Article Text

Abstract
Asthma is the most common chronic condition in children worldwide. It affects daytime activities, sleep and school attendance and causes anxiety to parents, families and other carers. The quality of asthma diagnosis and management globally still needs substantial improvement. From infancy to the teenage years, there are age-specific challenges, including both underdiagnosis and overdiagnosis with stigma-related barriers to treatment in some cultures and in adolescents. Guidelines are increasingly evidence based, but their impact on improving outcomes has been negligible in many parts of the world, often due to lack of implementation. New thinking is needed to enable substantial improvements in outcomes. The disease varies globally and plans will need to differ for individual countries or places where region-specific barriers prevent optimal care. A wide selection of educational activities is needed, including community-targeted initiatives, to engage with families. The Paediatric Asthma Project Plan has been initiated to strengthen diagnosis and management of asthma. This encompasses a vision for the next 10–15 years, building on the knowledge and experience from previous educational projects. It will take into account the educational needs of patients, carers and healthcare professionals as well as the accessibility and affordability of medication, particularly in low and middle-income countries where the prevalence of asthma is rising more rapidly. This overview presents a first step for those involved in the diagnosis and management of childhood asthma to strengthen care for children globally.
- asthma
- asthma epidemiology
- asthma guidelines
- paediatric asthma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
‘Each generation is equidistant from barbarism.’
Alfred North Whitehead, mathematician and philosopher (1861–1947)
Introduction
Why is the quality of asthma diagnosis in children so universally poor? Why, despite our increased knowledge, a profusion of evidence-based guidelines and the development of effective medications, do we remain incapable of improving asthma control, and preventing asthma attacks and death, in many parts of the world? Surely, we can do better.
The word ‘asthma’ has been used in children and in adults for centuries.1 Nearly 50 years ago, just before inhaled corticosteroids (ICS) were developed, we were told that all recurrent wheezing in children fitted into ‘asthma’ and that ‘wheezy bronchitis’ in the preschool age group did not exist as a separate clinical entity.2 The pathophysiology of asthma in all ages of patients was thought to primarily involve bronchial smooth muscle hypertrophy with intermittent smooth muscle spasm.3 4 With greater knowledge of the underlying immune mechanisms,5 6 ‘asthma’ gradually became used as a term for an inflammatory condition with ICS recommended as the first-line controller7; but ‘asthma’ is now no more a diagnosis than ‘anaemia’ or ‘arthritis’ and should only be used as an umbrella term to describe a clinical spectrum that includes symptoms of wheeze, breathlessness, chest tightness and cough.6 Some have questioned whether the term ‘asthma’ should be abandoned altogether due to the increasing recognition of many different phenotypes in all age groups.8 9 However, probably better than abandoning this term is to ask the question: ‘Which of the asthmas does this patient have?’6
There have been successful attempts to improve the education of healthcare professionals, children and their families.10 However, childhood ‘asthmas’ remain poorly diagnosed, with control falling short of expected standards. The 2015 National Review of Asthma Deaths in England & Wales demonstrated that paediatric case record-keeping was worse than that in adults, the overall standard of care for children and young people being inadequate.11 The most recent asthma guidelines from the UK National Institute for Health and Care Excellence focus on recommendations for diagnosis and management of patients with mild-to-moderate asthma and are targeted at primary care physicians.12 Many issues contribute to the inability to accurately diagnose asthma in children, including failure to perform any objective tests, issues surrounding age appropriateness of tests, misunderstanding of the significance of symptoms and—especially in some areas of the world—stigma. Patients, parents and carers have misconceptions about asthma control in children13 that differ across the world.14 It is vital to recognise these differences, train local healthcare professionals and develop a comprehensive global plan that will benefit children wherever they live—an objective of the Lancet Asthma Commission.6 This overview aims to highlight the global burden of childhood asthma, recognising regional differences around the world and determine a road map to develop a training and education programme to improve the diagnosis and management of these very common conditions. While every effort has been made to provide source references for the information presented, some statements are necessarily opinion based as a definitive citation is not available.
The ‘Asthmas’
Asthma should be considered a disease with a broad clinical spectrum, making no assumptions about the underlying pathology. Airway disease should be deconstructed into components of fixed and variable obstructions, inflammation (presence and type) and infection.6 The context should be considered, including comorbidities such as obesity, and social and environmental issues. The latter include adherence and exposure to allergens and pollutants, with emphasis on identifying what is treatable.15 This approach highlights that asthma in high-income countries may not be the same as that in the high-infection, high-pollution settings that are common in low and middle-income countries (LMICs). The childhood asthmas are a spectrum of disease with similar clinical features but with wide variations in presentation, aetiology and pathophysiology.16 17 The pattern of inflammatory phenotypes is different from that in adults, with eosinophilic phenotypes predominating.18 Symptoms and markers of inflammation in children do not always correlate,19 and there are no reliable, evidence-based biomarkers for accurate diagnosis, monitoring response to therapy or risk assessment.
Prenatal factors associated with subsequent asthma inception include a family history of atopic disease, maternal smoking and asthma, environmental pollution (especially tobacco smoke and indoor biomass exposure), diet, nutrition, maternal stress, use of antibiotics and birth by caesarean section.17 In childhood, factors associated with more severe asthma symptoms and worse asthma control include allergic sensitisation (particularly multiple early aeroallergen sensitisation20–22) and exposure to high environmental levels of the allergen. Allergic conditions such as atopic dermatitis or allergic rhinitis, early severe viral respiratory infections (especially rhinovirus C or respiratory syncytial virus), decreased lung function in infancy, small family size, low socioeconomic status, antibiotic usage, infections and gender may all influence asthma severity21 23 Secondhand tobacco smoke, use of biomass fuels and air pollution are associated with an increased likelihood of attacks in those who already have asthma.24 The influence of these factors varies globally.23 24 Fortunately, smoke-free legislation has achieved substantial benefits for child respiratory health, including lower hospital admission rates and hospital attendances for asthma attacks.25 26 However, these gains are being jeopardised by the increasing promotion of e-cigarettes and the often weak responses by the legislature.
Age-specific challenges to asthma diagnosis and management
Diagnosis is particularly challenging in the first 3 years of life, both in identifying whether the child has an airway disease at all and in recognising the underlying pathophysiology.27–31 Recurrent wheezing is common but most will lose their symptoms by the age of 6 years.27 Diagnosis is made almost entirely on a clinical history of recurrent wheeze, recurrent cough for days, chest tightness, breathlessness and sometimes includes response to a trial of ICS treatment.28 These symptoms, however, do not tell us which child has which specific phenotype.28 There is no standard definition for the type, severity or frequency of symptoms in this young age group, and evidence-based recommendations are lacking.32 Should we routinely measure blood eosinophil and/or IgE levels, perform skin prick tests and attempt lung function and bronchodilator responsiveness assessments? Many of these are possible in young children, although may not be feasible in some below 3 years of age, and in resource-poor regions.33 Airway inflammation and airflow limitation are difficult to measure in young children, but all too often are not even attempted.34 This may result in undertreatment of children with eosinophilic airway inflammation and overtreatment of children with transient, non-eosinophilic wheezing.32 Undertreatment may have consequences for the child with asthma, in terms of chronic symptoms and repeated attacks of wheeze,35 36 although early intervention with ICS does not prevent progression to eosinophilic airway inflammation.37–40 Overtreatment of transient wheezing risks treatment side effects without any benefit.
Most asthma symptoms in children are intermittent and variable,7 but children may adapt their lifestyle to minimise symptoms by reducing physical activity; so it is vital that we really understand their true level of asthma control.41 Control by ICS is the present cornerstone of treatment in eosinophilic airway inflammation-driven asthma, yet poor adherence is common and remains under-recognised.42 Even with the use of short courses of oral corticosteroids (OCS) to relieve asthma attacks, there is variation in the dosage used and the length of the OCS course within the UK alone.43 There are concerns from the USA about the overuse of short courses of OCS,44 and global standardisation in future would be helpful. Intentional barriers to adherence within the family setting are common. These may have unscientific bases driven by culture-specific perceptions and medication beliefs.45 Effective education can reduce these concerns and increase willingness to accept ongoing preventative treatment. A clear strategy for early review of treatment and the management plan is essential, but rarely takes place.46
Lower airway deposition of medication can be improved by the use of a spacer,40 although poor technique occurs with most inhaler systems47 and recommendations in guidelines are not always followed.48 The high cost and lack of availability of commercially produced spacers limit their use in LMICs, although spacers made with plastic bottles can be equally effective.49 In some LMICs, access to any form of care can be lacking or care may be unaffordable.49
Teenagers often wish to take charge of their own health; some may stop medication due to stigma or embarrassment.50 Barriers to asthma management are more common in teenage boys,50 but teenage girls fare worse in overall asthma control.51 In adolescence, a lack of self-management skills and insufficient health literacy knowledge contribute to poorer outcomes and worse adherence.52 Teenagers with asthma are at risk of being neglected due to the gap in available services, and the fact that this is an age when patients do not regularly attend appointments.53 Neither paediatric nor adult clinics seem adept with the transition of care.53 Cooperation between paediatric asthma specialists and primary care physicians is essential to strengthen this transition and optimise long-term care.54–58
Identification of children whose symptoms will persist needs to be improved.9 59 The Melbourne longitudinal cohort study has followed children from 7 to more than 50 years of age.60 Those with initial severe asthma were more likely to have symptoms persisting throughout, with lung function remaining low from study enrolment.60 The Asthma Predictive Index may provide improved predictions but lacks sensitivity or specificity and has not been validated in LMIC settings.61 Among children with mild-to-moderate asthma, 75% have been shown to have abnormal lung growth in childhood, often with a further decline in early adulthood.62
Where are we now?
A plethora of asthma management guidelines have been published but healthcare providers rarely follow them, with little change in use observed over time.63 64 It is unlikely that any one guideline can be applied globally and new ideas, rather than new guidelines, are needed to improve diagnosis and management.65
Global overview
Similar challenges exist worldwide, but there are region-specific differences. There is a general lack of effective primary care, poor coordination between primary and secondary care, inaccurate diagnosis and poor adherence to treatment and failure to effectively tackle those factors that can make asthma worse. There is a tendency to progress with the use of expensive medicines without first ensuring basic management approaches have been optimised, that there has been a lack of recognition of asthma attacks and a failure of regional applicability together with implementation of simplified treatment guidelines. Only a few countries have been successful in the widespread implementation of national treatment guidelines. Shining examples of these are the Finland Asthma Project,10 the 12-year to 15-year study in Costa Rica66 and the Belo Horizonte Project in Brazil.67 Lessons from these and other regional innovative incentives still need to be shared across the globe and we will incorporate these into our educational plan. In addition, the availability and cost of medications and spacers in LMICs remain a huge barrier that could be overcome with directed resources, much in the way vaccination rates have improved in this setting.68
Asthma by geographical region
Asthma has been considered a disease of higher income countries, but this view is now obsolete, with the prevalence rising faster in LMICs.14 To better understand the global context, a group of respiratory paediatricians and healthcare professionals met in March 2017. Each was chosen for their in-depth knowledge of childhood asthma within their world region. Information was shared on the similarities and differences between world regions and proposals developed as a basis for discussion.
Africa
In Africa, like many LMICs, the burden of disease is high and outcomes are disproportionately worse among the poorest populations.14 69 Underdiagnosis and undertreatment with appropriate inhaled therapies prevail.14 69 There is a major lack of resources, poor health system infrastructure, lack of inhaled bronchodilators and corticosteroids and lack of knowledge of childhood asthma.14 69 This results in the widespread use of oral bronchodilator therapy alone. The high incidence of tuberculosis, HIV and respiratory infections hinders the accurate diagnosis of asthma.69 Poor access to care and the unavailability and unaffordability of inhaled medications and spacers are challenges.68 Outdoor pollution, exposure to secondary tobacco smoke, indoor air pollution or viral infections are highly prevalent and all precipitate asthma attacks.70
Asia
In Asia, wide disparities in care are seen, reflecting the diversity of healthcare systems. Access to care differs widely between China, Japan, the Indian subcontinent, Singapore and other Southeast Asian countries. Where access is more limited, early diagnosis is problematic and can result in years of inappropriate treatment or more likely no treatment at all. The cost of care in countries with less established healthcare systems remains a major challenge, with regular treatment unaffordable for most families.
