Article Text

Abstract
Background Suboptimal adherence to CPAP limits its clinical effectiveness in patients with obstructive sleep apnoea (OSA). Although rigorous behavioural interventions improve CPAP adherence, their labour-intensive nature has limited widespread implementation. Moreover, these interventions have not been tested in patients at risk of poor CPAP adherence. Our objective was to determine whether an educational video will improve CPAP adherence in patients at risk of poor CPAP adherence.
Methods Patients referred by clinicians without sleep medicine expertise to an urban sleep laboratory that serves predominantly minority population were randomised to view an educational video about OSA and CPAP therapy before the polysomnogram, or to usual care. The primary outcome was CPAP adherence during the first 30 days of therapy. Secondary outcomes were show rates to sleep clinic (attended appointment) and 30-day CPAP adherence after the sleep clinic visit date.
Results A total of 212 patients met the eligibility criteria and were randomised to video education (n=99) or to usual care (n=113). There were no differences in CPAP adherence at 30 days (3.3, 95% CI 2.8 to 3.8 hours/day video education; vs 3.5, 95% CI 3.1 to 4.0 hours/day usual care; p=0.44) or during the 30 days after sleep clinic visit. Sleep clinic show rate was 54% in the video education group and 59% in the usual care group (p=0.41). CPAP adherence, however, significantly worsened in patients who did not show up to the sleep clinic.
Conclusions In patients at risk for poor CPAP adherence, an educational video did not improve CPAP adherence or show rates to sleep clinic compared with usual care.
Trial registration number ClinicalTrials.gov Identifier: NCT02553694.
- compliance
- auto-PAP
- sleep apnea
- clinic show rate
Statistics from Altmetric.com
Key messages
What is the key question?
Can viewing an educational video in the sleep laboratory before an in-laboratory polysomnogram improve CPAP adherence in patients at risk of poor CPAP adherence?
What is the bottom line?
Viewing an educational video prior to the sleep study does not lead to improved outcomes.
Why read on?
Improving CPAP adherence is a clinically relevant outcome given that there is a dose–response relationship between CPAP adherence and various neurocognitive and cardiometabolic outcomes.
Introduction
Obstructive sleep apnoea (OSA) is an increasingly prevalent chronic disorder associated with significant morbidity and mortality.1 CPAP remains the most efficacious treatment and continues to be considered the gold standard for treating patients with moderate to severe OSA. However, suboptimal adherence to CPAP therapy limits its clinical effectiveness.2 Indeed, if CPAP adherence is defined as greater than 4 hours of nightly use, 46%–83% of patients with OSA have been reported to be non-adherent.3 Given that there is a dose–response relationship between CPAP adherence and various neurocognitive and cardiometabolic outcomes,4–6 there is a need for identifying ways to improve CPAP adherence.7 Several relatively labour-intensive interventions have been proven to improve CPAP adherence. These interventions include enhanced education and frequent phone calls,8–10 cognitive behavioural therapy11 and motivational enhancement.12–15 There is a need for simpler, low-cost interventions that can improve CPAP adherence. Early interventions are critical since patients establish CPAP usage patterns very early in the course of therapy.16–18 Unfortunately, attempts to enhance CPAP adherence using less time-consuming and labour-intensive interventions via telemedicine have led to mixed results.19–21 A short video aimed at enhancing CPAP therapy is an attractive educational tool given that patients can view it without significant staff effort while waiting in the sleep laboratory or in the clinic. This educational method has been evaluated in two small randomised controlled trials.22 23 In one study, although rates of return to sleep clinic improved with the video education, objective CPAP adherence was not available in the majority of patients.22 In the second study, there was a trend towards improved CPAP adherence in the video education group.23
While several sociodemographic factors have been associated with poor CPAP adherence, randomised controlled trials have not focused on enriching their cohorts with such patients. Socioeconomic status,24 25 race and ethnicity26–30 and not being seen by a clinician with sleep medicine expertise28 31 32 are among a few factors associated with CPAP adherence. In this context, we designed a randomised controlled trial to test the hypothesis that, compared with usual care, an educational video about OSA and CPAP viewed in the sleep laboratory before a split-night polysomnogram (PSG) improves CPAP adherence. Our goal was to enrol patients who we have previously reported to be at higher risk of poor CPAP adherence. These patients include those referred for PSG by clinicians without sleep medicine expertise in an urban inner-city tertiary-care medical centre that serves a predominantly minority population.28
Methods
Participants
The primary aim of the Sleep Apnea Video Education for CPAP (SAVE-CPAP) study was to assess the impact of an educational video on CPAP adherence in a patient population at increased risk of low CPAP adherence. We performed a parallel-arm, investigator-blinded, randomised controlled trial comparing enhanced education using an educational video with usual care. The study was registered at ClinicalTrials.gov (NCT02553694) and was approved by the University of Chicago’s Institutional Review Board (IRB14-0198). All patients provided written informed consent.
Between August 2014 and April 2016, all adult patients referred to the University of Chicago Sleep Disorders Center for an in-laboratory split-night PSG for suspicion of OSA were screened for eligibility. Eligible patients had to be >18 years of age, referred for a split-night PSG by a clinician without board certification in sleep medicine (ie, at higher risk of CPAP non-adherence),28 31 32 diagnosed with OSA and successfully titrated with CPAP during the split-night PSG. Patients were excluded if they had prior CPAP use, had undergone a prior PSG, had prior consultation with a sleep medicine clinician or were unable to be set up with home CPAP therapy within 14 days of the split-night PSG. Additional exclusion criteria were dementia, non-English-speaking, illiterate, legally blind, not being diagnosed with OSA or not requiring CPAP titration during the split-night PSG, and requiring bilevel positive airway pressure (PAP) titration or oxygen supplementation.
Randomisation
Random number generator with block size of four was used to generate a weekly order of intervention to be used by the sleep technologists in the sleep laboratory. The weekly allocation was concealed from the investigators. On a weekly basis, patients were randomly assigned to enhanced education, which included viewing a 4 min educational video about OSA and CPAP therapy developed by our team, or to usual care which included receiving an informational pamphlet on OSA and CPAP therapy developed by the American Academy of Sleep Medicine (AASM).
Procedures
Prestudy
Patients’ baseline characteristics were collected on the night of the split-night PSG. Patients completed questionnaires regarding their demographic information, the Epworth Sleepiness Scale (ESS),33 Center for Epidemiologic Studies Depression (CES-D)34 and the Pittsburgh Sleep Quality Index (PSQI).35 Comorbidities were confirmed by reviewing the electronic medical record (Epic, Verona, Wisconsin, USA).
Enhanced education using a video
The educational video script included information aimed at increasing knowledge about the consequences of untreated severe OSA and the importance of CPAP adherence. Following randomisation and before the initiation of the PSG, the sleep technologist in charge of performing the split-night PSG informed the patient about group allocation and played the video which was viewed by the patient. The sleep technologist did not provide any additional guidance to the patients during the video. Moreover, the investigators did not have any contact with the patients during the overnight in-laboratory PSG. The video lasted 4 min and was titled ‘Understanding your sleep study and sleep apnea’. In this video, an African–American female patient-actor has a discussion with a white male sleep technologist in the sleep laboratory regarding the process of undergoing PSG, the consequences of untreated severe OSA and the importance of CPAP therapy. Additionally, voice-over and text slides describe the process of PSG in more detail, emphasising the importance of CPAP therapy. A copy of the video is available as an online supplementary video.
Usual care
Pamphlets on OSA and CPAP therapy purchased from the AASM were provided to the patients randomised to usual care on arrival to the sleep laboratory prior to initiating the PSG (http://www.aasmnet.org/resources/pdf/products/snoringandsleepapnea_web.pdf). The educational pamphlets were handed out to the patients by the sleep technologist in charge of performing the split-night PSG. The investigators did not have any contact with the patients during the overnight in-laboratory PSG.
Polysomnography
Following educational intervention and questionnaire completion, the patients underwent a split-night PSG as per routine clinical care. Details of PSG procedures are provided in the online Supplementary material.
Poststudy
The morning following the split-night PSG, the patients were given a morning questionnaire to complete, which assessed perception of CPAP therapy. This questionnaire has not been validated, and it was developed by the investigators for the purpose of the SAVE-CPAP clinical trial.
Home CPAP therapy
All split-night PSGs were reviewed by board-certified sleep specialists the next business day. Enrolled patients received auto-PAP (APAP) devices within 2 weeks from the date of the split-night PSG. Two types of APAP units were used, and there was no significant difference in the distribution of the devices between the two intervention groups (p=0.56). AirSense S10 AutoSet (ResMed) was used in 64% of the patients in the video education group and 68% in the usual care group. System One REMStar 60 Series Auto (Philips Respironics) was used in 36% of the patients in the video education group and 32% in the usual care group. The minimum pressure was set at 2–3 cm H2O below the optimal pressure and the maximum pressure was set at 2–3 cm H2O above the optimal pressure. APAP devices for home therapy were delivered to the patients by trained respiratory therapists who spent 30–40 min with each patient going over the process of using APAP.
Phone calls
As part of a priori planned exploratory analysis, both groups were further randomised to receive a phone call the next business day following the split-night PSG from either the sleep physician who interpreted the split-night PSG or from a non-physician sleep laboratory staff member. The sleep medicine physicians briefly discussed the results of the sleep study and the importance of CPAP therapy, and reminded the patients of their scheduled sleep clinic appointment. The sleep physician recorded the time spent on the phone with the patients. The non-physician staff phone calls only reminded patients of their scheduled sleep clinic appointment without discussing any details of the PSG or CPAP therapy.
CPAP adherence monitoring
The patients were set up with home CPAP therapy using APAP devices by durable medical equipment providers within 2 weeks of the split-night PSG. All APAP devices were equipped with modems transmitting nightly adherence data to a secure server, thereby allowing remote monitoring without clinic attendance. CPAP adherence data were obtained from the secure server after the first 30 days of therapy by trained research assistants. CPAP adherence was also monitored remotely for an additional 30 days after the sleep clinic consultation date, regardless of whether the patient attended the sleep clinic appointment. The investigators were unblinded when patients were scheduled for their sleep clinic consultation visit, regardless of whether they attended the clinic appointment or not.
Sleep clinic attendance rate
The patients were scheduled to be seen in the sleep clinic 6–8 weeks after initiating home CPAP therapy. Outpatient sleep clinic consultation attendance rate following the split-night PSG was obtained through the electronic medical record approximately 2 months after the scheduled appointment date.
Power analysis
A priori sample size calculation was performed based on available data.11 19 28 Randomised controlled trials have reported an increase in CPAP adherence of 2–3 hours/night with various behavioural interventions.11 19 We estimated the sample size required to detect 1 hour/night higher level of CPAP adherence during the first 30 days of therapy with video education compared with usual care. Assuming an SD of 2.5 hours based on our prior observational data28 and power of 80%, with a two-sided significance level of 0.05, the estimated total sample size was 208. Importantly, this trial was not powered for equivalence or non-inferiority.
Statistical approach
Our prespecified primary outcome was unadjusted CPAP adherence during the first 30 days of therapy measured in hours/night. Our secondary outcomes were sleep clinic show rate and CPAP adherence during the 30 days after the scheduled sleep clinic appointment (regardless of whether the patient showed up to the appointment or not). There were no missing values for these outcomes. All analyses were performed based on intention-to-treat. Results were considered statistically significant if the two-sided p value was <0.05. Continuous variables are reported as mean (95% CI) and were compared using independent t-test for normally distributed data and non-parametric Mann-Whitney U test for non-normally distributed data after confirming distribution of data using the Shapiro-Wilk test of normality. Categorical variables were compared using X2 test. As an exploratory analysis, we also compared the impact of a phone call made by either a sleep physician or a non-physician member of the sleep laboratory on CPAP adherence and clinic show rate. All statistical analyses were performed using IBM SPSS Statistics V.22.
Results
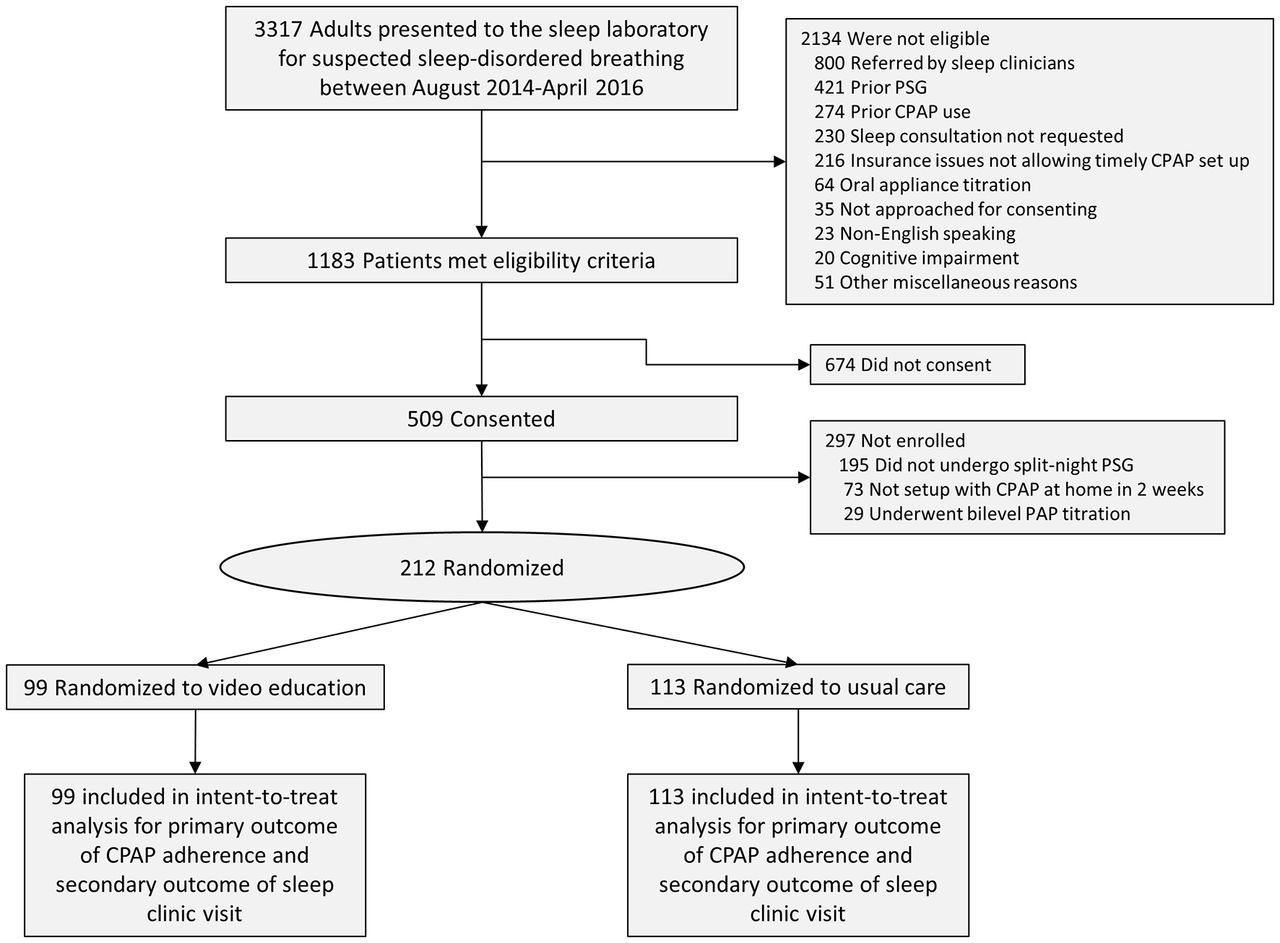
A total of 3317 adult patients were referred to the sleep laboratory between August 2014 and April 2016 for suspicion of OSA. Of these, 1183 met our eligibility criteria and 509 consented to participate in the study. However, 297 were not enrolled because they did not undergo CPAP titration during the PSG due to not having OSA or having mild OSA. Other reasons for not enrolling were inability to set up with home CPAP therapy in a timely fashion or requiring bilevel PAP titration. Therefore, 212 patients were randomised: 99 to video education and 113 to usual care (see figure 1).

Participant flow in the Sleep Apnea Video Education for CPAP trial. PAP, positive airway pressure; PSG, polysomnogram.
The group randomised to video education was slightly older than the usual care group. More than half of the patients were women, 60% were non-Hispanic black and 6% were Hispanic. OSA-related symptoms were similar between the two groups. Other sociodemographic data are summarised in table 1. The prevalence of comorbidities obtained from electronic medical records is summarised in table 2. Diabetes and coronary heart disease were more prevalent in the video education group. Baseline PSG data are presented in table 3. In general, the cohort had moderate to severe OSA. The Apnoea–Hypopnoea Index (AHI) and Oxygen Desaturation Index scores were higher in the video education group. The minimum and maximum pressure settings on the home APAP devices between the two groups were similar. Additional PSG variables are summarised in table 3.
Baseline descriptive characteristics in video education and usual care groups
Comorbidities in the video education and usual care group
Polysomnographic data in the video education and the usual care group
Primary outcome measure
There was no significant difference in CPAP adherence, defined as mean nightly CPAP use at the prescribed pressures during the first 30 days of therapy, between the video education group (3.3, 95% CI 2.8 to 3.8 hours/day) and the usual care group (3.5, 95% CI 3.1 to 4.0 hours/day; p=0.44). Although the usual care group used CPAP on more days than the video education group (21.5, 95% CI 19.8 to 23.2 days vs 18.7, 95% CI 16.6 to 20.9 days; p=0.045), the per cent of days used above 4 hours per night did not differ between the two groups (p=0.58). APAP units effectively treated OSA as demonstrated by the low residual AHI and low mask leak (table 4). In a post-hoc analysis of covariance, there was no significant difference in CPAP adherence between the two groups after adjusting for age, source of referral and baseline AHI.
Primary and secondary outcomes
Secondary analyses
There was no significant group difference in the sleep clinic attendance rate (54% video education vs 59% usual care group; p=0.41). We monitored CPAP adherence during the 30 days after the sleep clinic appointment date. For patients who did not show up to the sleep clinic appointment, we used the date of the clinic appointment as the start date for the 30 days after sleep clinic visit. There was no significant difference in mean nightly CPAP use between the two groups. The video education group used CPAP for 2.9 hours/night (95% CI 2.4 to 3.5 hours/night) vs 3.4 hours/night (95% CI 2.9 to 3.9 hours/night) in the usual care group (p=0.71).
Exploratory analyses
In the video education group, 51 patients were randomised to receive a phone call from a sleep physician and 48 were randomised to receive a phone call from a staff member. In the usual care group, 62 were randomised to receive a phone call from the sleep physician and 51 were randomised to receive a phone call from a staff member. There was no group difference in the time the sleep physicians spent on the phone talking to the patient (video education 4.8 min, 95% CI 4.1 to 5.6 min; vs usual care 4.8 min, 95% CI 4.0 to 5.5 min; p=0.9). As summarised in online supplementary table 1, there was no significant difference in CPAP adherence or sleep clinic attendance rate among the four groups. There was also no significant group difference in patients’ perception on various questions related to whether they plan to use CPAP and whether they plan to show up to the sleep clinic appointment (see online supplementary table 2).
In a non-randomised and unadjusted univariate post-hoc analysis, we explored whether there was an improvement in CPAP adherence in the 30 days after the consultation in those who showed up for the sleep clinic appointment. Of the 212 patients, 120 (57%) showed up to the sleep clinic appointment. In these patients, CPAP adherence between the first 30 days of therapy and the 30 days after the sleep clinic appointment did not change (3.9, 95% CI 3.4 to 4.3 hours/night vs 3.9, 95% CI 3.4 to 4.3 hours/night; p=0.9). These patients also reported symptomatic improvement. The ESS decreased by an average of 2 points (95% CI 1.3 to 2.7; p<0.001) and the CES-D score decreased by an average of 3.4 points (95% CI 2.2 to 4.6; p<0.001). In contrast, in the 92 patients (43%) who did not show up to the sleep clinic appointment, CPAP adherence worsened in the 30 days after the scheduled appointment date compared with the first 30 days of therapy (3.0 hours/night, 95% CI 2.5 to 3.5 vs 2.2 hours/night, 95% CI 1.7 to 2.8 hours/night; p=0.001).
We also examined the association between CPAP adherence, educational level and race in our cohort (see figure 2). In patients who reported attending less than 4 years of college, there was no significant difference in CPAP adherence between blacks and non-blacks. In contrast, in patients who reported attending four or more years of college, CPAP adherence was significantly lower in blacks. To further explore factors associated with CPAP adherence at 30 days, we performed a post-hoc linear regression model that included the entire cohort (n=212). Variables introduced in the model were selected based on prior studies and biological plausibility and included age, sex, race (black or not), years attended college (≥4 years or more of college vs <4 years of college), body mass index, ESS score, CES-D score, habitual sleep duration derived from the PSQI questionnaire, complaints of difficulty initiating or maintaining sleep, AHI, mask type, mask leak (high leak or not), and the response to the following question obtained on the morning after the split-night PSG: ‘I plan to use CPAP almost every night’. The response to this question was categorised as ‘strongly agree or agree’ or ‘disagree or strongly disagree’. The only variables independently associated with CPAP adherence were years attended college and the response to the question regarding the likelihood of using CPAP. Compared with less than 4 years of college, those who attended college for four or more years had an adjusted increase in CPAP adherence of 1.0 hour/night (95% CI 0.3 to 1.7 hour/night; p=0.006). After adjusting for other confounders, those who disagreed or strongly disagreed with the statement ‘I plan to use CPAP almost every night’ used CPAP 1.4 hours less per night (95% CI 0.03 to 1.9 hours/night; p=0.044). Race was not significantly associated with CPAP adherence after adjusting for other confounders (p=0.35). Moreover, race–education interaction term was not significant (p=0.66 for interaction).

{kind=link}
{kind=link}
Unadjusted 30-day CPAP adherence based on years attended college and race. Values reported as mean (95% CIs).
Discussion
To the best of our knowledge, this study is the first randomised controlled trial to assess the impact of an educational video on CPAP adherence in a population of patients at increased risk for poor CPAP adherence. We demonstrated that compared with usual care, a brief video education prior to the sleep study does not lead to improved outcomes. Furthermore, a phone conversation after the sleep study between the patient and the sleep physician had no impact on any of the outcomes. Our study shows that a simple intervention such as our short educational video is not sufficient to improve a complex behaviour such as CPAP adherence, particularly in a patient population at increased risk for CPAP non-adherence. Indeed, randomised controlled trials that have demonstrated significant improvement in CPAP adherence have involved more complex and more intensive behavioural interventions than ours, such as rigorous education plus frequent phone calls,8–10 cognitive behavioural therapy11 and motivational enhancement.12–15 Despite their proven efficacy, these behavioural interventions have not seen widespread implementation in clinical practice. We posit that the lack of implementation of these behavioural interventions is likely related to the limited resources faced by most clinical practices. Moreover, it remains unclear whether these behavioural interventions are effective if implemented in patients at high risk for poor CPAP adherence.
Although we and others have previously reported that CPAP adherence is significantly lower in blacks,26–28 in the present study race was not independently associated with CPAP adherence after adjusting for other important covariates, such as self-reported years of attending college. In a small subgroup analysis, we could only identify two variables that were significantly associated with poor CPAP adherence: attending less than 4 years of college and the response to a simple question regarding the likelihood of using CPAP. Bakker et al 29 also found that low CPAP adherence was associated with educational level and socioeconomic status, not race and ethnicity. Similar to our finding, prior studies have reported that patients’ experience with and benefit perceived from CPAP therapy after just the first night of CPAP titration are important factors in determining long-term adherence.36 37 Notably, Lewis et al 36 demonstrated that in a small cohort of predominantly white men, a single question on the morning following CPAP titration predicts adherence to CPAP. Our study confirms the findings of Lewis et al in a larger and more diverse cohort in which more than half were women and two-thirds were minorities. Early interventions aimed at improving CPAP adherence are critical since patients establish CPAP usage patterns very early in the course of therapy.16–18 Therefore, simple questionnaires designed to identify patients at increased risk of poor CPAP adherence can be clinically useful. In the context of personalised medicine, early recognition of patients at risk of CPAP non-adherence may lead to a more strategic application of rigorous behavioural interventions in this specific patient population, thereby reducing workload and staff burden.
Two prior studies using video education reported positive outcomes. However, in one study objective CPAP adherence was not available in a large proportion of patients.22 In another small study, there was a trend towards improved CPAP adherence in the video education group.23 Despite our larger sample size and availability of CPAP adherence data in all enrolled patients, we were not able to demonstrate any improvement in outcomes with an educational video. This may in part be related to the fact that we were focusing on patients at high risk for CPAP non-adherence.
