Article Text

Abstract
Background Obesity hypoventilation syndrome (OHS) is the most common indication for home ventilation, although the optimal therapy remains unclear, particularly for severe disease. We compared Bi-level and continuous positive airways pressure (Bi-level positive airway pressure (PAP); CPAP) for treatment of severe OHS.
Methods We conducted a multicentre, parallel, double-blind trial for initial treatment of OHS, with participants randomised to nocturnal Bi-level PAP or CPAP for 3 months. The primary outcome was frequency of treatment failure (hospital admission, persistent ventilatory failure or non-adherence); secondary outcomes included health-related quality of life (HRQoL) and sleepiness.
Results Sixty participants were randomised; 57 completed follow-up and were included in analysis (mean age 53 years, body mass index 55 kg/m2, PaCO2 60 mm Hg). There was no difference in treatment failure between groups (Bi-level PAP, 14.8% vs CPAP, 13.3%, p=0.87). Treatment adherence and wake PaCO2 were similar after 3 months (5.3 hours/night Bi-level PAP, 5.0 hours/night CPAP, p=0.62; PaCO2 44.2 and 45.9 mm Hg, respectively, p=0.60). Between-group differences in improvement in sleepiness (Epworth Sleepiness Scale 0.3 (95% CI -2.8, 3.4), p=0.86) and HRQoL (Short Form (SF)36-SF6d 0.025 (95% CI -0.039, 0.088), p=0.45) were not significant. Baseline severity of ventilatory failure (PaCO2) was the only significant predictor of persistent ventilatory failure at 3 months (OR 2.3, p=0.03).
Conclusions In newly diagnosed severe OHS, Bi-level PAP and CPAP resulted in similar improvements in ventilatory failure, HRQoL and adherence. Baseline PaCO2 predicted persistent ventilatory failure on treatment. Long-term studies are required to determine whether these treatments have different cost-effectiveness or impact on mortality.
Trial registration number ACTRN12611000874910, results.
- Non invasive ventilation
- Sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
Do continuous positive airways pressure and non-invasive ventilation provide similar benefits for initial treatment of severe obesity hypoventilation syndrome?
What is the bottom line?
The rate of treatment failure, improvement in ventilatory failure and health-related quality of life and adherence were similar in both groups after 3 months treatment.
Why read on?
This is the first trial to compare continuous positive airways pressure and non-invasive ventilation in severe obesity hypoventilation syndrome.
Introduction
Of all the complications related to morbid obesity, the development of ventilatory failure is one of the most devastating, with a fourfold increased mortality risk if untreated.1 Known as the obesity hypoventilation syndrome (OHS), this problem is increasing in prevalence in parallel with the worldwide increase in obesity2 and is the most common indication for home non-invasive ventilation in many countries.3 ,4 If not managed appropriately, individuals with OHS are at risk of pulmonary hypertension, cor pulmonale and unstable respiratory failure. Compared with eucapnic morbid obesity, OHS is associated with a higher hospital admission rate, increased use of intensive care resources and substantial mortality.1 ,5 In addition, health-related quality of life (HRQoL) and functional capacity including physical activity are reduced.6 ,7 Positive airway pressure (PAP) therapy is effective for many in controlling ventilatory failure; however, treatment failure is common.8 ,9
The optimal mode of PAP therapy for OHS has not been established. It remains unclear whether simpler, less costly CPAP directed at controlling upper airway obstruction and increasing lung volumes is as effective as Bi-level PAP therapies which, in addition, provide inspiratory pressure support to enhance tidal volume.10 ,11 Previous trials in milder OHS suggest that both CPAP and Bi-level PAP provide similar improvements in ventilatory failure, symptoms and sleepiness over a period of 2–3 months.7 ,12 One of these studies excluded patients with persistent severe nocturnal hypoventilation during their first night on CPAP.7 Furthermore, this trial used Bi-level PAP that relied on the patient's inspiratory effort to trigger support from the ventilator (spontaneous mode). Central apnoeas or failure to trigger the ventilator into the inspiratory phase may occur with this mode,13 resulting in persistent hypoxaemia and sleep disruption.14 Spontaneous-timed ventilator modes attempt to overcome this problem by providing a ventilator delivered breath in the absence of adequate patient efforts, although a recent trial in milder ambulatory patients with OHS found no benefit in comparison to CPAP.12 The present trial aimed to address these deficiencies to help resolve doubt about choice of therapy for OHS, including its more severe forms. It compared the impact of simpler, less costly CPAP with Bi-level PAP on treatment failure including hospital re-admission. Bi-level PAP was implemented in spontaneous timed mode to minimise failure to trigger the ventilator and potentially optimise the ventilatory support offered by this mode of PAP. The study included all severities of OHS, not limiting the initial severity of ventilatory failure or hypoxaemia to milder variants.
Methods
Participants
Participants with a primary diagnosis of OHS (body mass index (BMI) >30 kg/m2 and daytime PaCO2 >45 mm Hg) were recruited from the ventilatory failure services at Austin Health, the Alfred Hospital (Melbourne) and The Royal Prince Alfred Hospital (Sydney), Australia. Potential participants were excluded if they had another condition that may contribute to hypoventilation including neuromuscular disease, chest wall abnormalities, respiratory depressant medications, COPD or an FEV1/FVC ratio <70% after bronchodilators. Participants presented either as a stable outpatient referral or following a hospital admission with an acute respiratory acidosis and initial stabilisation on Bi-level PAP. Arterial blood pH was in the normal range (7.35–7.45) at randomisation for both groups. Diagnostic polysomnography was not required for diagnosis, but undertaken as clinically indicated outside the protocol. Prior ventilatory support (Bi-level PAP or CPAP) was permitted provided the duration was <1 month in the 3 months prior to enrolment.
Study design and intervention
This randomised, double-blind, parallel trial compared Bi-level PAP with CPAP in incident cases of OHS over 3 months. The Bi-level PAP group received non-invasive ventilation using a spontaneous timed mode of ventilatory support. Fixed pressure CPAP was used in the CPAP group. The protocol included a planned change to Bi-level PAP in the event of treatment failure in the CPAP group. Polysomnography was used to facilitate titration of PAP settings at randomisation (details in online supplement). CPAP or Bi-level expiratory pressure was titrated to overcome obstructive events. In the Bi-level PAP group, the ventilator rate and pressure support were titrated to overcome nocturnal hypoventilation. Supplemental oxygen was added to maintain SpO2 ≥90%. No formal dietary advice or exercise programme was prescribed.
The project was approved by the Human Research Ethics Committees at Austin Health, The Alfred Hospital and The Royal Prince Alfred Hospital and all participants provided written informed consent. The study is registered at anzctr.org.au (ACTRN12611000874910).
Supplemental material
Randomisation and masking
Demographic information, anthropomorphic data, medical history and medications were collected at recruitment. Spirometry and daytime seated arterial blood gases were measured to assess eligibility criteria. Following baseline data collection, participants were randomly assigned (1:1) using a secure web-based randomisation system (http://www.randomization.com) with a block size of four. Allocation concealment was maintained using opaque, sealed envelopes. The devices used were able to deliver both CPAP and Bi-level PAP (VPAP III STA, ResMed, Bella Vista, Australia; Harmony, Philips Respironics, USA), enabling participants and assessors to be blinded to condition.
Outcomes
Control of ventilatory failure, healthcare utilisation, mortality, HRQoL, treatment adherence and physical activity were measured. The primary outcome of treatment failure was defined, a priori, as any of hospital admission, persistent or worsening ventilatory failure (failure of PaCO2 to fall below 60 mm Hg within 3 months or a rise in PaCO2 of 10 mm Hg from baseline at any time) or non-adherence (defined as average PAP use of <2 hours per night since last review for two consecutive reviews).9 ,15–17
Hospital attendance, ventilatory failure and adherence
Seated daytime arterial blood gases on room air for at least 10 min, and anthropomorphic data were measured at baseline, 1 and 3 months. Hospital and health professional attendances, medications, oxygen usage and participation in activities (eg, work, study and household duties) were recorded after 2 weeks and at the end of each month of treatment via a structured interview. Daily PAP usage was downloaded from the device at 1 and 3 months by a separate unblinded assessor.
HRQoL, cardiovascular risk factors, pulmonary function and physical activity
Participants completed questionnaires measuring sleepiness (Epworth Sleepiness Scale),18 generic (Short Form 3619 ,20 and respiratory HRQoL (Severe Respiratory Insufficiency Questionnaire)21 at baseline and 3 months. A morning, fasted venous blood sample was taken at baseline and 3 months for haemoglobin, lipid profile, haemoglobin A1C and C reactive protein. Maximal inspiratory and expiratory pressures and physical activity (sedentary time, moderate-to-vigorous physical activity and number of steps per day) were measured at baseline and 3 months (details in online supplement).
Statistical analysis
Baseline characteristics were expressed as mean and SD or percentages with 95% CIs and compared using Student's t-test and χ2 analysis, respectively. The proportion within each group with treatment failure (primary outcome) was calculated and compared between groups with χ2 analysis, with a sample of 60 providing an 80% power to detect a 33% difference between groups.
