Article Text

Abstract
Rationale Adiposity is associated with low lung function, but the longitudinal relationship between lung function and adiposity is inadequately studied.
Objective To examine the bidirectional longitudinal associations between rapid decline in lung function and adiposity phenotypes in healthy adults.
Methods This secondary analysis used a 25-year longitudinal dataset from the Coronary Artery Risk Development in Young Adults (CARDIA) study that enrolled 5115 participants.
Measurements In the first analysis, metabolic syndrome at or before CARDIA year (Y) 10 (Y10) was the predictor, and subsequent rapid decline in forced vital capacity (FVC) or forced expiratory volume in 1 s (FEV1) between Y10 and Y20 was the outcome. In the second analysis, rapid decline was the predictor, and incident metabolic syndrome at Y20 and/or Y25 was the outcome. In the third analysis, rapid decline was the predictor, and subsequent CT-assessed regional fat depots at Y25 were the outcome.
Results Metabolic syndrome at or before Y10 is temporally associated with rapid decline in FVC between Y10 and Y20 (adjusted p=0.04), but this association was explained by body mass index (BMI) at Y10. Rapid decline in FVC or FEV1 is temporally associated with greater incident metabolic syndrome at Y20 and/or Y25 (adjusted OR 2.10 (1.69, 2.61); p<0.001, and 1.56 (1.26, 1.94); p<0.001, respectively) and greater CT-assessed intrathoracic visceral adiposity at Y25 (adjusted standardised β 0.09; p<0.001 for both analyses). These associations were not explained by BMI levels prior to the outcome measurement.
Conclusions Healthy adults with rapid decline in lung function are at risk for developing metabolic syndrome and for disproportionate accumulation of intrathoracic visceral fat. Metabolic abnormalities may be an early extrapulmonary manifestation of lung impairment that may be preventable by improving lung health.
- Body mass index
- metabolic syndrome
- visceral fat
Statistics from Altmetric.com
Key messages
What is the key question?
Adiposity is associated with low lung function, but the longitudinal relationship between lung function and adiposity phenotypes is inadequately studied.
What is the bottom line?
Healthy adults with rapid decline in lung function are at risk for developing metabolic syndrome and for disproportionate accumulation of intrathoracic visceral fat.
Why read on?
Metabolic abnormalities may be an early extrapulmonary manifestation of lung impairment that may be preventable by improving lung health.
Introduction
Obesity and chronic lung diseases, affecting 79 million and 35 million Americans respectively, are currently contemporaneous epidemics in the USA and the world.1–3 Obesity constitutes a collection of heterogeneous phenotypes.4 This includes general adiposity (usually defined by body mass index or BMI), regional adiposity (usually defined by localised fat depots in the visceral, subcutaneous and intramuscular regions) and metabolically active adiposity (usually defined by the metabolic syndrome and its components). General adiposity and chronic lung diseases are both characterised by low lung function5–8 and systemic inflammation.9–14 Furthermore, regional and metabolically active adiposity measures such as abdominal adiposity and specifically intra-abdominal visceral adiposity are cross-sectionally associated with low values of forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1).15–17 An observational, cross-sectional, multicentre study found that more than 42% of hospitalised patients with chronic obstructive pulmonary disease (COPD) also had the metabolic syndrome.18 Many studies show that low spirometric values are associated with diabetes mellitus, a component of the metabolic syndrome.19–21 A nested case–control study of New York City firefighters concluded that abnormal plasma concentrations of triglycerides and high-density lipoprotein (HDL) cholesterol (also components of the metabolic syndrome) predicted low subsequent FEV1, independent of BMI.22 Thus, low lung function is associated with general, regional and metabolically active adiposity phenotypes. Longitudinal studies of the relationships between lung function and adiposity phenotypes are however limited, and the direction of this association is not well established.
The primary objective of our study was to examine the bidirectional longitudinal associations between rapid decline in lung function and metabolically active adiposity in healthy adults. Our secondary objective was to examine the association between rapid decline in lung function and regional adiposity, as defined by CT-assessed abdominal and thoracic fat depots. We hypothesised a priori that the metabolically active and regional adiposity phenotypes would be temporally associated with rapid decline and vice versa.
Methods
Study sample
This is a secondary data analysis, using a longitudinal dataset from the 25-year (1985–2011) Coronary Artery Risk Development in Young Adults (CARDIA) study that enrolled 5115 Caucasian and African-American subjects in four US cities. CARDIA was funded by the National Heart, Lung, and Blood Institute and designed to study cardiovascular disease risk factors in healthy adults. CARDIA recruited 5115 healthy individuals over the period 1985–1986 at four sites, including the University of Alabama at Birmingham (Birmingham, Alabama), the University of Minnesota (Minneapolis, Minnesota), Northwestern University (Chicago, Illinois) and Kaiser Permanente (Oakland, California). CARDIA-selected participants represented approximately an equal number of people in subgroups of age (18–24 and 25–30 years), race (52% black; 48% white), education level (high school or less and higher than high school) and sex (46% men; 54% women). Of the 5115 subjects initially enrolled, one subject withdrew consent, two subjects changed sex and 198 subjects did not attend follow-up exams after year 0 visit. These subjects were excluded from further analysis. Follow-up examinations were conducted at CARDIA years 2, 5, 7, 10, 15, 20 and 25 with a participant follow-up rate of 91%, 86%, 81%, 79%, 74%, 72% and 72%, respectively. At each examination visit, the study collected data including demographics, medical history, life style and habits, psychosocial history, physical examination parameters including blood pressure, weight, height, waist circumference and urine and blood samples. Medications were verified by study personnel. Written and signed informed consent was obtained from each participant. Institutional review board approval was obtained at each of the four participating study sites.
Study design
Our study involved analyses of three separate but related specific aims, as discussed below and shown in figure 1. For the longitudinal analysis for the aim 1, the metabolic syndrome, as defined by the Adult Treatment Panel (ATP) III of the National Cholesterol Education Program,23 at or before CARDIA year (Y) 10, was the predictor, and the rapid lung function decline between Y10 and Y20 was the outcome (analysis 1, figure 2). In order to study healthy adults, individuals with self-report of a provider diagnosis of lung disease (ie, ever-asthma, chronic bronchitis or emphysema) at any visit between Y0 and Y10 were excluded, thus reducing confounding. Also excluded were those with missing spirometry at Y10 and/or Y20. Rapid lung function decline was measured between Y10 and Y20, and subjects in the tertile with the greatest decline in lung function were compared with the rest, that is, subjects in the bottom two tertiles of decline. Rapid FEV1 and FVC decline was defined by cutpoints of 44.4 mL/year and 48.6 mL/year, respectively. The cutpoint for FEV1 is similar to that used in a recent large multinational study of lung function trajectories in COPD.24 Alternative analyses using decline as ternary variable (ie, three levels) and as continuous variable are presented in the online data supplementary 1.
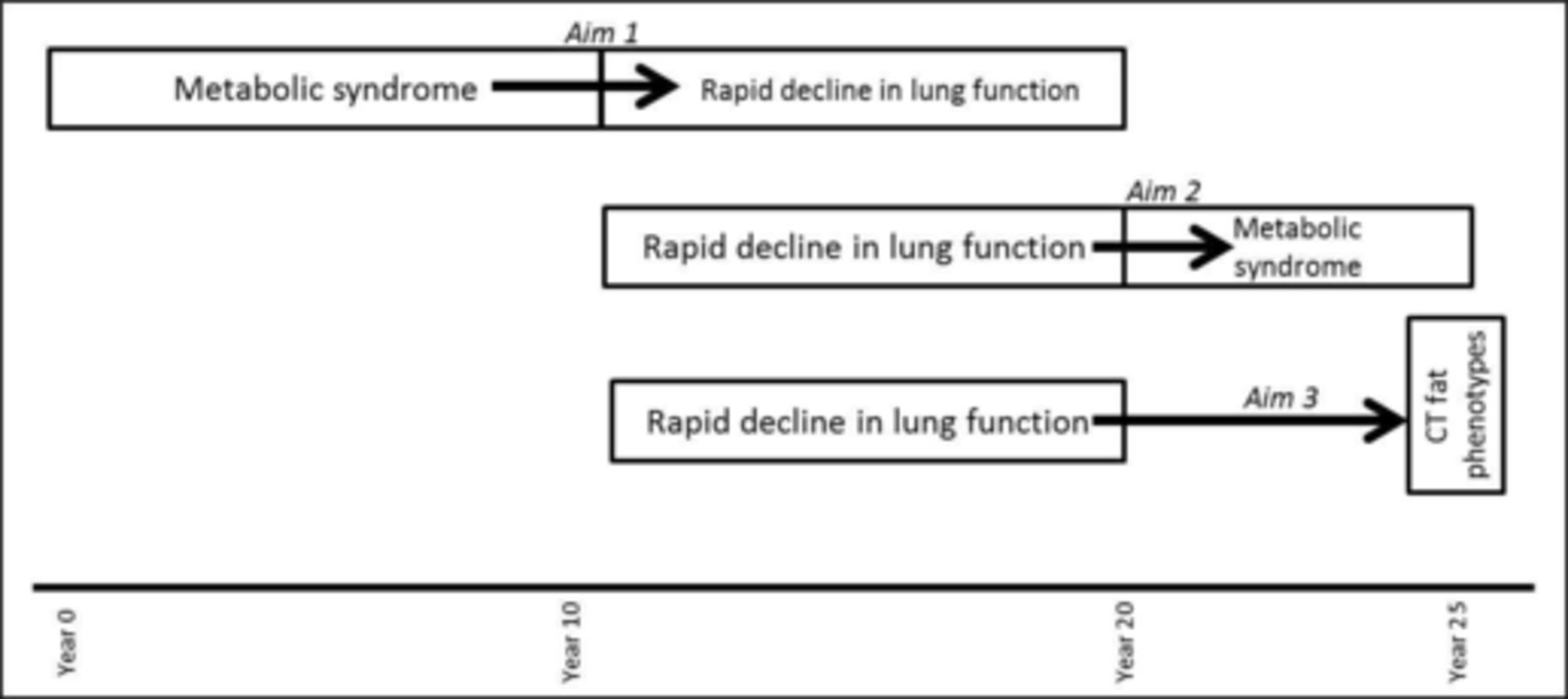
Overall plan for analyses.

Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) diagram for analyses 1 (aim 1) with metabolic syndrome as the predictor and rapid decline in lung function as the outcome.
For the longitudinal analysis for aim 2 that used rapid lung function decline between CARDIA Y10 and Y20 as the predictor and incident metabolic syndrome at Y20 and/or Y25 as the outcome (analyses 2, figure 3), exclusion criteria were similar to those for analyses 1. Also excluded were those with metabolic syndrome at any visit at or before Y10. Incident metabolic syndrome was measured at Y20 and/or Y25. Rapid FEV1 and FVC decline between Y10 and Y20 was defined by 44.2 mL/year and 48.1 mL/year, respectively, as described in analyses 1.24 Alternative analyses using decline as ternary variable and as continuous variable are presented in the online supplementary 1.

Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) diagram for analyses 2 (aim 2) with rapid decline in lung function as the predictor and metabolic syndrome as the outcome.
For the analysis of aim 3 using rapid lung function decline between CARDIA Y10 and Y20 as the predictor and CT scan-assessed regional fat depots at Y25 as the outcome (analyses 3, figure 4), exclusion criteria were similar to those for analyses 2. Also excluded were those with missing CT data at Y25. Rapid lung function decline between Y10 and Y20 was similarly defined as in analysis 2. Data from Y25 CT scan of the chest and abdomen were used to calculate regional adiposity, as described below.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) diagram for analyses 3 (aim 3) with rapid decline in lung function as the predictor and CT-assessed regional fat depots as the outcome.
