Article Text

Statistics from Altmetric.com
Introduction
Acquired central hypoventilation syndrome (CHS) is a rare cause of respiratory failure. We report a case of acquired CHS, diagnosed several years after Listeria monocytogenes (LM) rhombencephalitis.
Case report
In 1993, a 46-year-old woman presented to our Sleep Clinic with poor sleep, nocturnal choking episodes and daytime fatigue. She denied habitual snoring and hypersomnolence. Her medical history was unremarkable except for severe LM rhombencephalitis in 1977. At that time, the patient had been hospitalised in the intensive care unit following the acute onset of fever, influenza-like symptoms, meningism, facial palsy and nystagmus. Blood and cerebral spinal fluid samples were positive for LM on direct microscopic exam as well cultures. Treatment was initiated but the patient acutely deteriorated, exhibiting tetra paresis, bilateral pontomedullary syndrome, impairment of vigilance, and experienced a cardiac arrest. She was successfully resuscitated and remained in the intensive care unit with gradual and slow recovery. After a lengthy hospital stay, she was eventually discharged from the hospital and resumed a normal life, with few neurological sequelae such as dysphagia and mild facial palsy. To investigate the patient's sleep complaints, an in-laboratory full polysomnography was obtained and revealed central sleep apnoeas and hypopnoeas (Apnoea–Hypopnoea index (AHI)=50 events/hour) with severe nocturnal hypoxaemia. Morning arterial blood gases revealed alveolar hypoventilation with partial pressure of arterial CO2 or PaCO2 of 6.7 kPa and PaO2 of 9.5 kPa. The patient refused further investigations and therapy but agreed to return to clinic for a follow-up in 1 year. In 1994, polysomnography and arterial blood gases showed persistent sleep apnoea and daytime hypoventilation but the patient continued to decline treatment. The patient was then lost to follow-up until 2011, when she presented for the third time to the Sleep Clinic complaining of daytime fatigue, unrefreshing sleep, choking episode during sleep and daily morning headaches, with a body mass index of 21.67 kg/m2 and no comorbidity at the time of diagnosis. Clinical examination showed ataxic respiration while awake, mild left peripheral facial palsy, and asymmetrical elevation of the soft palate. Once again, the patient underwent polysomnography and morning arterial blood gases analysis, confirming disrupted sleep, central sleep apnoea (AHI=35 events/hour, oxygen desaturation index of 64 events/hour, time spent under 90% oxygen saturation of 287 min or 82% of total sleep time) with persistent daytime alveolar hypoventilation (PaCO2=7.64 kPa, PaO2=9.61 kPa). The AHI was 34 events/hour during non-rapid eye movement (REM) sleep and 41 events/hour during REM sleep. Prolonged periods of shallow breathing with sustained hypoxaemia were noted in non-REM as well as REM sleep (transcutaneous CO2 measurement was not available). Ataxic breathing alternated with central apnoeas and hypopneas lasting up to 59 s. Ventilatory CO2 response, assessed by the Read closed-circuit technique, was blunted (figure 1), confirming profound central chemo sensitivity impairment. Standard pulmonary function testing showed no abnormality. PHOX-2B mutation was excluded by genetic testing. Brainstem MRI showed two round hypodense defects in the area of respiratory centres (figure 2). Non-invasive bi-level nocturnal ventilation was initiated shortly after the sleep study. Although alveolar ventilation was rapidly corrected with non-invasive ventilation, nocturnal and daytime symptoms were slower to improve. In 2012, a polysomnogram while on nocturnal ventilation showed an AHI of 4.2 events/hour. Initially adherence to non-invasive ventilation was poor but gradually increased to reach a mean nightly use of 7 hours in 2014.
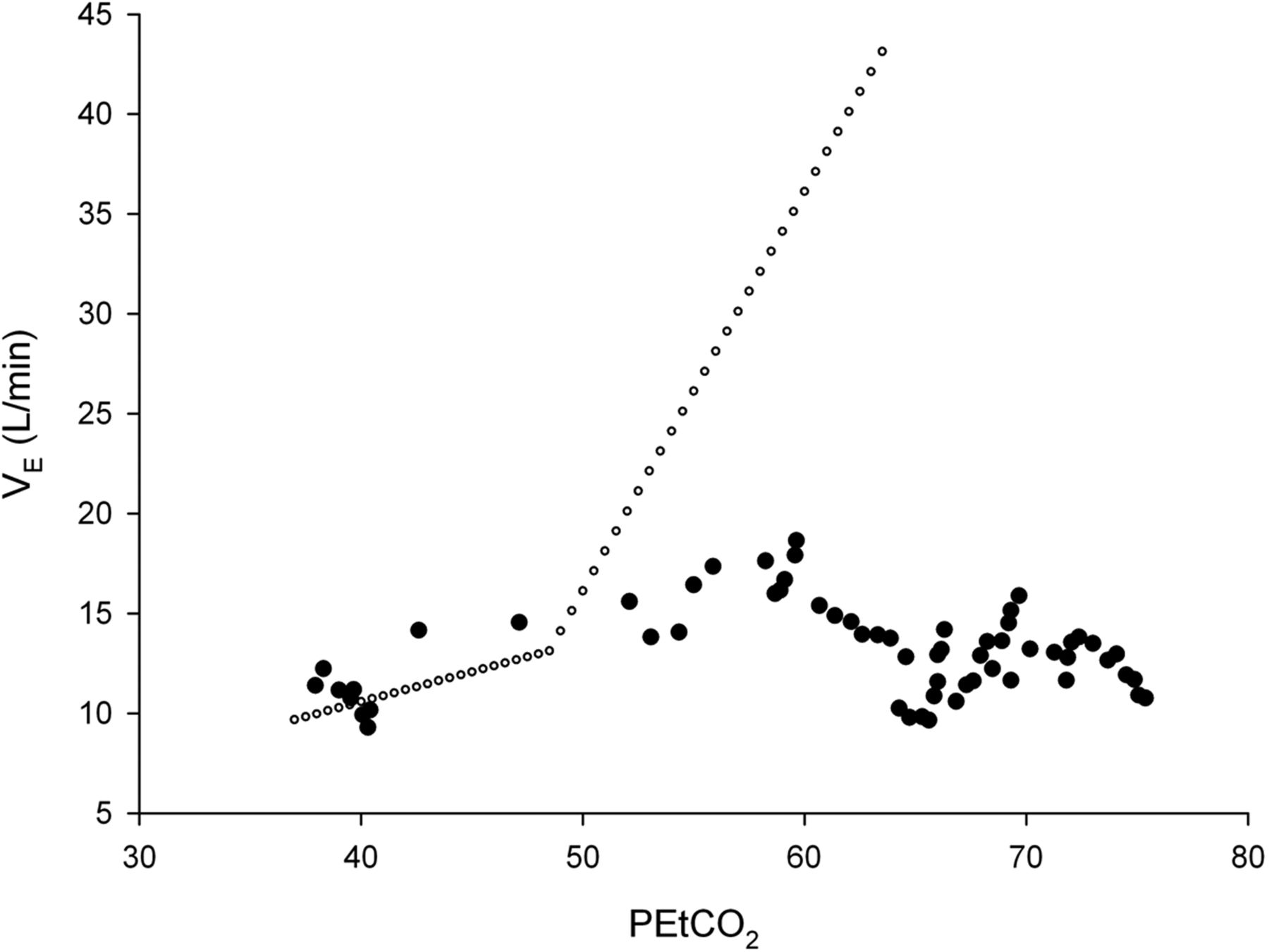
Ventilatory response to CO2 performed in 2011. The patient's response slope was 0.6 L/min/mm Hg (closed circles). The normal range for the laboratory is 1.5–3.5 L/min/mm Hg. Mean expected values are shown in open circles.
