between the RW infants with abnormal LCI compared with RW infants with LCI in normal range for the following factors: parental smoking, parental asthma, markers of asthma severity (numbers of emergency room visits or hospitalizations) and current therapy. FENO values were significantly higher in RW infants with abnormal LCI values compared with RW infants with LCI values in the normal range (FENO: 39.4 (1.3) ppb vs 17.9 (2.4) ppb, p=0.05). We did not observe any differences in other laboratory markers of inflammation (blood eosinophil counts) or allergy (serum IgE levels) between RW infants with normal and abnormal LCI values (data not shown).
Relationship between LCI and other lung function measures
Direct comparison of the pulmonary function tests was challenging due to the difference in success rates in the different tests, due in part because LCI was always performed first. For participants with both MBW and RVRTC measures (59 healthy infants and 24 RW infants), LCI remained significantly higher in RW group compared with our HC (online supplementary table E3). In this subgroup, increased LCI was associated with decrements in FEV0.5 and FEV25–75 (online supplementary figure E1). Among RW infants, one infant had concordantly abnormal LCI and FEV0.5 values, three had an abnormal LCI with a normal FEV0.5 but none had the inverse (abnormal FEV0.5 with a normal LCI). None of the subjects had an abnormal FEF25–75 z-score.
Discussion
This is the first study, to our knowledge, to assess ventilation inhomogeneity in a clinical cohort of RW infants compared with HC. We found that asymptomatic RW infants have significantly elevated LCI and FENO values compared with our HC. In addition, we found that a significant proportion (19%) of RW infants had individual LCI values above the ULN. Although this rate is seemingly low from epidemiological studies, we would anticipate that only 20%–30% of infants would have persistent wheezing at school age and an asthma diagnosis. Notably, clinical risk factors for asthma such as parental history of eczema were not associated with abnormal LCI value. This suggests that LCI may able to detect a subgroup of infants with RW who have abnormal physiology and airways inflammation.
Our HC participants are similar to the general population in length and weight z-scores according to WHO standards (table 1). Despite this, the pulmonary function parameters from our HC population significantly differed from published normative data for LCI, FEF25–75 and FRCpleth. Infant pulmonary function is difficult to perform, and hence reference data are generally based on studies of limited sample size. As a result, it has been recommended that studies should recruit local HC for infant pulmonary function studies17 to eliminate potential bias due to centres or equipment differences rather than depending on historically published HC.
There are few studies of LCI in young children with wheezing disorders. Among preschool children, LCI values are elevated in symptomatic children or those with multitrigger wheezing,16 30 whereas children with a history of wheezing disorders who are asymptomatic have LCI values that are similar to HC.14 31 Only one other study has measured LCI in a general population infant birth cohort. This study showed that LCI is significantly increased in infants with prenatal tobacco smoke exposure and infants who had a lower respiratory tract infection in the first year of life,32 suggesting these changes may correlate with early structural lung impairment; however, no imaging data were available to correlate these functional tests with imaging. Ventilation heterogeneity imaging is limited in RW and asthma, but persistent ventilation defects have been noted in asthmatics children compared with HC.33 Data from studies in adults suggest that the size and location of ventilation defects tends to persist over weeks to years34 and are more commonly found in the lung periphery and correspond to areas of air trapping on multidetector CT.35 In the only paediatric study that included preschool children, there was no effect of age on the detection of ventilation defects suggesting that these peripheral defects may be present from an early age.33 Abnormalities are commonly seen in conventional chest X-rays of infants and preschool children with RW, and recent evidence would suggest that radiological abnormalities predict more severe disease.8 Longitudinal studies combining functional and imaging measures of ventilation inhomogeneity in RW infants are needed to further explore this relationship.