Linear mixed models were used to examine the fixed effects of group (Bi-level PAP or CPAP), time (baseline, 1 and 3 months after commencing treatment) and their interaction, on arterial blood gas analysis, cardiovascular risk factors, physical activity and HRQoL, with the participant as a random (constant) intercept, fitted using restricted maximum likelihood and an autoregressive covariance structure to adjust for serial correlation across time (xtmixed, STATA software, V.11, StataCorp, College Station, Texas, USA). Outcomes were assessed at all three time points and the time point interaction with group was also determined. Model assumptions were verified by examining residuals plots. Intention-to-treat analysis was used. The relationship between potential predictor variables (independent predictors based on existing literature and biological plausibility) and persistent ventilatory failure at 3 months was evaluated by calculating univariate ORs (standardised for continuous variables).
Results
Participant characteristics
Sixty participants were randomised from 170 people assessed for eligibility between 1 November 2011 and 31 December 2013 (figure 1). Data collection was completed on 30 June 2014 after the recruitment target was met. Mean age was 53 years (SD 10), BMI 54.9 kg/m2 (SD 11.9) and PaCO2 59.6 mm Hg (SD 13.8) with no difference in baseline characteristics between the groups (table 1). Thirty-four participants used PAP therapy prior to randomisation, 21 using Bi-level PAP (initiated during an acute admission) and 13 used CPAP (12 as an outpatient prior to referral and 1 during an acute admission). On diagnostic polysomnography (n=47, 22 in Bi-level PAP and 25 in CPAP