{kind=link}
{kind=link}
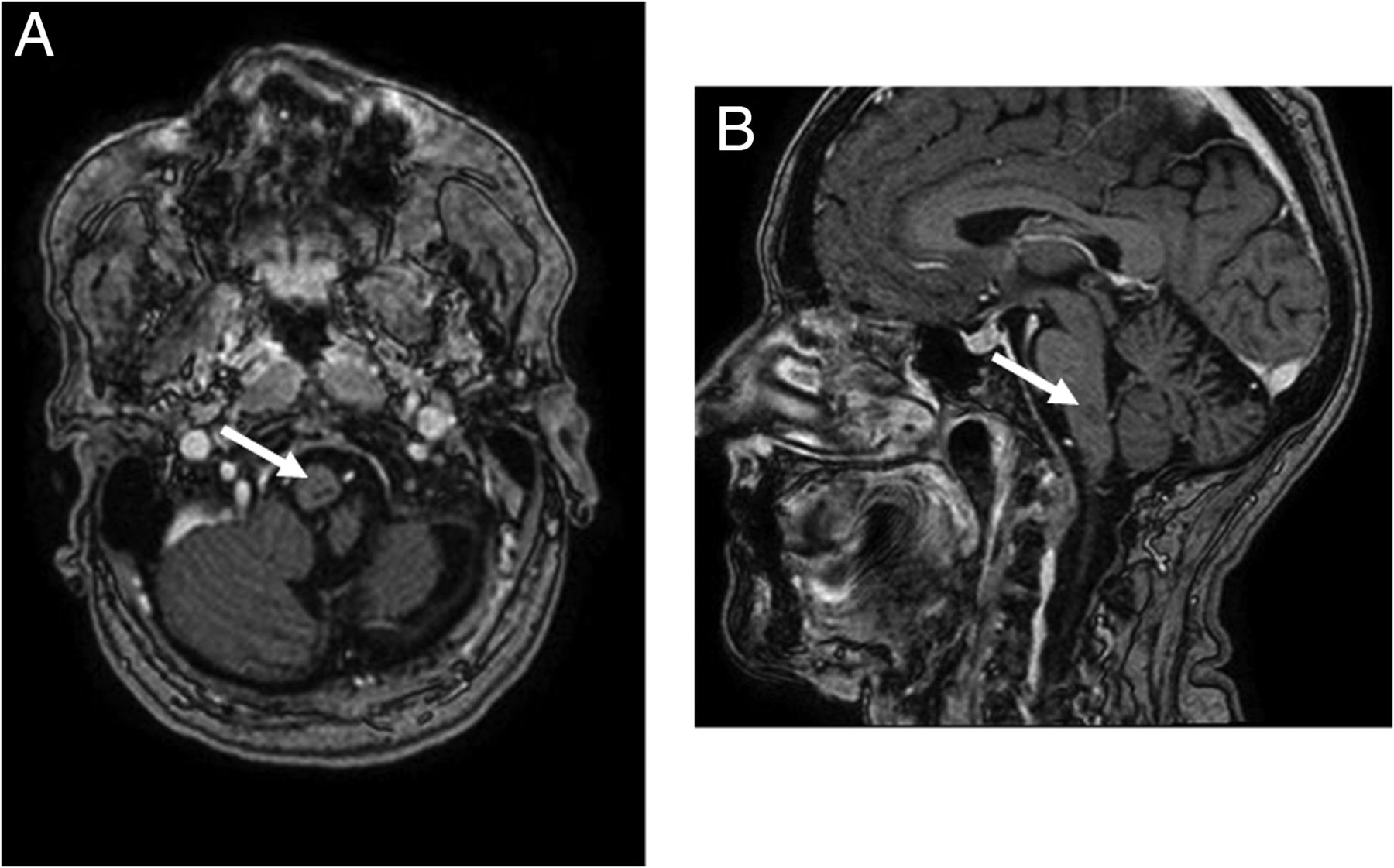
Transverse (A) and mid-sagittal (B) cerebral MRI scans performed in 2011, 34 years after severe Listeria monocytogenes rhombencephalitis, showing several small hypodense defects in the brainstem (see arrows). Moreover, severe left cerebellar atrophy is noted at the pontine level and the medulla oblongata.
Discussion
In mammals, automatic respiratory drive originates from and is modulated by neuronal networks located in the pons and medulla oblongata.1 Central chemoreceptors, which respond to variations in blood CO2 levels, are spread at the surface of the ventral medulla and allow minute ventilation adjustments to maintain PaCO2 and pH homoeostasis.2 In addition to specific respiratory centres, the neighbouring solitary tract nucleus is crucial for the control of breathing, as it integrates information from peripheral and central receptors.2 Vigilance states have a strong effect on respiratory centre control.2 Thus, it is not surprising that cases of CHS secondary to brainstem damage have been reported following infarction, compression, brainstem tethering, tumour or infection. Bilateral injury of these areas results in rapid death. However, less extensive damage may be compatible with survival but causes respiratory centre dysfunction and central hypoventilation.
