Article Text

Abstract
Introduction Viral acute respiratory infections (ARIs) cause substantial child morbidity. Sensitive molecular-based assays aid virus detection, but the clinical significance of positive tests remains uncertain as some viruses may be found in both acutely ill and healthy children. We describe disease-pathogen associations of respiratory viruses and quantify virus-specific attributable risk of ARIs in healthy children during the first 2 years of life.
Methods One hundred fifty-eight term newborn babies in Brisbane, Australia, were recruited progressively into a longitudinal, community-based, birth cohort study conducted between September 2010 and October 2014. A daily tick-box diary captured predefined respiratory symptoms from birth until their second birthday. Weekly parent-collected nasal swabs were batch-tested for 17 respiratory viruses by PCR assays, allowing calculation of virus-specific attributable fractions in the exposed (AFE) to determine the proportion of virus-positive children whose ARI symptoms could be attributed to that particular virus.
Results Of 8100 nasal swabs analysed, 2646 (32.7%) were virus-positive (275 virus codetections, 3.4%), with human rhinoviruses accounting for 2058/2646 (77.8%) positive swabs. Viruses were detected in 1154/1530 (75.4%) ARI episodes and in 984/4308 (22.8%) swabs from asymptomatic periods. Respiratory syncytial virus (AFE: 68% (95% CI 45% to 82%)) and human metapneumovirus (AFE: 69% (95% CI 43% to 83%)) were strongly associated with higher risk of lower respiratory symptoms.
Discussion The strong association of respiratory syncytial virus and human metapneumovirus with ARIs and lower respiratory symptoms in young children managed within the community indicates successful development of vaccines against these two viruses should provide substantial health benefits.
- respiratory infection
- viral infection
- clinical epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
What is the attributable risk for symptoms of acute respiratory infections (ARIs) when specific respiratory viruses are detected by PCR assays in nasal swab samples collected weekly from otherwise healthy young children?
What is the bottom line?
Attribution for ARIs by specific viruses was strongest for respiratory syncytial virus and human metapneumovirus in young children with lower respiratory tract infections, while among DNA viruses tested, only adenoviruses were significantly associated with an increased risk of symptoms.
Why read on?
The virus-specific attributable risk of ARIs is a population-level metric to inform causal inference in the aetiology of ARIs and provides quantitative estimates of the relative proportions of virus-associated ARIs in the community, yielding important insights for prioritising public health interventions.
Introduction
Viral acute respiratory infections (ARIs) are a common cause of morbidity in children, either on their own or in synergy with bacterial pathogens.1 Virus-positive ARIs early in life are associated with developing wheeze and asthma during childhood and adolescence.2 Community-based studies from the 1950s to 1960s examining the aetiology of ARIs by traditional laboratory detection methods remain the template for understanding childhood respiratory virus epidemiology.3 Advances in molecular diagnostics, including PCR testing, have improved virus detection in those with ARIs.4 However, this increased test sensitivity has also resulted in viruses being detected in asymptomatic individuals.4 5 The clinical significance of finding respiratory viruses is not always straightforward, and a better understanding of the proportion of infections that are symptomatic for individual viruses is needed.
The attributable fraction in the exposed (AFE) provides information about the percentage of cases among exposed individuals that can be attributed to the exposure. In our study, the AFE measures the percentage of ARIs in virus-positive children attributable to that particular virus. The AFE does not inform on the aetiology at an individual level, but is a key population-level metric for interpreting positive specimen results. It assists with estimation of the true burden of disease, thus guiding preventative strategies for respiratory infections, such as immunisation. Virus-specific AFE estimates for ARI in children are reported infrequently, with most studies reporting AFEs having important methodological limitations. Except for one community study,5 these investigations recruited either highly selected hospitalised children or outpatients as study cases,6–8 or used controls from outpatient clinics.6 7 A meta-analysis of 23 studies that calculated virus-specific AFEs included 22 studies employing hospital-based case ascertainment and only three using community-based controls.9 Other studies comparing symptomatic and asymptomatic groups calculated odds ratios (ORs),10–12 or relative risks,13 without calculating AFEs. Moreover, several studies focused solely either on specific viruses10 12 or outcomes.6 11–13
Longitudinal, community-based studies employing sensitive molecular-based assays with regular and frequent sampling, irrespective of illness, are best suited to explore the relationship between respiratory virus detections and ARI symptoms, especially as they represent most ARI episodes. The aim of our study was to examine the disease-pathogen associations of respiratory viruses in infants participating in a community-based birth cohort project14 and to calculate their virus-specific AFE values.
Methods
Study population
The Observational Research in Childhood Infectious Diseases (ORChID) project (clinicaltrials.gov: NCT01304914) is an observational, longitudinal community-based birth cohort study of ARI episodes in children until their second birthday.14 Participants were able to leave the study temporarily (such as during family holidays) and rejoin at a later date. It was conducted in the subtropical city of Brisbane, Australia (latitude 27° South, average monthly maximum temperature range 22°C–30°C, maximum rainfall in December-February, population 2.2 million) between September 2010 and October 2014. Parents consented antenatally for their child’s participation. For enrolment, infants needed to be healthy, without congenital abnormalities or underlying chronic disorders, and to be born at term (36–42 weeks). Recruitment was progressive over 2 years at one of two metropolitan hospitals (one private and one government-funded). Detailed methods of recruitment, study design and sample and data collection are described elsewhere.14 The Children’s Health Queensland, Royal Brisbane and Women’s Hospital, and The University of Queensland Human Research Ethics Committees approved the study.
Sociodemographic and clinical characteristics
Following recruitment, parents provided their sociodemographic and health history, pregnancy and birth details. Telephone interviews were conducted every 3 months to update immunisation, feeding and childcare attendance details. Childcare was categorised as formal (regulated care outside the child’s home) or informal (non-regulated care provided by family or friends).15 The duration of exclusive breast feeding was from birth to the introduction of either any milk formula or solids.
Symptom data collection
Parents were trained to recognise respiratory symptoms and provided with diary cards designed in a tick-box format and listed with predefined respiratory symptoms or diagnoses to be completed daily and returned by regular mail monthly. The diary cards were modified from a prior study16 and used successfully elsewhere.17
Virus detection
Viruses were identified from parent-collected anterior nose swabs at the infant’s birth, and weekly thereafter.18 Specimens were mailed to the laboratory, taking a median of 3 (IQR 2–4) days, and where they were processed and stored at −80°C until further analysis.14 19
Swabs were batch-tested for 17 respiratory viruses: human rhinovirus (HRV), influenza A and B (IFV-A, IFV-B), respiratory syncytial virus A and B (RSV-A, RSV-B), parainfluenza viruses 1–3 (PIV-1, PIV-2, PIV-3), human coronaviruses (HCoV) OC43, NL63, 229E and HKU1, human metapneumovirus (HMPV), adenovirus (AdV), human polyomaviruses WU (WU-PyV) and KI (KI-PyV) and human bocavirus-1 (HBoV-1), using previously validated real-time PCR assays.14 Details of sample collection, processing, PCR assay parameters, quality control measures and HRV typing into species A, B and C are outlined in the online supplementary text and E-table 1. Specimen quality was assessed by testing for a marker of human genomic DNA, endogenous retrovirus-3 (ERV-3).20 Swabs with ERV-3 cycle-threshold (Ct) values >38 (including undetectable Ct values) were deemed to be of lesser quality and excluded from parts of the analysis.21
Supplementary file 1
Definitions
New virus detection episode
When a new virus (different virus or new species/subtype of the same genus or species, respectively) was detected in a swab by PCR testing, or the same virus was detected after at least two negative intervening swabs, or the same virus was detected at least 30 days from the last positive swab.
Symptomatic new virus detection episode
When symptoms were reported 7 days before or 7 days after detecting a new virus.
ARI episode
ARI was defined as a new episode of respiratory symptoms of the upper and/or lower respiratory tracts demarcated by a window of ≥3 symptom-free days.17 22
Upper respiratory tract infection
Parent-reported runny nose/nasal congestion, dry cough or doctor-diagnosed otitis media.22
Lower respiratory tract infection
Parent-reported rattly breathing, moist cough, shortness of breath, wheeze or doctor-diagnosed pneumonia.22
ARIs were subcategorised hierarchically as either a lower respiratory tract infection (LRTI) or upper respiratory tract infection (URTI), respectively.
Analysis
The incidence rate of single new virus detection episodes (VDEs) per 100 child-years was calculated using Poisson regression. To account analytically for the differing lengths of time children remained in the study, the natural logarithm of the number of swabs returned was included in the model as an offset. Swabs were removed from incidence rate calculations for individual viruses when the participant was not at risk of a new VDE (a positive consecutive swab following the initial positive swab, and two swabs after the last positive swab, as per our definition of a new VDE), or the swabs were of lesser quality (to avoid underestimating incidence rates).21 When calculating incidence rates for ‘any virus’, we assumed children were at risk of being positive for new viruses in every swab.
The virus-specific risk and AFE of single VDEs in cases of ARI and LRTI were estimated using a generalised linear model with binomial family and log link. Robust variance estimates were calculated using sandwich estimators to account for repeated measures within children. We analysed LRTIs separately as children with these infections are more likely to visit family physicians, present to hospital and receive antibiotics.22 The AFE was calculated as 100%×(1−RR−1), where risk ratio (RR) is the proportion of children positive for a virus with ARI symptoms, divided by the proportion of children negative for the virus who have ARI symptoms (see online supplementary text 2). Only virus-negative swabs of lesser quality (Ct >38) were excluded in these analyses of association, as swab quality of positive swabs did not modify the association between VDEs and ARI symptoms (see online supplementary E-table 2).
The association between potential risk factors (age, sex, type of delivery, gestational age at birth, season, family history of asthma or eczema, tobacco smoke exposure, household size, maternal education status, mode of feeding, category of childcare attendance) and symptomatic and asymptomatic virus detection was examined using mixed-effects logistic regression with the child entered as a random effect to account for repeated measurements within children. Both univariable and multivariable analyses were conducted. Breast feeding and childcare attendance were analysed as time-varying variables. Multivariable models included all the above risk factors with no forward or backward selection. Only virus-negative lesser quality swabs were excluded in these analyses. As it was not possible to determine individual virus contributions to ARI symptoms during virus codetections, samples with more than one virus detected were analysed descriptively (see online supplementary E-table 3). Data were analysed using Stata V.12.1 (StataCorp, College Station, Texas, USA).
Results
Cohort characteristics
Of 891 potential participants approached, 165 (18.5%) eligible singleton infants from 163 families were enrolled (two families enrolled two siblings) (figure 1). Seven were excluded subsequently; one from ineligibility (born <36 weeks) and six for failing to provide any swabs. Of the remaining children, 158 provided 11 125 swabs (figure 1; 68.3% of maximum expected; median 84.5, range 1–104) from birth until their second birthday, and 154 infants provided 87 547 child-days of symptom diaries (77.9% of maximum expected days; median 726 (range 1–730 days)) with 67% followed until at least age 23 months (see online supplementary E-figure). One or more respiratory symptoms were recorded on 16 877 (19.3%) days, and corresponded to 1641 discrete ARI episodes.

Submission of nasal swabs and symptom diaries from participants in the Observational Research in Childhood Infectious Diseases study. Ct, cycle threshold; ERV-3, endogenous retrovirus-3.
Demographic and social characteristics are reported in table 1. Compared with the general population of Brisbane and the state of Queensland, study children were from smaller families of advantaged backgrounds (see online supplementary E-table 4).
Characteristics of children enrolled in the Observational Research in Childhood Infectious Diseases study
Virus detections
When calculating incidence rates, of the 11 192 total swabs submitted by all children, 3025 (27.2%) lesser-quality swabs (346 virus-positive and 2679 virus-negative) were removed from the analyses, as were 67 swabs submitted after the child’s second birthday, leaving 8100 swabs from 157 infants (figure 1). Overall, 2646/8100 (32.7%) swabs were positive for respiratory viruses (table 2), of which 1520 were new VDEs.
Respiratory viruses detected in 8100 high-quality nasal swabs collected from 157 infants from the Observational Research in Childhood Infectious Diseases (ORChID) birth cohort in the first 2 years of life. Incidence rates/100 child-years presented overall, and for the first and second years of life separately
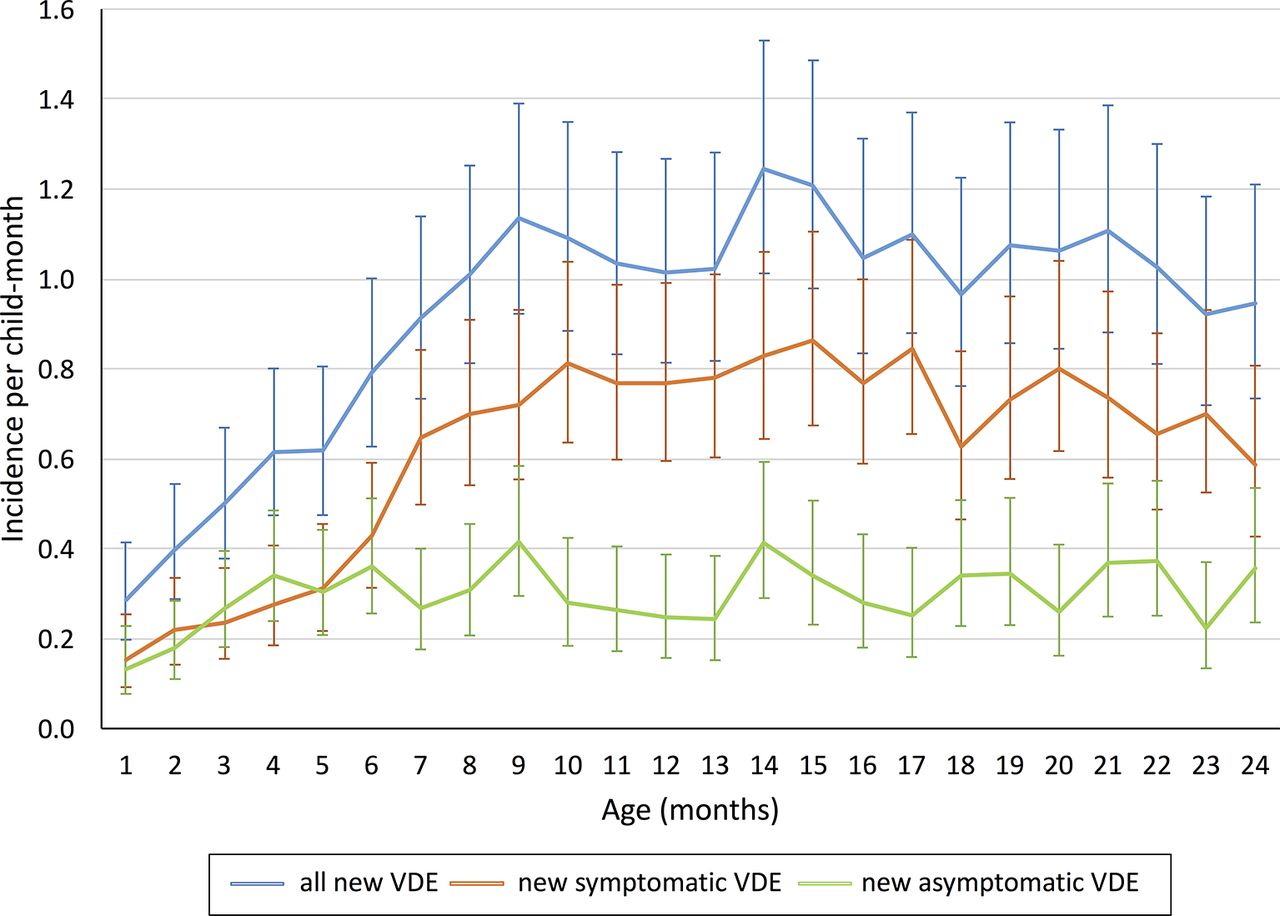
The incidence of new VDEs increased in the first 9 months of life, with symptomatic episodes dominating after 6 months of age (figure 2). There was an overall incidence rate of 978 new VDEs per 100 child-years (95% CI 930 to 1029, table 2). More than one virus was detected in 275/8100 (3.4%) specimens. HRV was the most commonly detected virus (2058/2646 detections, 77.8% of all positive detections, mean rate of 1002 new VDEs per 100 child-years, 95% CI 942 to 1066), followed by HBoV-1 (60 new VDEs per 100 child-years, 95% CI 49 to 73) and KI-PyV (56 new VDEs per 100 child-years, 95% CI 45 to 69) (table 2).
{kind=link}
{kind=link}
Incidence rate of new virus detection episodes per child-month by age and type of infection (n=151). VDE, virus detection episode.
Virus-positive ARIs and asymptomatic episodes
When considering virus-positive ARIs and asymptomatic episodes, we retained 346 virus-positive swabs with ERV-3 Ct values >38, but removed a further 244 swabs with missing symptom data, to give a final dataset of 8202 swabs from 151 participants (3 participants submitted swabs of high or no Ct values or swabs with no corresponding symptom data before withdrawing early in the study) (tables 3–5).
Acute respiratory infections and asymptomatic single new virus detections, risk ratios and attributable fractions by respiratory virus in 151 children from the ORChID birth cohort (n=8202)
Lower respiratory tract infections and asymptomatic single new virus detections, risk ratios and attributable fractions by respiratory virus in 151 children from the ORChID birth cohort (n=5267 swabs)
Number of children, child-months, virus-associated symptomatic and asymptomatic episodes and association between participant characteristics and acute respiratory infections in 151 children
Of 8202 swabs, 3894 (47.5%) were taken during symptomatic periods and 4308 (52.5%) from asymptomatic periods. Of all swabs taken any time during symptomatic periods, 1903/3894 (48.9%) were positive for a virus, and 1120/3894 (28.8%) were new VDEs. Overall, 984/4308 (22.8%) swabs taken during asymptomatic periods were positive for a virus, of which 562 (57.1%) were new VDEs and 491/562 (87.4%) were new single virus detections (tables 3 and 4).
Table 3 shows that for new VDEs involving only single viruses, HRV-A, HRV-C, IFV-A, PIV-3, RSV-A, RSV-B, HCoV-OC43, HCoV-NL63, HMPV, and AdV had statistically significant, positive AFE values, indicating they were significantly more often associated with ARI episodes than asymptomatic periods. In contrast, HCoV-229E, HCoV-HKU1, WU-PyV, KI-PyV, and HBoV-1 were frequently detected in asymptomatic periods and had low point estimates for AFE, indicating they were less likely to have caused the ARI.
Of the total 1641 ARIs, 111 (6.8%) did not have swabs submitted during the ARI episode, including swabs taken 7 days before or 7 days after the last day of the illness. Of the remaining 1530 ARIs, 1154 (75.4%) ARIs (935 (81%) URTI, 219 (19.0%) LRTI) had ≥1 swabs with a virus detected during this period.
RSV and HMPV were more strongly associated with LRTI than asymptomatic detections (table 4), with higher risk ratios than other viruses. While significant, the association between LRTI and HRV-C, HCoV-OC43 and PIV-3 detection was weaker. Interestingly, codetected specimens had among the strongest AFE values for both ARIs and LRTIs (tables 3 and 4), with HRV the most frequently detected virus group, usually in combination with DNA viruses (see online supplementary E-table 3).
To investigate the sensitivity of results from including lesser quality swabs, we reanalysed the data by excluding 346 virus-positive swabs of lesser quality, and found minimal change to the AFEs calculated in tables 3 and 4 (see online supplementary E-table 2).
Viruses and association with risk factors
Independent risk factors associated with symptomatic rather than asymptomatic VDEs, included increasing age, particularly after 6 months, and virus infections during non-summer seasons (table 5). The regression model revealed childcare attendance was also independently associated with higher rates of VDEs, both symptomatic and asymptomatic, but no other risk factors were found to be associated with asymptomatic VDEs.
Discussion
Healthy children in the ORChID community-based birth cohort experienced an incidence rate of 978 new VDEs per 100 child-years during the first 2 years of life, with HRV playing a dominant role. Overall, respiratory viruses were detected by PCR in regular weekly swabs at least once during 75% of ARIs, while in asymptomatic periods 23% of weekly nasal swabs were positive by PCR for respiratory viruses, accounting for 33% of all new VDEs. We demonstrated evidence of attribution for ARIs by RNA viruses, which included HRV (HRV-A, HRV-C), influenza (IFV-A), parainfluenza (PIV-1, PIV-3), RSV (RSV-A, RSV-B), HCoV (HCoV-OC43, HCoV-NL63) and HMPV; and AdV as the single DNA virus representative. All these viruses were detected significantly more often in children with an ARI than during asymptomatic periods and had statistically significant positive AFEs. The largest association was observed for RSV and HMPV, both of which were more strongly associated with LRTIs than other respiratory viruses. Increasing age ≥6 months, non-summer months and childcare attendance were independent risk factors for symptomatic VDEs. Age as a host risk factor for symptomatic infection is also noted in other studies,23 and is presumably due to protection afforded by maternal transplacental and breastmilk antibodies in the very young.24 Environmental risk factors of season and childcare attendance for ARIs may be related to the intensity and opportunity for exposure in these settings experienced by young children.10 25
The virus-specific attribution of ARIs was quantified by identifying VDEs during asymptomatic periods and calculating the virus-specific AFE, an infrequently reported metric for helping to determine the relative causal roles of different viruses at a population level. A limitation of the AFE approach is that it cannot inform on the aetiology at an individual level: in individual cases it does not differentiate between those with a true positive test identifying the virus responsible for the ARI and those with a false positive result from asymptomatic virus shedding. Nevertheless, knowing the AFE for respiratory viruses can help inform clinicians on the likely clinical significance of detecting one or more viruses in nasal swab specimens taken from infants or young children during an ARI episode, by assigning the group aetiological fraction for viruses detected in that child. Importantly, AFE estimates can be applied to studies of ARIs in different settings to estimate the true burden of disease in the community, thus informing which viruses should be prioritised in future public health policies and interventions.
Most previous studies have overestimated AFE values by using ORs, rather than RRs, in calculations.5 6 8 9 ORs overestimate the effect size when the event is not rare, as occurs with ARIs in children. These studies are principally cross-sectional, hospital-based and often have poorly matched controls. Consequently, our estimates of AFE being lower than reported elsewhere is not surprising, and, we believe, are likely to provide more accurate estimates of the ARI and LRTI burden attributable to these viruses in the broader paediatric population.
The proportion of asymptomatic infections in our study highlights the risks of extrapolating hospital-based data from sick children to the community setting. Previously, the significance of detecting viruses by PCR was tempered by concerns that this may be from an incubating or unrelated subclinical infection or represent continued virus nucleic acid shedding from a recent ARI that has resolved. The intensive longitudinal specimen and symptom sampling from our cohort, as well as the definitions of VDEs and symptomatic VDEs used, helped identify nascent and subclinical infections. In this context, our observations emphasise the frequency of subclinical infections by respiratory viruses in young children, who when otherwise well, may act as important ‘silent’ reservoirs of infection. Similar observations and conclusions were reported recently in a household study involving both child and adult contacts of symptomatic cases of laboratory-confirmed influenza.26 Nevertheless, in addition to influenza, established viruses, such as HRV, PIV-3, RSV, and HMPV are also important community respiratory pathogens, especially the latter two viruses, and potential candidates for vaccine and other therapeutic interventions.27 This contrasts with the novel DNA viruses, HPyVs and HBoV-1, which have low AFEs calculated for both ARIs and LRTIs, despite their higher detection rates.28 29 However, as suggested by this cohort, synergy may exist between multiple viruses causing ARIs. Unexpectedly, this involved mostly HRV and DNA viruses, and this finding warrants further study.
Strengths and limitations
The 78% of expected child-days and 68% of expected swab returns was a very good retention rate given the intensive and prolonged nature of the study for participating families. Analysis of incidence rates of ARI in participants that withdrew from the study at different periods showed no clear association between time of dropout and ARI incidence. Regular parent-collected nasal swabs avoids the need for home visits by research staff or clinic attendance during an ARI, minimising possible biased estimates of ARI events and specimen availability from losing families failing to seek healthcare. Moreover, regular weekly nasal swab collections increase the likelihood of virus detections during an ARI episode rather than relying simply on results from a single specimen. Our previous work found that with sensitive PCR techniques, parent-collected nose or nose-throat swabs sent to the laboratory by standard mail had comparable sensitivity to nasopharyngeal swabs obtained by healthcare workers.18 19 30 Longitudinal data collection also allows assessment of asymptomatic status by considering past and future illness history, as some viruses are detectable days before and after ARI symptoms develop,31 and are therefore less likely to yield false-positive findings.
There are also some important limitations to consider. To reduce the chances of false-negative test results,21 we excluded from analysis 2679 (23.9%) swabs where the internal control for human DNA, ERV-3, was either undetected or present at very low levels. We excluded both virus-positive and virus-negative swabs to avoid overestimating our incidence and prevalence rates. In addition, some viruses were detected rarely, in particular influenza, a finding reflected in other community studies,17 but nevertheless limiting our ability to provide precise AFE estimates for these agents. We also excluded codetections in individual virus assessments as multiple aetiological agents make individual contributions of each agent difficult to ascertain, but analysed them separately to look at the association patterns of individual viruses. Symptom information, other than doctor-diagnosed otitis media and pneumonia, captured by daily diaries was not validated. To maximise accuracy, parents were trained to recognise symptoms before commencing the study. While healthcare worker-validated symptoms would be ideal, a study of this scale is logistically challenging without parent participation. This study design has been used previously18 and with others have shown that parents can be trained to recognise symptoms of interest,18 often as reliably as healthcare professionals.32 33 Our rates of ARI, including those associated with wheeze, are comparable with other community studies.34 35
Finally, as is common for these types of studies, families in our cohort were from more advantaged backgrounds and ARI episodes were predominantly of a mild-to-moderate nature.22 While many children in our study were first-born and from advantaged families, factors thought to decrease the rate of ARIs, secular changes in Australia have led to an increased proportion of children from these families attending childcare at an earlier age than other sectors of the population. A slightly higher proportion (80%–85%) of our cohort attended some form of care by the age of 15–24 months, compared with 74% of children in the Australian population, with childcare attendance an independent risk factor for ARIs.25 Moreover, the incidence of ARIs in the ORChID cohort22 is comparable to other reports in this age group34 36 37 and RSV and HRV-associated ARIs approximate other community-based studies conducted in more temperate climates of Australia (Perth) and Europe.38–40 Our findings for this cohort remain valid and provide important estimates on community respiratory virus exposures and ARIs in Australian children in a subtropical, urban setting.
Conclusions
Respiratory viruses, particularly HRV, were detected with remarkable frequency in healthy Australian children in the first 2 years of life, with at least one-third of new VDEs unaccompanied by symptoms. With molecular methods used increasingly to detect respiratory viruses in young children, our study provides insights into supporting attribution for virus-specific ARIs in this age group managed within the community. The established RNA respiratory viruses and AdV were more strongly associated with symptomatic than asymptomatic infections, while no such associations were found for the newly described DNA viruses, HPyVs and HBoV-1. These data emphasise the high community levels of HRV circulating among children. Importantly, they also provide evidence to suggest that the current clinical trials of candidate RSV and HMPV vaccines seeking to protect infants against severe disease and hospitalisation might also deliver substantial health benefits for all young children within the community.27
Acknowledgments
The authors acknowledge the generosity of the study families who participated in the study and the efforts of the recruitment nurses and volunteer staff for administrative assistance. The authors thank Professor Arto Palmu, National Institute for Health and Welfare, Helsinki, Finland, for critical review of the manuscript.
References
Footnotes
Contributors MS had full access to all of the data in the study and had the final responsibility for the decision to submit for publication.Study concept and design: KG, SBL, RSW, TPS, MDN, DW, DMW. Analysis and interpretation of data: MS, SBL, RSW, KG, TPS, AA, LM, SB. Drafting of the manuscript: MS, SBL, RSW, KG. Critical revision of the manuscript for important intellectual content: MS, RSW, TPS, DMW, AA, LM, SB, DW, MDN, SBL, KG. Statistical analysis: MS, RSW. Administrative and technical support: MS, RSW, SBL. Study supervision: SBL, RSW, KG.
Funding This study was supported by a National Health and Medical Research Council (NHMRC) (Australia) project grant (APP 615700) and a Children’s Hospital Foundation Queensland (CHFQ) (programme grant number: 50006). MS is the recipient of an NHMRC Dora Lush Clinical Scholarship and a CHFQ PhD Clinical Scholarship. SBL is the recipient of an NHMRC Early Career Fellowship and a CHFQ Mid-career Fellowship . DMW reports a Career Development Fellowship from the NHMRC. SB is the recipient of a CHFQ Early Career Fellowship.
Competing interests After completion of data collection for this study, MDN became a full-time employee of GlaxoSmithKline, GlaxoSmithKline Vaccines Value Health Science, 150 Beach Road, Gateway West #7, Singapore 189720, Singapore. Other authors have no competing interest to declare.
Ethics approval Children’s Health Queensland, Royal Brisbane and Women’s Hospital and The University of Queensland Human Research Ethics Committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published Online First. Figure 2 has been updated to include the missing figure legend.