groups), mean apnoea hypopnoea index was 82 events per hour (SD 45.1) with oxygen saturation <90% for 67% (SD 31.4%) of sleep (no difference between groups). Two participants in the Bi-level PAP group and one in the CPAP group withdrew from the study and were not included in the analysis of the primary end point. All participants were included in the mixed models for the secondary outcome analysis. The criteria to change from CPAP to Bi-level PAP in the CPAP group did not occur prior to 3 months for any participant and all remained on CPAP. After titration with polysomnography, the mean expiratory positive airway pressure (EPAP) was 11.9 cm H2O (SD 2.3), inspiratory positive airway pressure (IPAP) 19.3 cm H2O (SD 2.8) and rate 15.0 breaths/min (SD 2.7) in the Bi-level PAP group. Mean CPAP was 15.2 cm H2O (SD 2.8).
Baseline characteristics

Flow diagram of participants through the study (consort diagram). PAP, positive airway pressure.
Primary end point: treatment failure
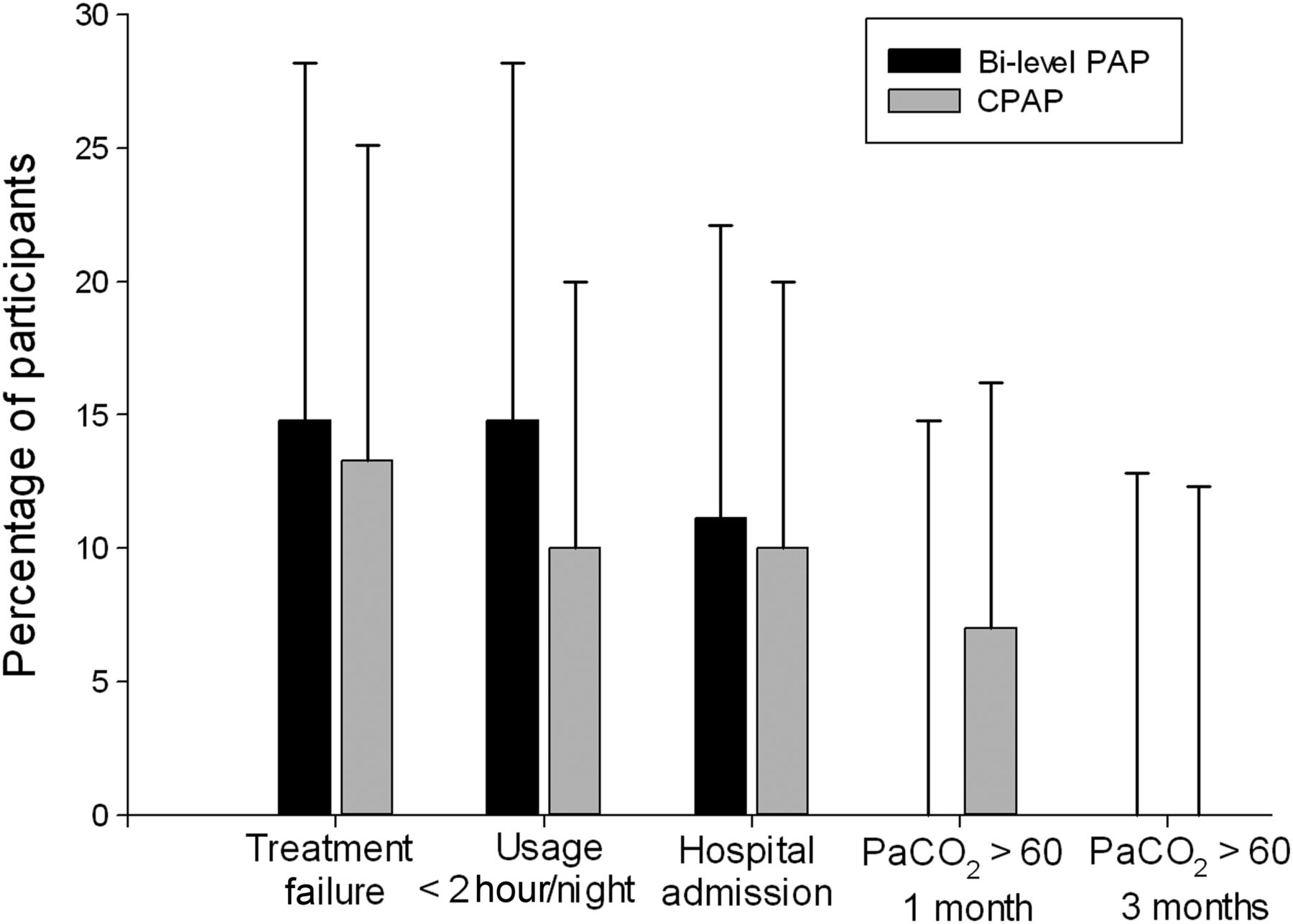
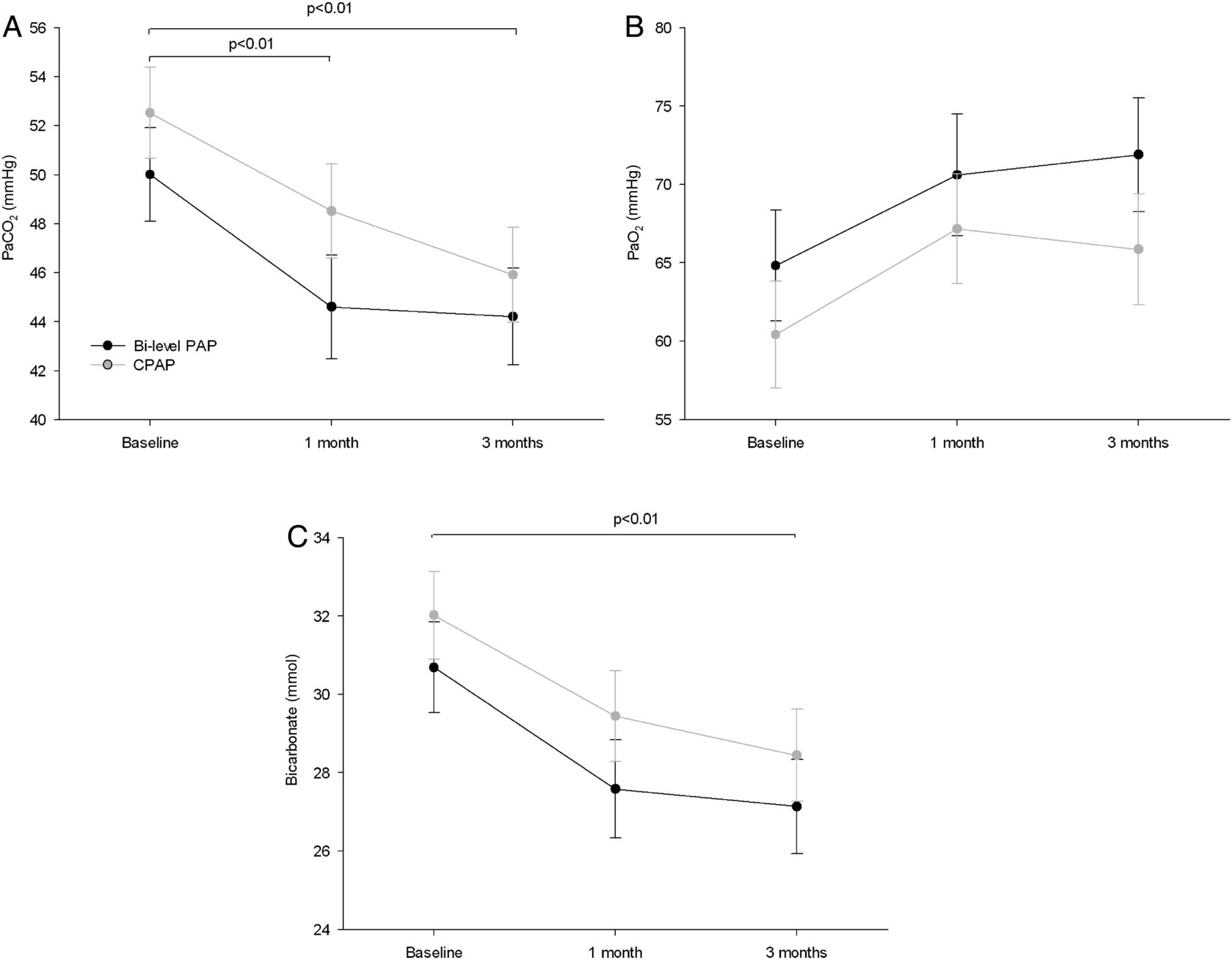
There was no difference in the proportion of participants with treatment failure after 3 months (Bi-level PAP 14.8% vs CPAP 13.3% (between-group difference 1.5% (95% CI −16.6% to 19.6%), p=0.87, Bi-level PAP n=27, CPAP n=30, figure 2). This outcome was not changed by including those that withdrew during the course of the study as treatment failures in the analysis (Bi-level PAP 20.7% vs CPAP 16.1%, p=0.65) and there was no relationship between study site and treatment failure. Adherence (mean at the final review 5.3 hours/night (2.63) Bi-level PAP, 5.0 hours/night (2.4) CPAP; adherent <2 hours/night, Bi-level PAP 14.8% versus CPAP 10.0% (between-group difference 4.8% (−12.4% to 22.0%), p=0.58), hospital admissions (Bi-level PAP 11.1% vs CPAP 10.0% (between-group difference 1.1% (−14.9% to 17.1%), p=0.89) and persistent severe hypercapnia (PaCO2 ≥60 mm Hg: Bi-level PAP 0.0% vs CPAP 6.9% (between-group difference 6.9% (−2.3% to 16.1%), p=0.20; 0% in both groups at 3 months) were each similar in both groups (figure 2). There were similar improvements in PaCO2, PaO2 and bicarbonate after 1 and 3 months of treatment in each group, but no significant treatment group by time interaction (figure 3A–C). However, there was a trend towards more patients in the CPAP group having a persistently elevated PaCO2 (>45 mm Hg) at 1 month (CPAP 65.5% (95% CI 45.7% to 82.1%), Bi-level PAP 39.1% (95% CI 19.7 to 61.5), χ2=3.59, p=0.058), but this was less evident after 3 months (CPAP 53.6% (95% CI 33.9% to 72.5%), Bi-level PAP 37.0% (95% CI 19.4% to 57.6%), χ2=1.52, p=0.218). None of the participants required supplemental oxygen after final titration of their device therapy with polysomnography. No unintended effects were reported during the study.

Treatment failure. Percentage of participants with treatment failure at 3 months, defined as device usage <2 hours per night at two consecutive reviews, a hospital admission during the trial or PaCO2 persisting above 60 mm Hg. Error bars represent 95% CI for proportion (h=hours, units for PaCO2 are mm Hg). PAP, positive airway pressure.

Daytime arterial blood gas analysis: (A) PaCO2; (B) PaO2; (C) Bicarbonate. Daytime arterial blood gas analysis at baseline (randomisation), 1 and 3 months after treatment with Bi-level positive airway pressure (PAP) or CPAP (means and 95% CIs).
Secondary and exploratory end points
HRQoL and sleepiness
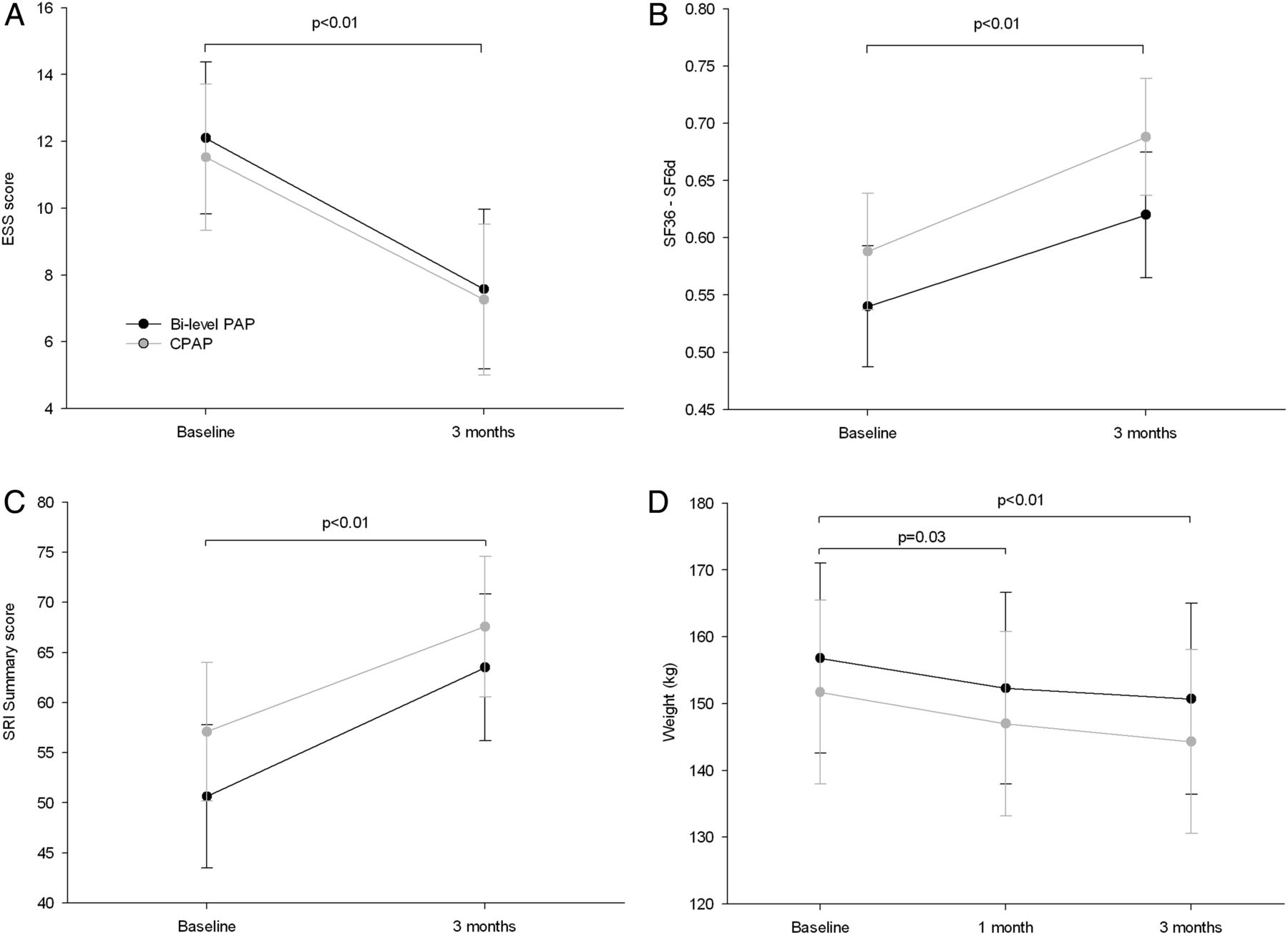
Sleepiness and HRQoL improved on treatment, with no between-group difference in the degree of improvement seen (figure 4). The mean Epworth Sleepiness Scale scores fell from a mild-level of chronic sleepiness to the normal range (11.8 to 7.4 for all participants, p<0.01, figure 4A). Generic and respiratory-specific HRQoL also improved from baseline to 3 months in both groups with improvements in all subscales apart from bodily pain (see figure 4B, C and online supplementary table S1). This included improvement in the subscales related to mental health and physical function. There were no significant group by time interactions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sleepiness, health-related quality of life and weight. (A) Sleepiness (ESS, Epworth Sleepiness Scale), (B) generic quality of life (SF36, Short Form 36), (C) respiratory-specific quality of life (SRI, Severe Respiratory Insufficiency Questionnaire) and (D) weight at baseline and 3 months after treatment with Bi-level positive airway pressure (PAP) or CPAP (means and 95% CIs).
Cardiovascular risk factors, physical activity and pulmonary function
There was no difference in cardiovascular risk markers between the Bi-level PAP and CPAP groups (table 2). Total cholesterol and high-density lipoprotein both increased after 3 months; however, there was also a non-significant trend to a rise in low-density lipoprotein. Haemoglobin A1C fell slightly and there was no change in blood pressure. Weight also fell in both groups with an average loss of 6.7 kg for all participants over 3 months (figure 4D), with non-significant increases in physical activity (table 2). Maximal inspiratory pressure increased in both groups (table 2).
Physical activity, cardiovascular markers and ventilatory function
Predictors of persistent ventilatory failure
An exploratory analysis assessed the relationship between persistent ventilatory failure at 3 months (PaCO2 >45 mm Hg) and predictor variables (see online supplementary table S2). Only PaCO2 at initial presentation was significantly related to persistent ventilatory failure (OR 2.3, p=0.03). Those in the highest quartile at presentation (PaCO2 >62 mm Hg) had more than an eightfold increased risk of persistent ventilatory failure (OR 8.2, p=0.02) compared with those in the lowest quartile (PaCO2 ≤50 mm Hg). Consistent with this finding, those with a lower pH or higher bicarbonate at presentation had a non-significant trend towards increased risk of persistent ventilatory failure at 3 months. Similar trends were observed with increasing age, lower absolute FEV1 and lower baseline respiratory disturbance index on polysomnography.
Discussion
In those with recently diagnosed OHS, this project found that CPAP and Bi-level PAP had similar rates of treatment failure and provided similar improvements in control of ventilatory failure, HRQoL and cardiovascular risk factors after 3 months of treatment, although there was a trend for ventilatory failure to remit more rapidly in the Bi-level PAP group. The project population included those with severe ventilatory failure and also used a controlled mode of ventilation in the Bi-level PAP group in order to provide this therapy in its optimal form and maximise the likelihood of identifying a difference between the groups. Persistent mild ventilatory failure was common after 3 months of treatment, with the severity of ventilatory failure at presentation the only clear predictor. These findings suggest that CPAP can be safely used to treat isolated OHS of all severities following initial stabilisation and with careful monitoring.
The very high mortality and morbidity associated with OHS has led clinicians to use PAP therapies in order to minimise these risks. While CPAP can result in substantial improvements in ventilatory failure in patients with severe obesity hypoventilation, it is clear that nocturnal hypoventilation and daytime hypercapnia may persist in some patients with OHS on this treatment.8 This is perhaps not surprising given that CPAP addresses only some of the purported mechanisms for OHS. CPAP is expected to improve the increased work of breathing related to upper airway obstruction during sleep (obstructive sleep apnoea (OSA)) and by increasing lung volumes to reduce airways resistance and flow limitation evident at low lung volumes and recruit atelectatic lung.22 ,23 However, it is not expected to overcome the work of breathing due to reduced chest wall compliance in severe obesity, nor directly correct hypercapnia by increasing tidal volume. Clinicians have sought to use non-invasive ventilation (usually Bi-level PAP) to overcome the latter issues, with OHS now the most common indication for non-invasive ventilation in many countries.3 ,4 However, our results both support and, by their inclusion of more severe cases (higher inclusion PaCO2 and BMI, and lower FVC), extend the findings of two previous randomised controlled trials of CPAP versus Bi-level PAP in suggesting that CPAP provides similar improvements in ventilatory failure and symptoms to Bi-level PAP after 3 months of treatment, regardless of mode.7 ,12 There was a trend in the current trial towards those with more severe OSA being less likely to have persistent ventilatory failure after 3 months, supporting the concept that upper airway obstruction during sleep (corrected by both CPAP and Bi-level PAP) is one of the important determinants of treatment response.24 The current project was not adequately powered to discern whether OSA severity could predict control of ventilatory failure with CPAP alone.
We found improvements in subjective sleepiness and generic and respiratory-specific HRQoL after 3 months of treatment in both groups with average sleepiness returning to normal population levels.18 ,20 Consistent with the findings from the previous randomised trials in milder and ambulant OHS, there was no difference between the CPAP and Bi-level PAP groups in this population with more severe ventilatory failure.7 ,12 Interestingly, inspiratory muscle pressures improved on PAP therapy and an increase in FEV1 was also recently reported.12 Weight loss and recruitment of atelectatic lung with increased lung volumes could explain these findings as changing functional residual capacity impacts inspiratory muscle pressures.22 ,23
OHS is associated with a high incidence of cardiovascular risk factors and cardiac failure.1 We sought to determine whether PAP may ameliorate some of these risks. Weight fell in both groups, in accordance with previous work.7 ,25 We did not assess body composition or whether some of the weight loss related to diuresis after commencing PAP therapy. However, in a previous study the fall in weight in a similar group of patients with OHS was due primarily to fat mass loss.25 Haemoglobin A1C fell slightly, suggesting improved glycaemic control. Subjectively physical functioning improved on the HRQoL scores, a potential explanation for this fall, although we were unable to demonstrate improvements in objectively measured physical activity. Increased physical activity after commencing treatment in OHS has previously been related to weight loss, specifically loss of fat.25 In the very severe population in this project, baseline activity was very low, even in comparison to previous reports in OHS.25 The lack of change in activity on treatment suggests that correction of sleepiness and ventilatory failure alone are not sufficient to improve a complex behaviour like physical activity.