Spirometry variables
Spirometry was performed at Y0, Y2, Y5, Y10 and Y20, using a protocol strictly adhering to the American Thoracic Society guidelines relevant at that time.25–27 Spirometry data were used from visits Y10 and Y20 for our study. Additional detail is provided in the online data supplementary 1.
Metabolic syndrome
This variable is defined by the ATP III in the presence of any three of the following five risk factors: (1) abdominal obesity with waist circumference more than 102 cm (>40 inches) in men and more than 88 cm (>35 inches) in women, (2) plasma concentrations of triglyceride ≥150 mg/dL or drug treatment for hypertriglyceridaemia, (3) plasma concentrations of HDL cholesterol of <40 mg/dL in men and <50 mg/dL in women or drug treatment for hypercholesterolaemia, (4) elevated blood pressure with systolic pressure of ≥130 mm Hg or diastolic pressure of ≥85 mm Hg or drug treatment for elevated blood pressure and (5) serum fasting glucose ≥110 mg/dL or drug treatment for diabetes mellitus.23
Waist circumference
Waist circumference was measured using a cloth anthropometric centimetre tape, applied horizontally at the level laterally midway between the iliac crest and the lowest lateral portion of the rib cage and anteriorly midway between the xiphoidal process of the sternum and the umbilicus. A second observer/recorder helped observe the position of the tape. After recording the measurement, the tape was removed, and a second measurement was made; both measurements were recorded to the nearest 0.5 cm, and mean of the two measurements was obtained.
Plasma concentrations of triglyceride and HDL cholesterol, and serum glucose
A fasting morning blood draw was performed by technicians with documented class time and experience in phlebotomy. Plasma samples for total triglyceride and HDL cholesterol were batched and sent monthly to Northwest Lipid Research Laboratory (Seattle, Washington); serum samples for fasting glucose level were similarly sent to the Central Laboratory at the American Bioscience Laboratory (Van Nuys, California). All samples was placed in freezer (−70°C) within 90 min of phlebotomy; quality control samples were also obtained and placed in separate boxes. HDL cholesterol was measured after plasma precipitation with dextran sulfate/magnesium chloride.
Blood pressure measurements
Three resting blood pressure measurements were taken over 15 min, after at least 5 min of rest. Caffeinated beverages were held for at least 30 min prior to blood pressure check. Measurements were taken by appropriately trained and supervised technicians. Mean values of the three systolic and diastolic blood pressure measurements were obtained.
Body weight and height
Weight was measured at every CARDIA visit using a calibrated scale, and the result was recorded to the nearest 0.2 pounds. Height was measured at each visit with the individual standing erect on the floor or hard platform with his/her feet flat on the ground and with straight back against mounted metal centimetre ruler and eyes looking straight ahead in Frankfort horizontal plane, and the result was recorded to the nearest 0.5 cm. BMI was calculated using height and weight measurements.
CT-assessed regional fat depots
Chest CT scan was performed from the posterior lung recess to the lung apex and including the upper part of the abdomen. Intrathoracic visceral adiposity was represented by measuring the pericardial adipose tissue by analysing data originating from the 45 mm of adipose tissue encasing the proximal coronary arteries. Abdominal adiposity was subcategorised in abdominal intramuscular, abdominal subcutaneous and intra-abdominal visceral adipose tissue compartments, with a protocol using volumetric acquisition and analysis centred at the L2–L3 and L4‐L5 vertebral levels. All CT-assessed continuous regional adiposity outcome measures were logarithmically transformed due to non-normal distribution. Non-alcoholic fatty liver disease was examined as a separate regional fat measure, categorically defined by CT-assessed liver attenuation of ≤40 Hounsfield units. Additional details are provided in the online data supplementary 1.
Statistical analysis
For univariate analyses, χ2 and Student’s t-tests were used for continuous and categorical outcomes, respectively. For univariate and multivariable analyses for categorical and continuous outcomes, logistic regression and linear regression tests were used, respectively.
Models and covariates: Standard covariates used in adjusted models included age, sex, race, socioeconomic status (represented by the total combined family income for the previous year), number of education years, current smoking status, pack-years of smoking, physical activity level (based on self-reported physical activity on a five-point scale) and the relevant spirometric parameter, all measured at CARDIA Y10. Exploratory analyses adding BMI at Y10 as a covariate to the fully adjusted model is presented in footnotes. BMI was not selected as a covariate a priori in the fully adjusted model since it is strongly associated with the metabolic syndrome and its components such as the waist circumference with which it bears a correlation of 0.9, and therefore its inclusion could lead to over adjustment in the main models.
For analyses 2, exploratory analyses adding BMI, hypertension and family history of diabetes mellitus at Y10 as covariates to the fully adjusted model are presented in footnotes.
For analyses 3, standard covariates were obtained at Y20 instead of Y10 used in above sets of analyses. Since the correlation between BMI and intrathoracic visceral adiposity is 0.52, BMI at Y20 was additionally included along with standard covariates in the adjusted model.
All analyses were conducted using SAS (Statistical Analysis Software V.9). p Values less than 0.05 were considered statistically significant.
Results
Analysis 1: metabolic syndrome is temporally associated with subsequent rapid decline in FVC, but this association is explained by prior BMI
Subjects with prevalent metabolic syndrome at or before CARDIA Y10 (mean age of 35 years) when compared with those without were heavier in weight and older; more likely to be black, men, report family history of diabetes mellitus; and have lower socioeconomic status, education and physical activity levels (table 1). Prevalent metabolic syndrome at Y10 predicted rapid decline in FVC (but not FEV1) over the subsequent 10 years (adjusted p=0.04, fully adjusted model, table 2). When Y10 BMI was additionally adjusted for, this longitudinal association was no longer significant, but BMI was a significant predictor of FVC decline (table 2, note 1).
Comparison of characteristics measured at CARDIA Y10 (mean age of 35 years) between groups with and without the metabolic syndrome at or before Y10
Metabolic syndrome at or before CARDIA Y10 (mean age 35 years) is temporally associated with rapid decline in FVC over subsequent 10 years
Analysis 2: rapid decline in lung function is temporally associated with incident metabolic syndrome
Subjects with rapid decline in FEV1 between CARDIA Y10 and Y20 visits (at mean ages of 35 and 45 years) when compared with those without were older; more likely to be men, ever-smokers, have hypertension, family history of diabetes mellitus, lower socioeconomic status and lower education; and have higher values of FEV1 and FVC at Y10 (table 3). Rapid decline in FEV1 predicted a greater incidence of the metabolic syndrome at CARDIA Y20 or Y25 (mean ages of 45 or 50 years; adjusted p value<0.001, table 4). These findings were similar between men and women. Similar results were seen when rapid decline in FVC was used as the predictor variable. These results were not explained by prior BMI since the Y10 BMI values were no different between those with and without rapid decline (table 3). Furthermore, adjustment for prior BMI did not change the results (table 4, note 1). Adjustment for Y25 regional adiposity measures did not change the results, except for intrathoracic visceral adiposity confounding the association between rapid decline in FEV1 and metabolic syndrome (table 4, note 2). Rapid decline in lung function also predicted subsequent individual incident components of the metabolic syndrome, with the strongest association with abdominal adiposity and hyperglycaemia (table E-VI, online data supplement).
Comparison of characteristics measured at CARDIA Y10 (mean age of 35 years) between the groups with and without rapid FEV1 decline (over subsequent 10 years)
Rapid decline in lung function between CARDIA Y10 and Y20 (mean ages of 35–45 years) is temporally associated with incident metabolic syndrome at Y20 or Y25 (mean age of 45 or 50 years)
Analysis 3: rapid decline in lung function is temporally associated with greater intrathoracic visceral adiposity later in life
Subjects with rapid decline in FEV1 between CARDIA Y10 and Y20 (mean ages of 35–45 years) when compared with those without had greater subsequent intrathoracic visceral adiposity at Y25 (mean age of 50 years), and this relationship was not explained by prior BMI (p<0.001, fully adjusted model, table 5). These findings were similar between men and women. Similar results were seen when rapid decline in FVC was used as the predictor variable.
Rapid decline in lung function between CARDIA Y10 and Y20 (mean ages of 35–45 years) is temporally associated with CT-assessed intrathoracic visceral adiposity at CARDIA Y25 (mean age 50 years)
Discussion
Rapid decline in lung function in healthy adults is temporally associated with incident metabolically active adiposity and greater subsequent intrathoracic visceral adiposity, and these associations are independent of prior BMI. While metabolically active adiposity also is temporally associated with subsequent rapid decline in FVC, this longitudinal association is explained by prior BMI.
Many studies demonstrate that gain in weight is associated with a reduction in lung function, and conversely weight loss is associated with an improvement in lung function.28–33 Our study uses the metabolic syndrome (a marker of metabolically active adiposity), instead of the commonly used BMI variable (a marker of general adiposity), to predict subsequent decline in FVC and demonstrates that the signal for this association primarily lies in the BMI value. The reason why general adiposity, rather than metabolically active adiposity, better predicts subsequent rapid decline in FVC in our longitudinal study is unclear. Other cross-sectional investigations have found the opposite: a large French population-based study by Leone et al demonstrated that abdominal adiposity, even with a normal BMI, is associated with lower FVC.34 Adiposity may reduce FVC due to mechanical or inflammatory causes. Mechanical causes include decreased respiratory compliance with consequently decreased lung volumes and increased gas trapping from premature small airway closure, particularly at the lung bases.6 35 36 In addition, adiposity is associated with both increased levels of proinflammatory adipokines (such as leptin, interleukin-6, and tumour necrosis factor-alpha) and decreased levels of anti-inflammatory adipokines (such as adiponectin).5 These adipokines in turn regulate systemic inflammation that is likely associated with impaired lung function.37–39 Either directly or indirectly via systemic inflammation, adipokines may also affect oedema and inflammation of small airways, resulting in their premature closure in obese subjects, in turn accentuating the mechanical effect on respiratory compliance.
Rapid decline in lung function and poor lung growth are both risk factors for COPD, the most common chronic lung disease.8 24 Many studies have shown that chronic lung disease is also associated with increased risk for the metabolic syndrome, including diabetes mellitus.40 41 Our longitudinal study using rapid decline in lung function as a subclinical marker for chronic lung disease demonstrates a similar association with incident metabolically active adiposity. The signal for this association does not lie in the BMI value, implying that this association is not simply explained by the mechanical restrictive effect of general adiposity. It is possible that low lung function results in chronic or intermittent hypoxia within the adipose tissue which in turn impacts their secretion of adipokines.42 These adipokines may in turn result in the development of the metabolic syndrome and diabetes mellitus. Hypoxia is however an unlikely explanation for the association seen in our population of primarily healthy adults with near-normal lung function. It is more likely that a systemic spillover of pulmonary inflammation, related to rapid decline in lung function, impacts the systemic secretion of adipokines by the adipose tissue and consequent metabolic dysfunction.43 44 This hypothesised mechanism may be supported by data from allergen inhalation of sensitised BALB/cJ mice that showed that lung inflammation impacted the response of adipose tissue, as assessed by reduced serum adiponectin and reduced fat expression of adiponectin mRNA45; this model may however be an imperfect analogy to our subjects since patients with asthma were excluded from our study. It is also possible that the impact of rapid decline in lung function may extend beyond influencing the inflammatory function of fat but may also include a disproportionate expansion of metabolically active intrathoracic visceral fat depot (as shown in table 4, note 2 and table 5).
Recent studies suggest that ectopic fat present within cells of non-adipose tissue (such as viscera) may be more metabolically active and more relevant for metabolic dysfunction than physiological fat present within cells of adipose tissue.46 47 Most literature on ectopic fat focuses on intra-abdominal visceral adiposity, and the physiological significance of intrathoracic visceral adiposity is not well understood. Animal studies suggest that intrathoracic visceral adipose tissue has a greater capacity for fatty acid release than adipose tissue elsewhere in the body.48 Our study demonstrates that after adjustment for general adiposity, rapid decline in lung function is associated with greater subsequent intrathoracic visceral adiposity. It is possible that the lung may have paracrine signalling to induce changes in nearby fat depots.