In China, parents do not seem to recognise or understand the concept of difficult-to-treat (refractory) asthma. In Japan, there may be less concern about treatment adherence as regular doctor visits occur where repeat prescriptions are offered. Childhood asthma deaths have steadily fallen in Japan; although the death rate in China is low, the disease prevalence has increased, particularly in large cities.
Australasia and Europe
Here, the overall prevalence is high.71–73 Access to healthcare is less problematic due to well-established healthcare systems and subsidised medication costs. There are some remote sparsely populated areas where access, and accuracy of diagnosis, may be less reliable. Even where access is good, diagnosis can be wanting and the overuse of reliever treatment, underuse of ICS and lack of planned follow-up are all evident.11 74
Lung function assessment remains patchy, with little agreement on its value despite information from long-term studies.9 60 62 Even basic attention to patient inhaler technique by UK prescribers, a number of years following clear recommendations within national treatment guidelines, has been shown to be lacking.48 Similarly, the use of markers of severity or disease progression is poorly developed. Mortality is higher and more could be done for those most vulnerable in society, who are over-represented.75 Better coordination is needed among primary healthcare, hospitals, schools and child protection agencies.76 Greater patient engagement is needed, particularly during the teenage years.
There is a drive in the UK12 and Australia77 towards a better focus on phenotyping patients to improve the accuracy of diagnosis and provide tailored treatment strategies. This is particularly pertinent in the non-atopic, obese adolescent.78
South America
Asthma care here has many similarities with Asia and Africa. There is often poor access to care resulting in lack of control and increased asthma attacks, low accessibility to effective medications, weak clinical infrastructures, poor patient compliance, lack of effective education and difficult social and cultural factors. Prescriptive international guidelines do not always fit into local social and cultural backgrounds in some countries. Albarran et al suggested this could apply to the Global Initiative for Asthma guideline recommendations in countries such as Venezuela.79 The authors warned about too rigid an application of such recommendations.38 In contrast, the Wheezy Child Programme in Belo Horizonte, Brazil, showed that expensive medications are not necessary to achieve a good outcome, with the simple use of regular ICS and intermittent short-acting β2-agonists (SABAs) highly effective in reducing hospital admissions and emergency room visits in young children with asthma from 1994 onwards.67 Overdiagnosis in very young and underdiagnosis in older children are continuing themes. There is no consistent intercountry agreement about step-down treatment. The disease burden is high, multifactorial and mimics the financial and political variabilities seen in South American countries.80
North America
Children up to 3 years old tend to be underdiagnosed, while patients aged 4–11 years are more likely to be overdiagnosed. Access to therapy is strongly related to patient demographics. Rural, low-income and Latino groups have limited access to asthma specialists and conventional therapy. US drug prices are very high, making it problematic for those with no medical insurance. High prices affect the willingness of health insurance providers to reimburse for or allow the prescribing of high-cost medications. Individual healthcare systems play a major role in the philosophy of treatment, but medications may be frequently switched based on formulary recommendations and costs, confusing patients and probably affecting treatment adherence. Tracking of asthma hospitalisations is poor and lung function testing is limited. There is a need to improve identification of those at risk of attacks and to follow them up. Clinicians are aware of guidelines but only relating to the treatment steps.37
Key global challenges are summarised in box 1.
Main global challenges in paediatric asthma
Accurate diagnosis of asthma and its type (eg, eosinophilic vs non-eosinophilic)
Accessing appropriate treatment
Improving adherence to treatment
Determining the key local environmental factors responsible for triggering symptoms
Stopping the escalation of treatment along guideline steps without considering why the simple basics are not working
Adapting global guidelines to local needs and implementing these in clinical practice
Culturally appropriate training and education in childhood asthma for all
Where would we like to be?
Improving the knowledge and understanding of asthma is important and beneficial.81 82 The child and family should be at the centre of such plans, managed by well-informed local healthcare professionals and supported by regional services, including schools and town councils. The package we propose will be sensitive to local cultural attitudes as well as to the age of the child. The needs of young children and their families, and those of teenagers, are clearly very different.83
The word ‘asthma’ carries a stigma in many countries around the world, such as some South American countries, resulting in unwillingness to accept the diagnosis. In Nigeria, it is not only a stigma: parents believe it is an infectious disease, so take their child out of school when a diagnosis is made (personal communications, GF and CC). Such misconceptions can also lead to misdiagnosis and treatment with antibiotics.69 Teachers therefore need support and training in asthma within any educational package.
Policy-makers must be provided with compelling evidence to demonstrate the burden of the disease in both familial and financial terms, to ensure that improvements reach beyond locally committed clinics.84 In LMICs, increased governmental understanding of the long-term socioeconomic burden caused by failure to diagnose asthma and lack of effective treatment could result in changes in attitude about how future childhood asthma will be addressed.14 It is important to stress that huge benefits can be obtained through simple, low-cost medicines if distributed and used correctly. The basic bundle required is salbutamol and corticosteroid inhalers, oral prednisolone and a plastic bottle converted into a spacer. LMIC governments do not need to invest huge sums of money to make a big difference to asthma care.
Any asthma education plan in children needs to be age appropriate. Several initiatives have been developed to improve knowledge and self-management. One of the first was the American AIR WISE Education Program, which consisted of four weekly self-management sessions.85 It reduced the need for emergency asthma treatments through better knowledge and changes in behaviour. Similarly, the USA-based Open Airways for Schools programme aims to educate and empower children by taking a fun and interactive approach to asthma self-management.86 In Bermuda, the island-wide Open Airways programme is a model of excellence using a range of techniques, including annual assemblies and small group sessions.47 Improved adherence and control was also seen in those with persistent asthma who participated in an internet-based monitoring and education programme.87 Such new technology could provide additional means of addressing treatment adherence using connected inhalers, which record patient usage.88 Several other educational initiatives hope to provide families with information needed to manage their asthma effectively. These include the Asthma Initiative of Michigan89; the Centres for Disease Control and Prevention90; the American Academy of Allergy Asthma and Immunology 91 and the School-based Asthma Management Program.92 The National Asthma Education and Prevention Program (2003)93 provides schools with a guide to managing asthma among pupils.
What is lacking is a better coordinated approach. Lack of coordination with few well-funded initiatives in LMICs has highlighted the disparities in asthma education and resource allocation. The Asthma Drug Facility provided a great step forward in enabling access to affordable, good-quality, essential asthma drugs in LMICs; however, this initiative is no longer operational, and there is a need to establish a similar global means of ensuring equitable access to high-quality, low-cost inhaled medication. A range of educational activities could be employed, including community-targeted activities. This could take the form of active learning modules, social media or community groups (asthma clubs and church/school groups). Technology-based solutions, designed in collaboration with children, could also prove successful. A toolbox of best practice examples on how to improve asthma treatment is needed whereby local respiratory experts could provide regionally targeted input and examples before local rollout. An approach using role models or ‘Asthma Champions’ to destigmatise asthma could be particularly useful in many regions such as Africa, with delivery targeted via channels such as social media, short media service (SMS) messages, radio, television or newspapers. We could identify, for example, high-profile sports personalities with asthma who would be very strong leaders of this programme. Opinion-based publications proposing adaptation of international treatment guidelines to meet the local challenges could assist in tailoring treatment to meet the needs of the local population.
The Paediatric Asthma Project Plan
It can take 17 years for new medical practices to be adopted.94 The transfer of scientific knowledge into day-to-day clinical practice is complex and relies on a systems approach, knowledge transfer and ultimately behavioural change. We therefore need a plan with a 10-year to 15-year vision for what the diagnosis and treatment of asthma in children should look like in future. We are aware that to succeed, it will be essential that all levels of government are enthused, engaged and involved. The plan must include the educational needs of the children, their families and healthcare professionals; but also accessibility and affordability of the medicines, particularly in LMICs.
Educational interventions targeted at patients have shown limited improvements in health outcomes. Any programme would need clear patient-related outcome measures.95 Initiatives within the school setting may afford opportunities for the education of children with and without asthma, together with teachers and other staff members.90 96
We need to improve adherence to treatment and increase correct inhaler use. This can build on the US schools initiative. Health education needs to be strengthened through school-centred asthma programmes, but also within the community to educate all local children about the management of this common chronic disease. In addition, healthcare personnel need to be aware of the barriers to adherence at follow-up visits.97
We will learn from the initiatives and experiences of countries where successes have already been achieved and aim to identify their critical success factors, including those in infectious diseases such as tuberculosis and HIV.
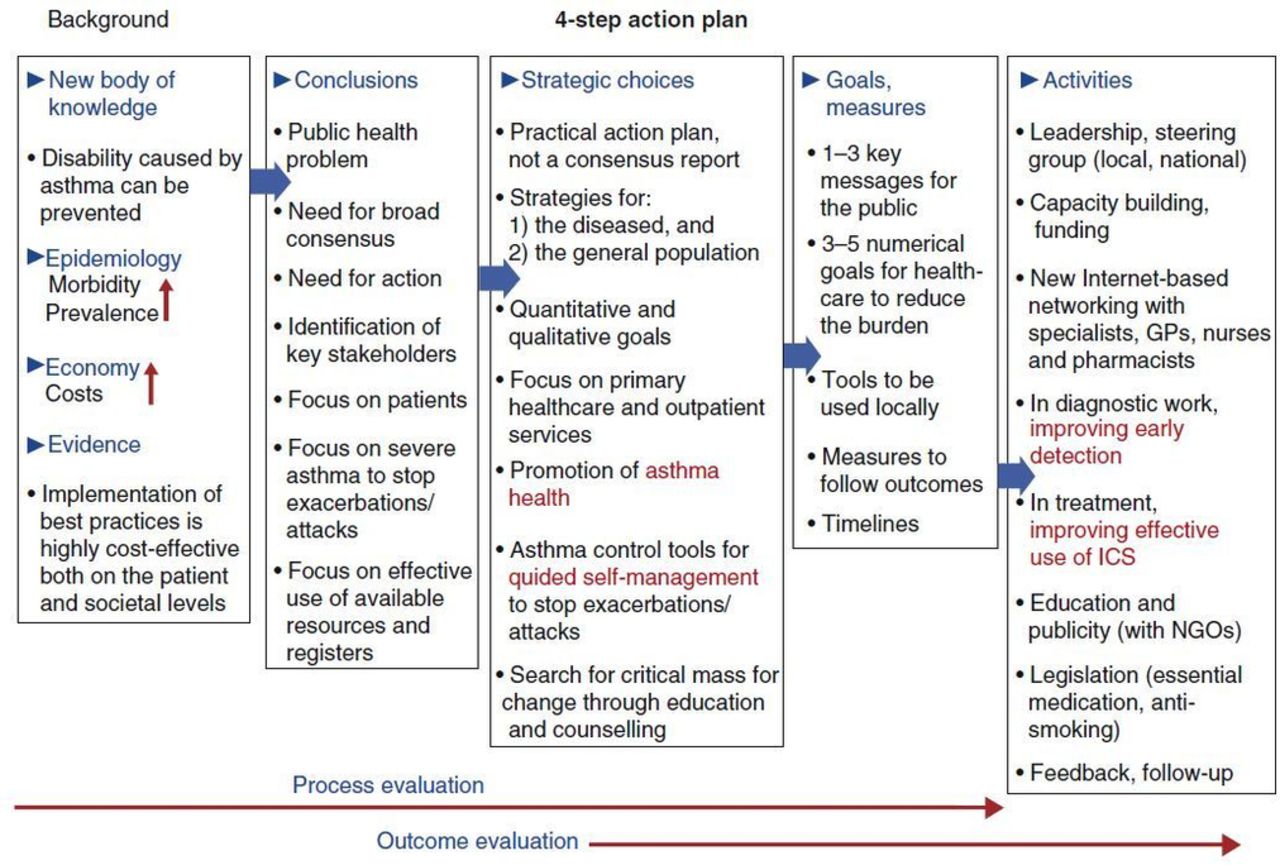
A 10-year National Asthma Programme was undertaken in Finland between 1994 and 2004 to improve asthma care. The programme’s success was achieved through earlier diagnosis, guided self-management, reduction of tobacco smoke and better patient education.10 The key features are described in figure 1.10 22 Central to their plan was the identification of primary care physicians as the key facilitators with the need for standardised education across the country. The programme reached 36 000 healthcare workers, ranging from national medical specialists to healthcare workers in the municipalities. In addition, the commitment of both political and regulatory authorities was central to the sustainability of the initiative. Different plans will be needed for different regions. Clear definitions for how to measure successful implementation of educational activities will need to be developed.98

{kind=link}
This breaks down the comprehensive asthma training programme in Finland into five distinct segments. Following better understanding of asthma knowledge, epidemiology and economics, there was recognition of a need for action, a better focus on patients and more effective use of available resources. There then followed a focus on primary healthcare improvement, the development of tools to measure outcomes and the devising of activities for diagnosis, treatment, better education and legislation.10 ICS, inhaled corticosteroid; GPs, general practitioners; NGO, non-governmental organisations.
We will develop comprehensive training templates from which countries and/or regions can select those most applicable to their locality to develop individualised training programmes ensuring continuous medical education of healthcare professionals. The establishment of clinical educational hubs will enable healthcare professionals to observe and participate in learning within a clinical setting. Teamwork and communication skills are important components. In many countries, trained nurses or other healthcare personnel have been involved in asthma management in the primary care setting. They are frequently supported by a lead primary care practitioner, often with a specialist interest, but the establishment of a team approach has been central to their success.
Educational interventions often fail by not clarifying the learning context. Learning theorists99 100 suggest that adults learn best when the topic is immediately relevant to them—through experience, and when the learning is problem-centred. Central to success is an awareness that the knowledge must be turned into a change in clinical practice. We will apply Guskey’s five steps of professional development to encourage this (box 2).101 We will also collaborate with international education groups to improve global training and education using a face-to-face ‘Teach the Teacher’ programme in various parts of the world. This would be a three-stage process drawing on the experience of successful programmes in other fields. The strategy will be: (1) establish an expert faculty with experienced teachers of primary care; (2) invite countries to participate with a group of ‘master teachers’ providing the opportunity to learn about design and implement an educational programme in their country and (3) roll out the educational programme in their respective countries.
Guskey’s five steps of professional development101
Participants’ reactions: to measure initial satisfaction with the process
Participants’ learning: to evaluate new skills and knowledge
Organisation support and change: the organisation’s advocacy, support and so on are assessed
Participant use of new knowledge and skills: degree and quality of implementation are measured
Student learning outcomes: assess student progress
Web-based education; e-learning
The development of web-based programmes and the use of mobile telephone technology will be considered as a means of delivering asthma education training programmes. These could be aimed at children, their families and/or healthcare professionals. Case-based learning can be incorporated allowing easier access and convenience for busy healthcare personnel. In addition, careful observation of emerging technology may provide additional strategies to address some problems currently associated with the delivery of effective education.
Consensus regarding treatment, identification of research needs and advocacy
Without the institution of some of the above measures, the application of isolated initiatives will have minimal impact. There is also a need to act politically to facilitate change. Working with the relevant regulatory bodies to promote accurate diagnosis, training and patient support is essential for success. We will develop these core values and plans over the coming months, with a planned rollout in late 2018.
The wider context of asthma treatment will be scrutinised. There have been many controversies and disagreements over the years. Should SABA-only treatment be the appropriate initial therapeutic approach in school-age asthma? Some guidelines suggest a trial of ICS treatment in all probable patients with asthma, but then stopped in those who show no benefit.102 What is the appropriate ICS starting dose and when do we use non-ICS-containing treatments? Which patients should be considered suitable for these approaches? A more pragmatic approach may be needed for those who exhibit seasonal asthma. Clear definitions will be needed to assess when a child is eligible for step-up treatment. Differences in clinical views are still common, compounded by lack of clinical trials in children. The presentation and management of asthma differ widely according to world region and to the patient’s age; therefore, consideration is needed to involve parents in dosing strategies and in considering the child’s ability to take medications and determine their optimal inhaler technique. By simplifying and standardising these, it might be possible to achieve better outcomes. Can we give clearer advice about step-down therapy? There are huge disparities in global views on many of these topics, leading to confusion and an inability to compare outcomes from different world regions.
Summary and conclusions
This overview is a global appeal to strengthen the diagnosis and management of childhood asthma. We have an opportunity to examine why we are failing to progress satisfactorily in many parts of the world. This impacts on patients’ health as young children and also as they become adults and indeed throughout their adult life. We have failed to work well together on a global scale and have failed to recognise that the umbrella term ‘asthma’ is unhelpful and probably should be abandoned or only used to describe a clinical symptom complex. Guidelines have been developed, but have become increasingly long and complex. They are poorly implemented by healthcare professionals and have made little impact on health outcomes in children.63 64 Our plan, though ambitious, does not involve the use of new expensive medicines, but builds on the knowledge and experience from previous educational work.101 If we implement the knowledge we have today and produce an effective training and education plan, we believe we will succeed. Incorporated into that plan, we will attempt to provide practical solutions to the questions we have raised in box 3. We will do this through consultations at a global level over the coming months.
Paediatric Asthma Project Plan—questions to be addressed
Can specific biomarkers identify children most at risk and in need of specific treatment strategies?
How best can we address poor treatment adherence?
Can guidelines be simplified for practical use in the primary care setting?
What community strategies need addressing at a global level?
What are the specific needs for low and middle-income countries?
Do we really understand the disease burden at a global level?
Can we promote the global re-establishment of an asthma drug facility to enable widely accessible and affordable high-quality asthma medications?
Acknowledgments
Professor Gilberto Fischer (GlaxoSmithKline (GSK), Brazil), Professor Jian-guo Hing (GSK, China) and Professor Yuichi Adachi (GSK, Japan) were key members of the Paediatric Advisory Board who presented their overviews on the state of diagnosis and management of paediatric asthma from their world regions and subsequently provided further information to help develop the consensus paper. They continue to be fully involved with the ongoing project. Medical writing support in the form of development of the first draft in consultation with the authors, assembling tables and figures, copyediting, referencing and graphic services was provided by Catherine Amey of Gardiner-Caldwell Communications, Macclesfield, UK, and was funded by GSK.
References
Footnotes
Contributors Drafting/revising: all authors. Final approval or publication: all authors. Agreement to be accountable for all aspects (accuracy/integrity): all authors.
Funding This study was funded by GlaxoSmithKline.
Competing interests WL is a GlaxoSmithKline (GSK) employee and GSK shareholder. AB has nothing to disclose. DAF has consulted for GSK and Merck, Sharp & Dohme. MF is a GSK employee and GSK shareholder. AO has consulted for GSK and Boehringer Ingelheim. SP reports personal fees from AstraZeneca, personal fees from Chiesi and personal fees from ALK, outside the submitted work. SJS has consulted for Aerocrine, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, GSK, Genentech, Merck, Novartis, Roche and Teva and has received research support from the National Institutes of Health, the National Heart, Lung and Blood Institute, the National Institute for Allergy and Infectious Diseases, the National Institute of Environmental and Health Sciences, the Environmental Protection Agency, the Colorado Cancer, Cardiovascular and Pulmonary Disease Program and GSK. HJZ reports grants from Allergy Society of South Africa, grants from South Africa Medical Research Council and other from GSK, outside the submitted work.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.