Article Text

Statistics from Altmetric.com
Description
A 65-year-old female presented with a cavitary lesion in the right upper lung field (figure 1A). The diagnosis was aspergilloma because of the chest CT appearance of a fungus ball-like mass in the cavity (figure 1B) and treatment was started with itraconazole (200 mg/day). However, the cavitary lesion enlarged over a period of 6 months (figure 1C), with a C-reactive protein (CRP) level under 0.5 mg/dL. The patient was referred to our hospital and microscopic examination of a transbronchial lung biopsy of the cavitary lesion revealed lung cancer. A right upper lobectomy was performed. Histologically, pleomorphic carcinoma, confirmed by immunohistochemical staining, proliferated in a polypoid manner from the wall of the cavity, which consisted of malignant cells and cartilage tissues (figure 2A, B). There was no evidence of fungal elements. After surgery, the serum carcinoembryonic antigenlevel went down from 8.4 (<5.0) to 2.4 ng/mL.

Chest X-ray (A) and CT (B and C) before (A and B) and after (C) treatment with itraconazole for 6 months. A fungus ball-like mass was observed in the cavity (A–C). The cavitary lesion enlarged despite the treatment (C).

{kind=link}
{kind=link}
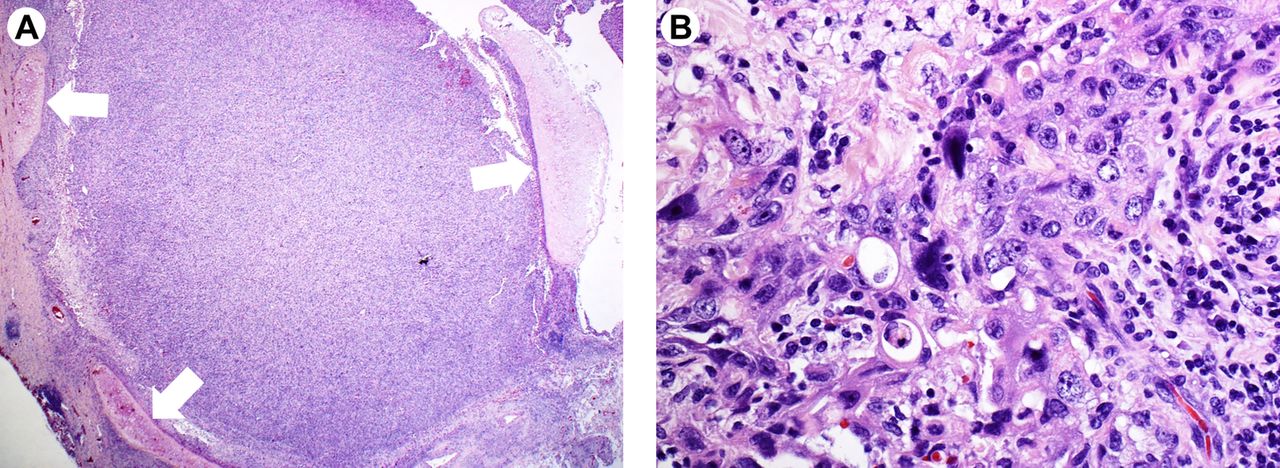
Histology of a resected specimen. Pleomorphic carcinoma proliferated in a polypoid manner from the wall of the cavity, which consisted of malignant cells and cartilage tissues (arrows) (A) and undifferentiated malignant cells without distinct architectural features (B).
A primary lung cancer has been considered to manifest a cavitary lesion in three ways: (1) cavitary necrosis of the primary tumour itself, (2) abscess formation of the lung parenchyma distal to bronchial obstruction by the tumour and (3) secondary carcinomatous abscesses induced by infected tumour emboli from the primary tumour.1 These pathophysiologies are usually accompanied by high levels of inflammatory markers reflecting breakdown of the tissue. A case of cavitary lung cancer with a fungus ball-like mass, which is extremely rare,2 ,3 manifested high levels of CRP.2 Interestingly, the wall of the cavity, but not the polypoid mass, in our patient included cartilage tissues, suggesting that the wall was derived from the bronchial wall, which was diffusely replaced by tumour cells later and probably enlarged by a check valve mechanism without breakdown of the tissue.
Although a fungus ball-like shadow suggests a pulmonary aspergilloma, comprehensive examinations including endoscopy for a differential diagnosis of lung cancer should always be considered, regardless of inflammatory marker levels.
Footnotes
Contributors Conception and design: TT, TS. Collection and interpretation of data: TT, TS, KN, FO. Drafting of the manuscript: TT, TS. Approval of the final version of the manuscript: TT, TS, KN, FO.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.