Article Text

Statistics from Altmetric.com
A 42-year-old male non-smoker presented to the emergency department with a 1-month history of fever. He had no medical history. He was treated with oral antibiotics for a presumed chest infection. Initial chest radiograph (CXR) is shown in figure 1A.
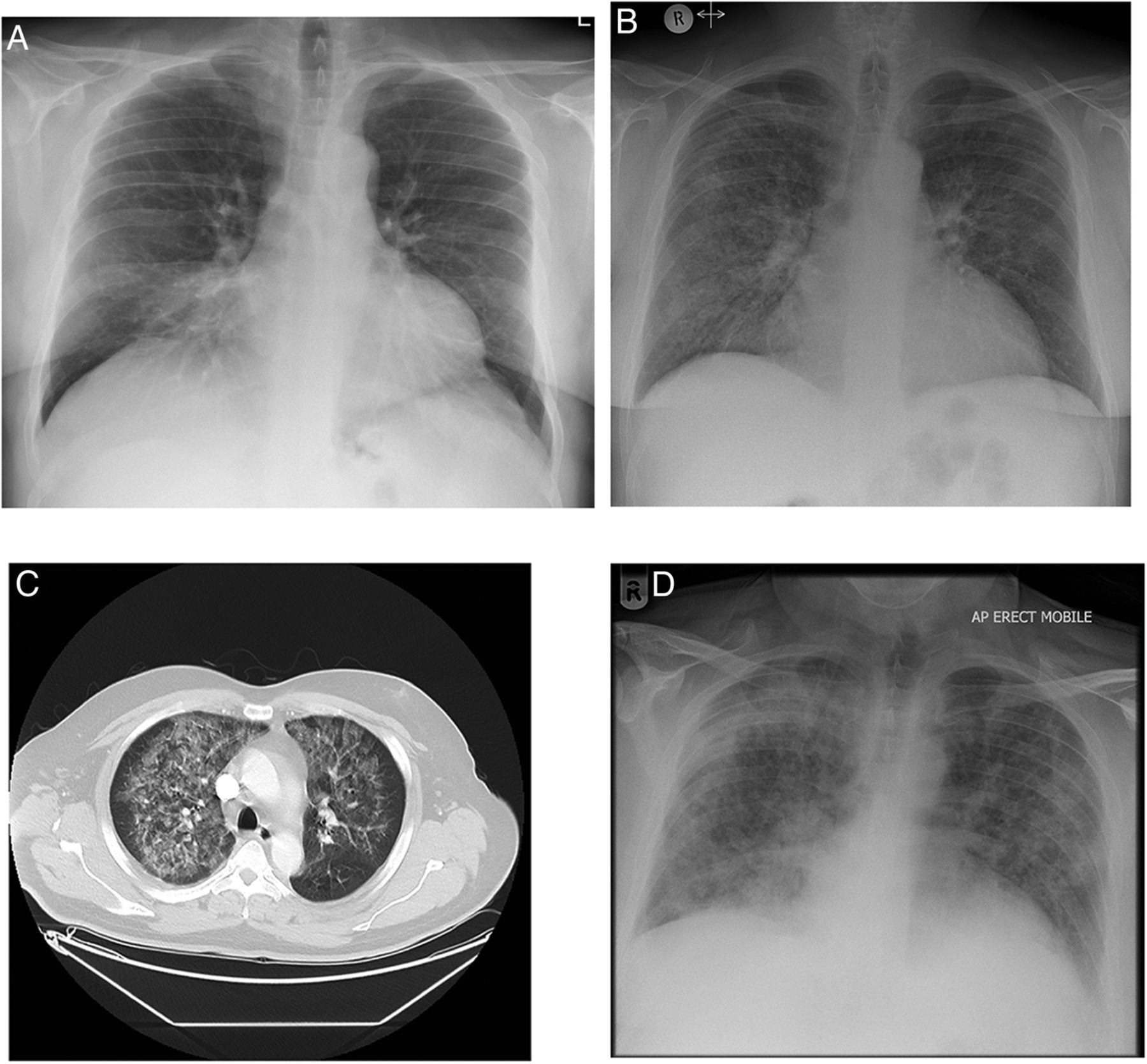
(A) Initial presentation chest radiograph (CXR). (B) Repeat CXR 2 weeks postpresentation. (C) CT chest 2 weeks postpresentation. (D) CXR at the time of rapidly worsening acute respiratory failure.
Two weeks later, he was seen in outpatients with fever, progressive dyspnoea and haemoptysis. Repeat CXR (figure 1B) was performed in addition to a chest CT (figure 1C).
He underwent urgent bronchoscopy and bronchoalveolar lavage (BAL). After the procedure, he was admitted due to persistent hypoxia.