Our sleep laboratory allows referral of patients for in-laboratory PSG and initiation of home CPAP therapy without a prior sleep medicine consultation.19 28 Importantly, not being seen by a clinician with sleep medicine expertise has been associated with poor CPAP adherence in several observational studies.28 31 32 In contrast, two Australian multicentre randomised controlled trials demonstrated similar levels of CPAP adherence when patients were managed by sleep specialists or by primary care providers38 or nurses,39 although in these trials primary care providers and nurses either underwent significant training on OSA and CPAP management or had extensive clinical experience.38 We believe our study may be more reflective of real-world practice where clinicians without sleep medicine expertise routinely refer patients to the sleep laboratory without having undergone prior training regarding OSA diagnosis and management as in the two Australian clinical trials.38 39
Our study has several limitations. Our trial was not powered for equivalence or non-inferiority. As such, a type II error is possible and we therefore cannot claim that the interventions are equal. Specifically, we cannot exclude the possibility that some of our patients allocated to usual care accessed online educational materials outside of the context of the clinical trial. Additonally, our study was not appropriately powered for the exploratory outcomes. Although only 43% of eligible patients consented to participate in the trial, baseline characteristics were similar between groups. Moreover, The primary outcome remained insignificant even after adjusting for baseline AHI, age and source of referral. The open-label nature of our study may have increased the risk of bias. We chose objective outcomes such as CPAP adherence and sleep clinic attendance rates in order to minimise bias. Although our randomisation schema consisted of weekly as opposed to individual allocation to the two groups, the sleep physicians were blinded to the weekly assignment. Our cohort consisted of predominantly minority population treated in an inner-city tertiary-care medical centre and therefore our findings may not be generalisable. But it is precisely this group of patients that is at increased risk of CPAP non-adherence. We did not standardise the content of the phone discussion between the sleep physicians and the patients. It is certainly possible that the effectiveness of the brief phone conversation may have been impacted by the communication skills of the physician. However, our goal was to design a pragmatic clinical trial that is reflective of routine clinical practice. Although our primary outcome of CPAP adherence at 30 days is relatively short compared with other studies, our secondary outcome was CPAP adherence during the 30 days after the sleep clinic appointment date. Importantly, early patterns of CPAP use have been shown to correlate strongly with long-term CPAP adherence.16–18 Of note, the sleep clinic appointment date was approximately 6–8 weeks after initiating CPAP therapy. Therefore, CPAP adherence during the 30 days after the sleep clinic appointment date reflects CPAP adherence during the third month of therapy. Importantly, we remotely monitored CPAP adherence using modem technology embedded in the CPAP units and thus had no missing data, which strengthens our findings. Lastly, our intervention took place in the context of a clinical visit in the sleep laboratory, not at home. Future studies promoting CPAP adherence should explore multidimensional educational and motivational interventions that take place in the sleep laboratory combined with home-based interventions leveraging digital technology.
In summary, our study demonstrates that in a population of patients at increased risk for poor CPAP adherence, a brief educational video does not improve CPAP adherence or sleep clinic attendance rate. Our trial emphasises the need for additional randomised controlled trials designed to test previously reported effective behavioural interventions in at-risk patient populations. Ultimately, improving CPAP adherence is a clinically relevant outcome given that there is a dose–response relationship between CPAP adherence and various neurocognitive and cardiometabolic outcomes.
Acknowledgments
The authors wish to thank the sleep technologists at the University of Chicago Sleep Disorders Center. The authors are also grateful to Mark Saathoff, Lisa Spampinato and Deborah X Guzman-Buchness for providing their expertise in developing the educational video. They also would like to thank Pritzker School of Medicine Experience in Research (PSOMER) visiting students Maria Espinosa and Ana Lucia Fuentes for their early collaboration on this project.
References
Footnotes
ASG and JSB contributed equally.
Contributors JSB, BM, ASG and VMA designed the study. SS, KA, LE and MM collected data. BM, ASG, JSB, VMA and JMF participated in data management, analyses, interpretation and manuscript preparation. BM oversaw all analyses and takes full responsibility for the work as a whole, including the study design, access to data, and the decision to submit and publish the manuscript. All authors approved this manuscript in its final form.
Competing interests ASG, JSB, SS, KA, LE, MM and JMF have no conflicts of interest to declare. VMA, JMF and BM receive support from the National Institutes of Health Grant R25HL116372-03. BM is supported in part by the National Institutes of Health Grant R01HL119161. He has also received honorarium from Zephyr Medical Technologies and has served on the advisory board of Itamar Medical. None of the competing interests are related to the content of the submitted research.
Ethics approval University of Chicago’s Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.