The only significant predictor of persistent ventilatory failure after 3 months was the degree of ventilatory failure (PaCO2) at presentation, with an eightfold increased risk for those with a PaCO2 of >62 mm Hg. There was a trend for those with poorer ventilatory function (lower FEV1) and increasing age to have a higher risk and, as noted above, those with more frequent obstructive events during sleep tended to have better control of hypercapnia on treatment at 3 months. OHS is associated with a greater degree of ventilatory impairment than is expected for the degree of obesity alone, possibly due to more central obesity.22 This in conjunction with increased airways resistance results in increased work of breathing and it is not surprising that poorer ventilatory function predicts persistent hypercapnia. Our study population had severe OSA and it is possible that patients with OHS with milder OSA may respond differently to CPAP in comparison to Bi-level PAP. Adherence with PAP therapy has previously been related to better control of ventilatory failure, and although we were unable to clearly replicate this finding we observed a similar trend.9 In retrospective studies, predictors of survival in OHS include age, elevated inflammatory markers and low PaO2.15 Importantly, improvement in ventilatory failure (fall in PaCO2) on treatment also predicts improved survival and so this appears to be a useful marker of treatment success.
This project included participants with more severe ventilatory failure and obesity than the previous trials in OHS, but still found that CPAP provided similar benefits to Bi-level PAP. Not surprisingly, the pressures required to control upper airway obstruction were higher than in the trials in milder OHS.7 ,12 Bi-level PAP was applied in ST mode with a high backup rate in an effort to optimise ventilation, hence we are unable to comment as to whether a spontaneous mode would have provided similar effectiveness. Participants were carefully screened for other causes of ventilatory failure, hence the results are only applicable to pure OHS. While the clinical end point of treatment failure was similar in both groups, greater power and longer follow-up would be required to detect subtle differences between the groups and mortality was not addressed. The study was powered to detect a difference of 33% in treatment failure (assuming 40% treatment failure in the CPAP group), which appeared realistic based on published rates of non-adherence and persisting ventilatory failure.8 ,9 ,15 ,16 ,26 ,27 The observed between-group difference was 1.5%. The components of treatment failure (non-adherence, hospital admission and severe persistent ventilatory failure) were all considered clinically important. However, at 3 months none of the participants had persisting severe ventilatory failure so this did not contribute to the incidence of treatment failure, while 12% were non-adherent and 11% had hospital admissions. This project assessed cardiovascular risk markers, finding no difference between groups, but not cardiovascular events or cardiac function. Polysomnography was used to facilitate optimisation of PAP settings at the start of the project, although it was not used to assess control of nocturnal hypoventilation at the end of the study, relying on daytime arterial blood gases to determine control of ventilatory failure.
Conclusions
This multicentre study found that Bi-level PAP and CPAP provided similar control of ventilatory failure, hospital admissions and HRQoL in newly diagnosed OHS. Treatment adherence was also similar. It extends previous work by including patients who presented acutely to hospital with more severe disease in conjunction with using Bi-level PAP in a spontaneous timed mode to optimise the control of nocturnal hypoventilation. The severity of ventilatory failure at presentation was the only predictor of persistent ventilatory failure at 3 months. Studies of longer duration are required to determine whether there is any difference in the impact on mortality, given the high risk in this population, and whether either treatment confers a health economic advantage.
References
Footnotes
Australian trial finds that CPAP provides similar benefits to non-invasive ventilation in severe obesity hypoventilation syndrome.
Contributors MEH co-developed and drafted the protocol, conducted statistical analysis, recruited participants, drafted the manuscript and generated figures; DJB co-developed and drafted the protocol, wrote the institutional review board application, co-developed analysis, generated the random allocation sequence, assigned participants and edited the manuscript; AJP co-developed and drafted the protocol, co-developed analysis, recruited participants and edited the manuscript; AEH and BJY co-developed the protocol, recruited participants, co-developed analysis and edited the manuscript; DH co-developed the protocol and analysis and edited the manuscript. BS contributed to design, recruited participants, collected and entered data, conducted analysis and edited the manuscript; ED, DM, ATB, DF, CB, LR and NS contributed to design, recruited participants, collected and entered data and edited the manuscript.
Funding This investigator-initiated project was funded by an unrestricted grant from the ResMed Foundation, San Diego, California, USA.
Competing interests MEH reports grants from ResMed Foundation, during the conduct of the study; non-financial support from Philips Respironics, outside the submitted work. AJP reports grants from ResMed Foundation, personal fees from ResMed, personal fees from Philips Respironics, during the conduct of the study; personal fees from SenTec, outside the submitted work. DM reports grants from ResMed Foundation, during the conduct of the study; grants from National Health and Medical Research Council, grants from Victoria Neurotrauma Initiative, outside the submitted work. BS, AEH, BJY, ED, ATB, DF, CB, LR, NS, DH and DJB report a grant from ResMed Foundation, during the conduct of the study.
Ethics approval Austin Health Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.