The strengths of our study relate to our use of a well-characterised national cohort with an adequate sample size and African-American minority enrolment, study of an innovative hypothesis, longitudinal study design, high-quality spirometry tests, strict quality control for laboratory tests and CT-assessed regional fat depots. In addition, the reasonably low loss-to-follow-up rate of 28% over the 25-year follow-up period would suggest that selection bias is an unlikely explanation for our results. Our study has several limitations. Our CT assessment of intrathoracic visceral adiposity does not allow one to differentiate physiologically beneficial brown fat from proinflammatory white fat. Brown fat is typically present in the upper chest and neck, rather than around the pericardium. It is therefore reasonable to presume that our intrathoracic visceral fat depots are representative of white fat. While we have measurements of lung function and metabolically active adiposity at more than one time point, we studied only one time point measurement of CT-assessed fat, which limits our ability to study a longitudinal change in that variable. Fat within and around the lung includes peribronchial, pleural and mediastinal fat and is technically more difficult to measure than pericardial fat, the site of the greatest fat accumulation within the thorax.49 Our assumption that pericardial fat may reflect fat around the lung is supported by the findings of a small study that demonstrated a correlation as high as 0.68 between pericardial fat and fat at the interior margin of the chest wall anteriorly.49 One possible explanation for rapid decline predicting subsequent intrathoracic visceral adiposity is that individuals with rapid decline gain more weight than those without rapid decline. We did not find that to be the case (see table E-VII, online data supplement). Thus, this association was not simply explained by an increase in general adiposity. We are also unable to examine longitudinal change in dietary components as possible confounders in this study. We used the ATP III guidelines and not the International Diabetes Federation guidelines to define the metabolic syndrome in our study population of Caucasian and African-Americans. This approach is reasonable since the concordance between the two definitions is about 90% in the USA, where ATP III values continue to be used.50 Finally, causality is not supported by the findings of this study, but temporal association is established. This temporal association may however be due to coassociation with a third factor or process.
Our longitudinal findings add to the growing evidence for signalling between lung and adipose tissue, whereby diseases that affect one organ may impact the other. Healthy adults with rapid decline in lung function are at risk for developing subsequent metabolically active adiposity and for disproportionate accumulation of fat in metabolically active regional fat depots, independent of general adiposity. Metabolic abnormalities may be an early extrapulmonary manifestation of lung impairment that may be preventable by improving lung health.
References
Footnotes
Contributors AS, MM, BT, RK, LJS and DRJ made substantial contributions to the conception or design of the work, and CQ, JJC and AA made substantial contributions to the acquisition, analysis or interpretation of data for the work. AS, MM, BT, RK, LJS, DRJ, CQ, JJC and AA made substantial contribution towards drafting the work or revising it critically for important intellectual content. AS, MM, BT, RK, LJS, DRJ, CQ, JJC and AA provided the final approval of the version to be published. AS, MM, BT, RK, LJS, DRJ, CQ, JJC and AA agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The Coronary Artery Risk Development in Young Adults Study (CARDIA) is conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with the University of Alabama at Birmingham (HHSN268201300025C & HHSN268201300026C), Northwestern University (HHSN268201300027C and R01 HL122477), University of Minnesota (HHSN268201300028C), Kaiser Foundation Research Institute (HHSN268201300029C), and Johns Hopkins University School of Medicine (HHSN268200900041C). CARDIA is also partially supported by the Intramural Research Program of the National Institute on Aging (NIA) and an intra,agency agreement between NIA and NHLBI (AG0005). This manuscript has been reviewed by CARDIA for scientific content.
Competing interests None declared.
Ethics approval CARDIA study was approved by each of the four participating institutions.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data are available on request from the CARDIA Study Publications and Presentations Committee.