Bedside observations: temperature 36.4°C, oxygen saturation 95% with Fio2 0.35, blood pressure 125/45 mm Hg, heart rate 105 bpm and respiratory rate 25 breaths per minute.
Chest auscultation revealed bilateral fine inspiratory crackles. Examination of the heart sounds, jugular venous pressure and peripheries were unremarkable.
Blood tests: haemoglobin 10.5 g/dL, white cell count 7.3×109/L, creatinine 100 µmol/L, alanine transaminase 48 IU/L, c-reactive protein 118 mg/L, brain natriuretic peptide (BNP) 627 ng/L. Urinalysis revealed microscopic haematuria.
BAL fluid was heavily blood stained and showed no evidence of bacterial, viral or fungal infection, including pneumocystis jirovecii. Cytology showed neutrophilia with an abundance of red blood cells.
The clinical picture was suggestive of diffuse alveolar haemorrhage (DAH), of which there is a wide differential diagnosis including vasculitis, connective tissue diseases, toxins and idiopathic pulmonary haemosiderosis.1 Autoimmune serology was sent, and on further questioning the patient denied recent inhalation of pneumotoxic substances.
He was initially treated with intravenous tazobactam+piperacillin. Once BAL microbiology was negative, pulsed intravenous methylprednisolone was initiated for presumed vasculitis.
Later that day, he underwent a precipitous deterioration in his respiratory status with Po2 dropping to 7.1 kPa, despite an Fio2 of 0.6, and rapidly worsening CXR developments as shown in figure 1D.
Question
What is the diagnosis?
Answer
DAH secondary to subacute bacterial endocarditis complicated by aortic regurgitation.
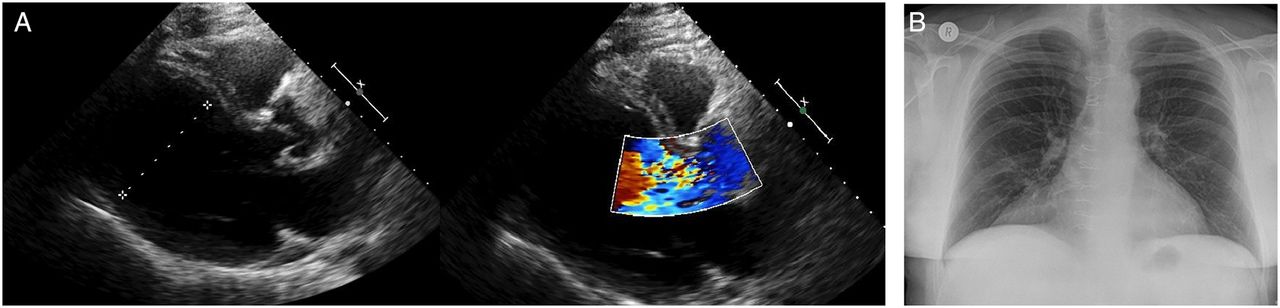
Hypoxaemia, anaemia, bilateral ground glass opacification on CT scan and erythrocyte predominance on BAL suggested DAH. However, the rapid deterioration on day 3 of admission and raised BNP prompted an urgent cardiology assessment to exclude acute left ventricular dysfunction. Bedside echocardiography revealed severe aortic regurgitation with thickened valve leaflets (figure 2A). Vegetations were confirmed with transoesophageal echocardiography and the patient underwent urgent surgery for aortic valve replacement. He was discharged 2 weeks later with a normal CXR (figure 2B). Autoimmune screen was eventually negative and he remained well with no further haemoptysis.

{kind=link}
{kind=link}
(A) Transthoracic echocardiogram with colour flow Doppler showing severe aortic regurgitation. (B) Chest radiograph on discharge from hospital.
The common causes of DAH have already been discussed above. Rarely it can be caused by mitral valve disease, mainly mitral stenosis, and rarer still is DAH associated with aortic valve disease, and the one case report that could be found in the literature was in the context of a systemic vasculitis.2
In cardiogenic DAH, the underlying cardiac valvular pathology causes an increase in left atrial pressure which induces a passive rise in backward pressure of the pulmonary vein.3 Persistent elevated venous pressure leads to abnormally engorged submucosal bronchial veins4 as well as mechanical stress failure of alveolar capillaries.5 Treatment of the underlying cause—in this case aortic valve replacement—will result in correction of cardiopulmonary haemodynamics, and therefore resolution of alveolar haemorrhage. When assessing DAH, this case emphasises the importance of considering cardiac causes, specifically aortic valve pathology which has not been described until now.
Footnotes
Contributors The authors were all involved in the clinical management of the patient this report is pertaining to. They also contributed to the writing and editing of the report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves