Article Text

Abstract
Sarcoidosis is a multisystem condition which may affect a number of organs and, within the cardiopulmonary system, most commonly manifests as parenchymal, airway-centred, nodal, vascular or cardiac disease. Pleural involvement is rare, but well described, and often presents as pleural effusions or pleural thickening. Here, we present the first case of active sarcoidosis manifesting as bilateral pleural calcification. We highlight the importance of a nuanced understanding of pulmonary physiology when dissecting coexistent extrathoracic and intrathoracic pulmonary restriction. We demonstrate the value of positron emission tomography scanning for identification of sites of sarcoid activity, in this case the pleura, to ensure tissue confirmation of this rare but functionally important manifestation of disease. Sarcoidosis should be considered within the differential diagnosis for patients with pleural calcification, not explained by more common causes.
- sarcoidosis
- lung physiology
- pleural disease
- interstitial fibrosis
- imaging/ct mri etc
Statistics from Altmetric.com
Anne-Marie Shanks (Specialty Doctor): A 41-year-old man presented with a 6-month history of progressive shortness of breath in the absence of cough or sputum production. He reported no features suggestive of a connective tissue disease and had no relevant environmental or occupational exposures; specifically despite detailed questioning, he had never worked, even briefly, with asbestos. The patient had no unwell contacts and denied fever or weight loss. There was no relevant recent travel history. His medical history was of a delayed diagnosis of type II diabetes complicated by peripheral neuropathy, retinopathy and ischaemic foci in the cerebral cortex. There was no history of pleural infection or intervention.
On examination, his body mass index was 26 kg/m2. He was not clubbed and there was notably limited expansion of the chest wall on inspiration. The chest was quiet to auscultation without evidence of crepitations or squawks. Oxygen saturation on air was between 80% and 85%.
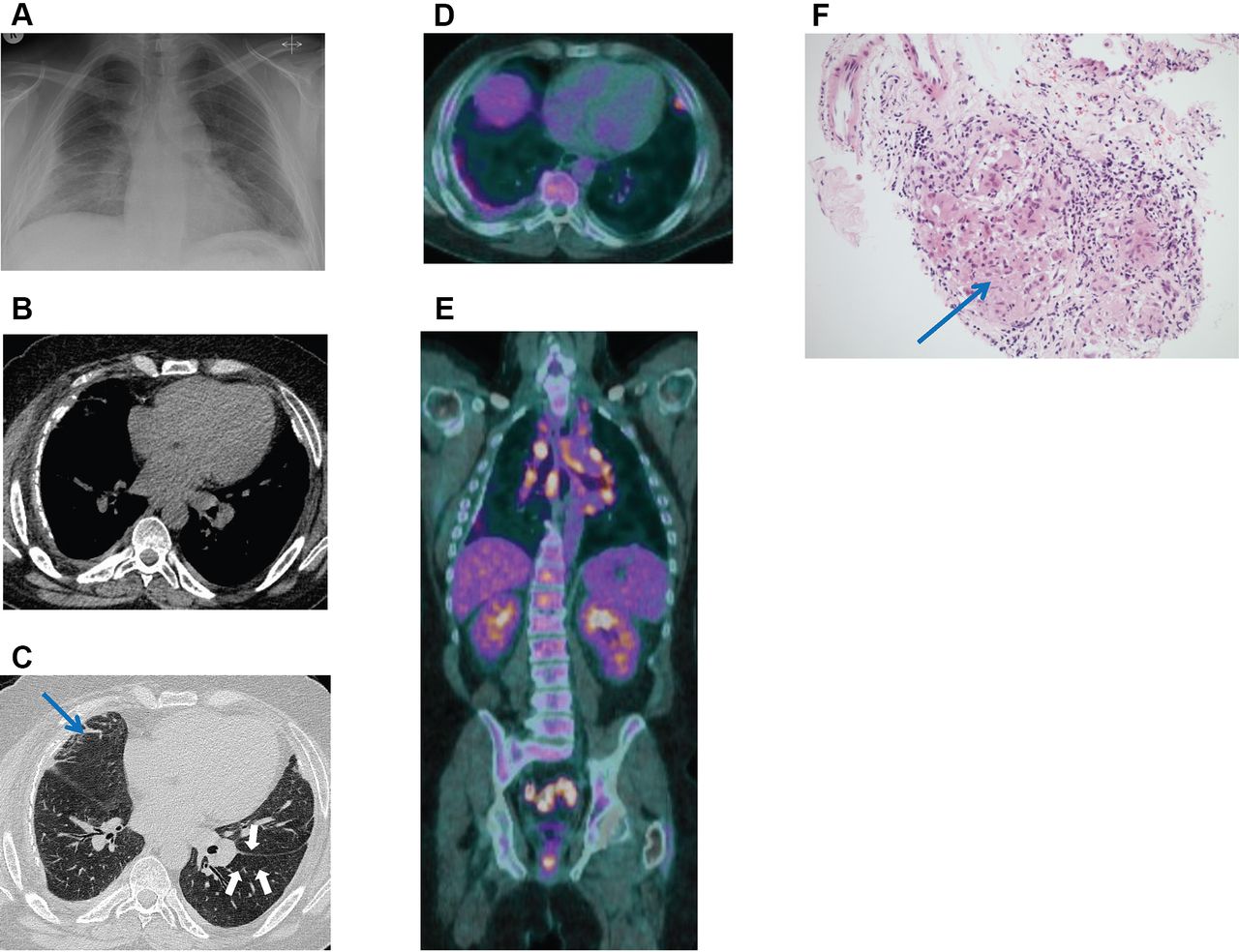
The only blood test abnormality was a mild microcytic anaemia. A chest radiograph (figure 1A) demonstrated subtle ground-glass opacification in the mid and lower zones of both lungs. Additionally, there was smooth lateral pleural thickening (partly calcified on the right) in both hemithoraces.
{kind=link}
(A) Index chest radiograph. (B) Presentation CT scan: mediastinal windows demonstrating bilateral smooth calcified pleural thickening. (C) Presentation CT scan: lung windows demonstrating bands of linear and curvilinear atelectasis extending into the lung from the visceral pleural surface (blue arrow) and a mosaic pattern containing lobular regions of decreased attenuation (white arrows). (D) PET scan: axial view demonstrating bilateral increased tracer uptake within the pleura. (E) PET scan: coronal view demonstrating multiple PET-avid mediastinal lymph nodes and pleural avidity on the right. (F) Histology from pleural biopsy demonstrating a small, well-formed non-necrotising granuloma (blue arrow). PET, positron emission tomography.
Pulmonary function tests revealed a restrictive lung deficit with an FEV1 of 1.12 L (32% predicted) and an FVC of 1.42 L (33% predicted). His carbon monoxide transfer factor (TLCO) corrected for haemoglobin was 44% predicted with a KCO of 112% predicted.
CT scan of the thorax (figure 1B–C) demonstrated a mosaic attenuation pattern without centrilobular nodules or evidence of fibrosis; in regions of decreased attenuation, there was a reduction in the number and calibre of pulmonary vessels. In addition, there was striking smooth bilateral pleural thickening with calcification and bands of linear/curvilinear atelectasis extending from the visceral pleura.
Breathing room air, he had type I respiratory failure with a partial pressure of oxygen in arterial blood (PaO2) of 6.9 kPa and a partial pressue of carbon dioxide in arterial blood (PaCO2) of 5.9 kPa, and overnight oximetry demonstrated episodic hypoventilation in a time course corresponding to rapid eye movement (REM) sleep with associated hypercapnia. Nocturnal non-invasive ventilation was initiated with supplementary oxygen at 2 L/min to maintain a target oxygen saturation range of 88%–92%.
Stephen R Thomas (Consultant Respiratory Physician): This is a difficult case because the predominant physiological abnormality observed is extrathoracic restriction, yet there is evidence of parenchymal involvement as manifest by the CT appearances. Moreover while extensive pleural thickening and calcification could have explained the restrictive physiology, the two common causes of this, prior pleural infection/surgery and asbestos exposure, were not elicited in the history. I therefore undertook bronchoscopy and transbronchial lung biopsy, which was reported as showing mild fibrosis with desquamative change with iron-containing macrophages.
Michael I Polkey (Professor of Respiratory Medicine and Consultant Physician): The transbronchial biopsy failed to demonstrate a unifying diagnosis. Hyper-IgG4 disease, a rarer cause of pleural calcification, was considered, but IgG4 levels proved normal at 0.79 g/L. Respiratory muscle weakness was also considered since this can be associated with parenchymal lung disease through the mechanism of connective tissue disease-associated interstitial lung disease (ILD), but his maximum sniff nasal pressure was 103 cm H2O (with the lower limit of normal for a man being 70 cm H2O).
The degree of respiratory failure was worrying given the patient’s location in a rural district general hospital, especially without a unifying diagnosis to guide treatment. The decision was taken to ask for advice from a tertiary centre.
Peter M George (Consultant Respiratory Physician): The patient was transferred to the Interstitial Lung Disease Unit at the Royal Brompton Hospital, London. His autoimmune serology including a myositis immunoblot was negative, as were avian and aspergillus precipitins. Serum ACE was within the normal range and vitamin D was low at 13 nmol/L. The combination of low gas transfer and hypoxaemia raised the possibilities of thromboembolic disease and pulmonary hypertension. Furthermore, the finding of haemosiderin-laden macrophages on the transbronchial biopsy meant that heart failure needed to be considered. A contrast echocardiogram excluded a patent foramen ovale and demonstrated normal left and right ventricular function with no evidence of pulmonary hypertension. A ventilation/perfusion scan was negative for pulmonary emboli.
His case was discussed at the ILD multidisciplinary team (MDT) meeting.
Sujal R Desai (Consultant Thoracic Radiologist): The plain chest X-ray shows bilateral smooth pleural thickening with calcification, and there is subtly increased density in the mid/lower zones. The non-contrast-enhanced CT confirms the presence of bilateral smooth calcified pleural thickening with bands of linear and curvilinear atelectasis extending into the lung from the visceral pleural surface. There is also a mosaic pattern containing lobular regions of decreased attenuation, for example in the right lower lobe, suggesting a component (although not dominant) of obstructive small airways disease. There are small volume discrete mediastinal lymph nodes, none exceeding 1 cm in maximum short axis dimension, although the absence of intravenous contrast makes interpretation of hilar lymphadenopathy difficult.
Alexandra Rice (Consultant Pathologist): The transbronchial lung biopsy showed very mild interstitial fibrosis with accumulation of haemosiderin-laden macrophages and very focal encrustation of pulmonary vasculature by iron. A few interstitial lymphocytes and eosinophils were present, but no granulomas were identified. The features were of mild haemosiderosis of uncertain aetiology.
Peter M George and Michael I Polkey: At the MDT, it was accepted that there was evidence of pleural disease, although it could not be demonstrated that it was of recent onset. However, a consensus favoured parenchymal lung disease because of the CT appearances and the transbronchial biopsy. There was considerable discussion as to whether the TLCO was lower than would be expected given the alveolar volume (VA).
The patient proceeded to flexible bronchoscopy and bronchoalveolar lavage (BAL). The BAL fluid microbiology was negative. The cell differential demonstrated a striking BAL lymphocytosis of 41% (<14%) (online supplementary table E1). The profound lymphocytosis suggested a differential diagnosis of hypersensitivity pneumonitis or sarcoidosis, but as it was not possible to exclude a diagnosis of lymphoma, a tissue diagnosis was sought.
Supplemental material
Pleural calcification would not be explained by any of the three diagnoses above and remained in physiological terms the predominant abnormality. It was our concern that there was an ongoing inflammatory process within the pleura, which if not diagnosed and treated had the potential to result in further lung encasement. In order to address this and to identify an appropriate site for biopsy, the patient proceeded to a whole-body positron emission tomography (PET) scan.
Sujal R Desai: The PET scan (figure 1D–E) demonstrated PET avidity in the mediastinal and hilar lymph nodes, and importantly in the regions of pleural thickening.
Peter M George: Fluorodeoxyglucose uptake within the pleura was a crucial finding and led us to proceed to a CT-guided pleural biopsy as well as an endobronchial ultrasound-guided transbronchial needle aspirate (EBUS-TBNA) of the mediastinal lymph node stations 4R, 7 and 11R.
Alexandra Rice: The pleural biopsy (figure 1F) showed dense fibrous tissue and well-formed non-necrotising granulomas overlying a small amount of lung parenchyma. The EBUS-TBNA sample also demonstrated multiple non-necrotising epithelioid granulomas. No organisms were seen on Ziehl-Neelsen and Grocott stains. The elastic van Gieson stain did not demonstrate the presence of elastic fibres.
Peter M George: The case was rereviewed at the MDT meeting and in view of the BAL lymphocytosis and the histological evidence of granulomatous inflammation within both the pleura and the mediastinal lymph nodes, a final diagnosis of pulmonary sarcoidosis was made.
Given the presence of progressive respiratory failure, the patient was treated with high-dose intravenous methylprednisolone (750 mg, 1 g, 1 g) on three consecutive days, followed by a tapering dose of oral prednisolone and an uptitrating dose of oral methotrexate initiated at 5 mg weekly.
Anne-Marie Shanks: Eight weeks after treatment with intravenous methylprednisolone, he was taking prednisolone 10 mg daily and methotrexate 12.5 mg weekly. His lung function tests were repeated and these demonstrated significant improvement in all parameters (online supplementary table E2). Supplemental oxygen was no longer required for ambulation and he had discontinued nocturnal non-invasive ventilation.
Discussion
Michael I Polkey, Anne-Marie Shanks and Peter M George: Pleural involvement is rare although described in the context of sarcoidosis,1 2 but there are, to our knowledge, no reports of sarcoidosis causing pleural calcification. Haemorrhagic pleural effusions are however described,3 and this would provide a plausible mechanism for the origin of the calcification, although there was no suggestion of this being the case for our patient. Pleural thickening associated with calcification is well recognised in patients exposed to asbestos. However, the calcification is generally more focal and discrete. A further differential for pleural thickening would be pleuroparenchymal fibroelastosis, but calcification is not a typically reported radiological finding.
PET scanning is an important but often underutilised imaging technique in sarcoidosis. It provides a means of highlighting sites of disease activity, identifies appropriate biopsy targets for diagnostic tissue confirmation and informs with regard to response to treatment.4 In this case PET scanning was critical by providing ‘reason to believe’ before undertaking pleural biopsy. When considering a possible diagnosis of sarcoidosis, this case highlights the important learning points that the serum ACE is often normal and the transbronchial lung biopsy is frequently unhelpful. In such scenarios, PET scanning can be of even greater clinical utility.
The physiology of this case was interesting as there was evidence of intrathoracic pulmonary restriction and a lymphocytic infiltrate, but also extrathoracic restriction secondary to the pleural disease. Typically with ILD, KCO is reduced due to impaired diffusing capacity of the alveolar membrane (Dm). VA is also low due to the restriction on lung inflation imposed by pulmonary infiltrates and/or fibrosis; for this reason TLCO, a calculated variable, is also reduced. In this case, there was MDT uncertainty as to whether there was a parenchymal component or if the lung physiology with a supernormal KCO could be explained purely by extrathoracic restriction. Hart et al 5 addressed this in patients with restrictive physiology, admittedly due to neuromuscular weakness (as opposed to pleural disease). Nevertheless for this purpose, pleural disease and respiratory muscle weakness are comparable in that they both impose extrathoracic restriction with normal underlying parenchyma; interestingly on the plot from that paper (online supplementary figure E1), our patient’s abnormalities could be largely explained by reduced VA.
To conclude, identifying a physiological abnormality led us to undertake the relevant imaging, which in turn led to histological demonstration of a rare condition, pleural sarcoidosis, and for the first time we report pleural calcification as a feature of this condition. Sarcoidosis should be considered when considering a patient with unexplained pleural calcification, particularly in the absence of asbestos exposure. In this clinical setting, we strongly advocate the use of PET scanning to facilitate biopsy and postulate that early initiation of immunomodulation might prevent irreversible pulmonary restriction.
Footnotes
SRT, MIP and PMG contributed equally.
Twitter Please follow Peter M George @DrPeteGeorge
Contributors All authors were involved in the clinical care of the patient and cowrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.