LM is a gram-positive bacillus that can cause opportunistic foodborne infections and is associated with a high mortality rate.3 Because of its ability to cross the blood-brain barrier, LM can infect the central nervous system (CNS) and lead to encephalitis, meningitis, cerebellar abscess or rhombencephalitis (or brainstem encephalitis).3 Although its exact prevalence remains unknown, LM rhombencephalitis is an uncommon infection in humans.3 Unlike other forms of listeriosis, predisposing factors are usually absent in patients developing rhombencephalitis, as was the case for our patient. After a non-specific prodromal phase, evidence of brain stem dysfunction appears, often leading to a fatal outcome, particularly when treatment is delayed.3 With proper early antibiotic therapy and supportive care, the mortality rate decreases to approximately 30%, with patients often displaying neurological sequelae. Although initial blood and cerebrospinal fluid samples may be negative for LM, cultures are eventually positive thereby delaying timely diagnosis. Brain CT may be normal or inconclusive but MRI typically reveals multiple abscesses in the brain stem and the cerebellum. Autopsy may show non-specific inflammation but usually confirms the presence of unilateral or bilateral multiple abscesses located in the brainstem and cultures are positive for LM.3 In our patient, neither cerebral CT scan nor MRI scans had been performed at the time of the initial infection but cerebral MRI scans obtained 34 years after the acute episode revealed two hypodense brainstem lesions, which argue against a congenital cause which would not exhibit these types of MRI abnormalities.4 Diagnosis and treatment may be delayed because symptoms are non-specific, blood and cerebrospinal fluid direct examination are often negative and CT or MRI may be inconclusive. This delay may lead to excess mortality, particularly in immunocompromised individuals. Fortunately, this was not the case in our patient.
Ataxic respiration during wakefulness and sleep, marked daytime alveolar hypoventilation without PHOX-2B mutation (known to cause congenital CHS1), a normal pulmonary function with extreme impairment of ventilatory response to CO2, and MRI findings in our patient were consistent with a diagnosis of acquired central hypoventilation. One aspect of our case, however, was quite unusual compared to congenital CHS: the presence of clearly defined apnoeas and hypopneas. Given the history of severe rhombencephalitis, MRI brainstem lesions were considered to be a sequel of the LM abscess. The patient's brainstem lesions were unilateral, likely accounting for her extraordinary recovery. To our knowledge, this case is only the third report of LM brainstem lesions leading to acquired secondary central hypoventilation.5 ,6 The course and outcome of the acquired central hypoventilation was quite different for these three patients. The two previous patients were diagnosed with the syndrome during the acute infection,5 ,6 one died approximately 7 months later in spite of nocturnal ventilation,5 while the other, like our patient, survived but continued to require ventilator support during sleep.6 Our case is remarkable not only because of the positive outcome in spite of severe initial sepsis and CNS infection but also because of the extreme delay between the rhombencephalitis and the diagnosis and treatment of acquired central hypoventilation. Our patient presented for the first time to the Sleep Clinic with a suspicion of sleep apnoea approximately 15 years after the acute episode. Because of the patient's reluctance to pursue investigations and treatment, it took an additional 10 years to initiate non-invasive bi-level nocturnal ventilation and correct alveolar hypoventilation.
With the incidence of listeriosis rising, more cases of LM rhombencephalitis are likely to occur. Respiratory abnormalities are common during the acute phase of LM CNS infection and may be a cause of death.3 A subset of patients may apparently recover but display subclinical ventilatory control impairment due to brainstem lesions. As is the case with late-onset central hypoventilation, such patients are at risk for acute respiratory failure during anaesthesia or with concurrent pulmonary infection, opioid or sedative use.1 Thus, in the recovery phase of LM rhombencephalitis, respiratory status should be evaluated during sleep with overnight polysomnography, arterial blood gases and chemo-sensitivity testing.
Footnotes
Contributors SHL was involved in manuscript drafting. SHL, NS, MJ-F, RT and JLP contributed to the patient care and manuscript revisions.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves