Article Text

Statistics from Altmetric.com
Description
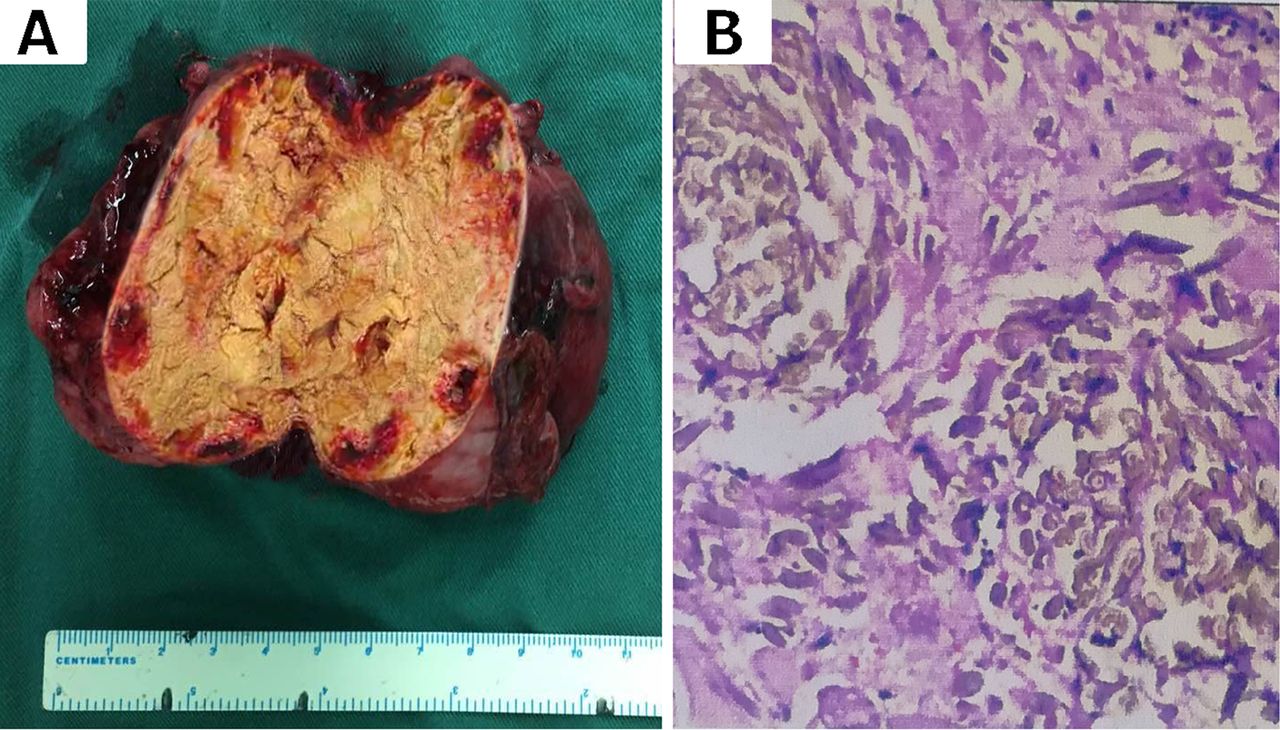
Following a 15-day history of cough with associated breathlessness, a 50-year-old woman presented with bilateral pleural effusions and a pericardial effusion. Her medical history included removal of an appendiceal cyst and a hysteromyoma resection 12 years previously. There was no cardiac or respiratory history. Physical examination revealed decreased breath sounds bilaterally with distant heart sounds heard. Pleural fluid demonstrated high levels of CA125 (2909.70 U/mL; reference range, 3.6–68.6 U/mL), cytokeratin fragment (CYFRA) (724.00 ng/mL; range, 0–3.3 ng/mL), squamous cell carcinoma antigen (SCC) (37.47 ng/mL; range, 0–1.5 ng/mL) and neuron specific enolase (NSE) (31.94 ng/mL; range, 0–16.3 ng/mL). Serum samples demonstrated high levels of CA125 (227.60 U/mL; range, 3.6–68.6 U/mL), CYFRA (6.79 ng/mL; range, 0–3.3 ng/mL), NSE (23.14 ng/mL; range, 0–16.3 ng/mL) and CA199 (39.13 U/mL; range, 0–37 U/mL). Serum markers for tuberculosis and rheumatoid arthritis were within the normal range, although C reactive protein (70.90 mg/L; range, 0–10 mg/L) and erythrocyte sedimentation rate (35 mm/hour; range, 0–20 mm/hour) were elevated. Positron emission tomography–CT (PET-CT) confirmed the presence of a hypermetabolic mass (SUVmax10.7, delay 1 hour, SUVmax14.0) measuring 10.5×7.5 cm in the abdominal cavity (figure 1), which prompted a laparotomy. At laparotomy, a 9.5×7.5×6.3 cm mass was resected and its cut surface was consistent with a surgical gauze swab (figure 2A). Histopathological examination revealed that the mass was a surgical gauze swab with features of a chronic granuloma (figure 2B). A diagnosis of gossypiboma was definitively confirmed.
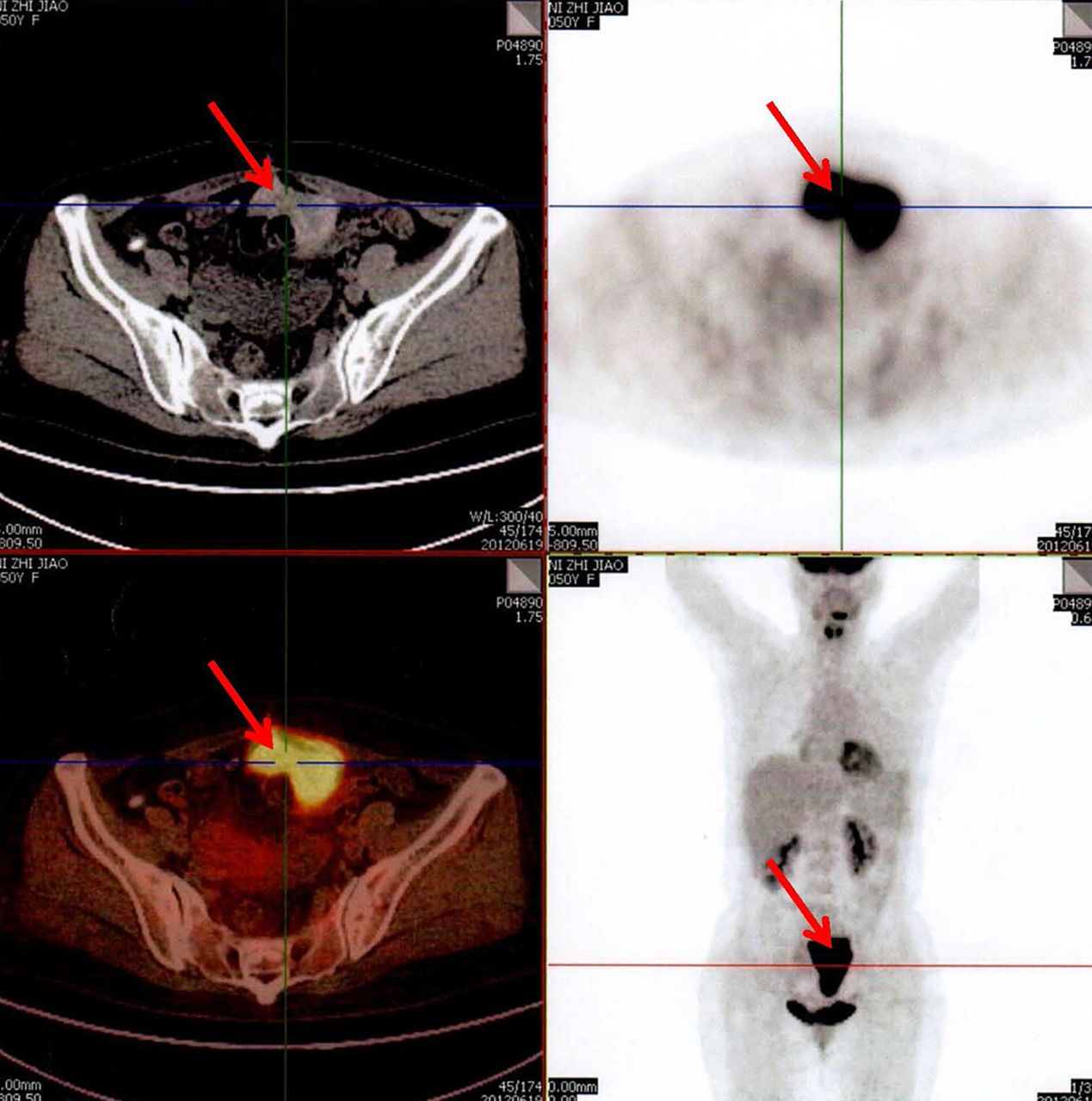
Hypermetabolic mass (red arrows) (SUVmax10.7, delay 1 hour, SUVmax14.0) identified on positron emission tomography–CT.
{kind=link}
{kind=link}
(A) Intraoperative cut surface of the mass demonstrating a retained surgical gauze swab. (B) Histopathological examinations of the surgical gauze swab with features of chronic granuloma.
The pericardial effusion and pleural effusions were observed to have resolved 1 month following surgery. In addition, tumour marker levels returned to normal, except for NSE (19.03 ng/mL). At 5 years follow-up after the operation, the patient demonstrated good recovery and absence of any lesions.
The current estimate for retained surgical swabs is one event per 10 000 procedures.1 Gossypiboma, or textiloma, is one of the most commonly retained surgical items.2 Although a correct gauze swab count at the end of a procedure may offer some reassurance, a retained surgical gauze swab can still occur.3 The highly variable manifestations of gossypiboma often prevent clinicians from making an immediate diagnosis. Although a medical history of previous surgery plays a key role in diagnosis, it was difficult to make an immediate diagnosis in this patient as the high levels of tumour markers in the serum and pleural fluid with a hypermetabolic mass on PET-CT scanning indicated a more serious diagnosis.
Clinicians must be cognisant of the association between retained surgical gauze swabs and pseudo-malignant pleural effusion. Surgical removal and histopathological examination is necessary to confirm the diagnosis.
Footnotes
Contributors All authors managed the patient. TF was responsible for writing, WW and XG for the figure and QG for the literature search.
Funding This work was supported by award from the National Natural Science Foundation of China (nos. 81770095 and 81700093).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.