We did not observe significant differences in spirometric parameters between RW infants and HC in our current study. Previous studies in RW infants have shown differences in FEV0.5compared with HC.11 12 36 A number of reasons could explain this discrepancy. First, the enrolment of contemporaneous HC may affect the results. When we compared the flow parameters in our study to the reference population, we found that both groups had significantly lower flows. This illustrates the importance of including local HC data into cohorts that study patients with respiratory disease. Second, our patient cohort differed in treatment from previous datasets. Most patients referred to our clinic were already treated with an inhaled corticosteroid (ICS) at the time of test, whereas Borrego et al 12 tested a similar population of RW children prior to starting ICS. Treatment may have normalised the flow parameters (FEV0.5 and FEF25–75), reducing the difference between RW and HC. There is limited evidence that ICS can improve some flow parameters in infants.37 38
We found that FENO values positively correlated with LCI values, and FENO values were significantly evaluated among RW compared with HC. Few other papers report both LCI and FENO values, and this is the first study to report both in infants. In older children, in a study of well-controlled older children and teenagers, FENO did not differ between asthmatics and HC despite a significant difference in LCI values.14 Another study of asymptomatic children with a history of asthma showed no difference between LCI and FENO values between children with positive airway challenge tests compared with children with negative airway challenge tests. Among preschool children, results are controversial; in two studies from the same group, they found that symptomatic children or children with a history of severe disease had both elevated FENO and LCI values compared with HC.16 30 In contrast, a recent study using the commercial N2MBW system found no differences in LCI or FENOamong a group of preschool outpatient asthmatics; however, other measures of ventilation heterogeneity such as Scond were elevated in this group.39 Other infant studies have also related higher single breath FENO levels with a decline in lung function and wheeze exacerbations requiring systemic steroids.11 Imaging studies may offer some insight; Svenningsen40 reported that ventilation defects noted on MRI were more commonly reported among adult asthmatic subjects with higher FENO levels. Taken together, it is not clear whether the observed changes elevated LCI and FENO in our study reflect the difficulty in adequately assessing symptom control or reflect a more severe phenotype of asthma.
There are some limitations to this study. Performing multiple infant pulmonary function measures is challenging because of the observed effects of RVRTC on LCI.19 LCI was always performed first and thus impacted our ability to generate flow data in all of our subjects. As a result, only 60% of the HC had paired results for LCI and RVRTC. Although our main observation of significant elevations in LCI in RW infants compared with HC remains robust in the subcohort with paired measures, we are limited in our ability to comment on the relationship of LCI to other lung function measures. This also precludes our ability to comment on the relative sensitivity of different lung function measures to detect airway obstruction associated with RW. A second limitation is the lack of imaging data. Chest X-rays, although available, were not performed on the day of testing, and thus we are unable to comment on atelectatic changes that could explain these LCI abnormalities. Third, the referral pattern bias towards a more severe infant wheezing phenotype limits our ability to comment on the generalisability of the observation to non-severe infant wheeze populations. Finally, the cross-sectional design of this study precludes our ability to comment of whether these are fixed or transient changes. Although the natural history of preschool wheezing is variable and often associated with no symptoms in later life, many infants continue to have recurrent symptoms and eventually are diagnosed with asthma. Whether RW infants with abnormalities in LCI are predicted to have a more severe form of childhood asthma cannot be addressed with the current dataset and will require further longitudinal follow-up.
In conclusion, we report for the first time that LCI is elevated in a clinical cohort of infants referred for RW compared with HC. Furthermore, LCI was abnormal at the individual level in 19% of these patients and characterised a group of infants with increased FENO suggesting a more severe endotype of RW. Further follow-up of this cohort of infants is necessary to determine whether these early abnormalities persist and are predictive of a diagnosis of chronic asthma and/or a more severe infant asthma endotype. Finally, larger multicentre cohorts of wheezing infants with objective functional physiological outcomes are needed to establish the clinical utility of these tests.
References
Footnotes
Contributors PS, ABB, PJM, SET and MS designed the study. ZL, PS, MS and FR interpreted the data and drafted the manuscript. ZL and WL performed the statistical analyses. ZL, PS, REF and FR interpreted the data and revised the manuscript. KK, TJM, ABB, AD, SB and PMG collected data, interpreted results and revised the manuscript. All authors approved the final version of the manuscript.
Funding CIHR, AllerGen NCE, Don & Debbie Morrison and SickKids Foundation.
Competing interests None declared.
Patient consent Guardian consent obtained.
Ethics approval All studies were approved by the Hospital for Sick Children Research Ethics Board (REB #1000011761 for Healthy Infants and REB #1000008533 for Wheezy Infants).
Provenance and peer review Not commissioned; externally peer reviewed.