Article Text

Statistics from Altmetric.com
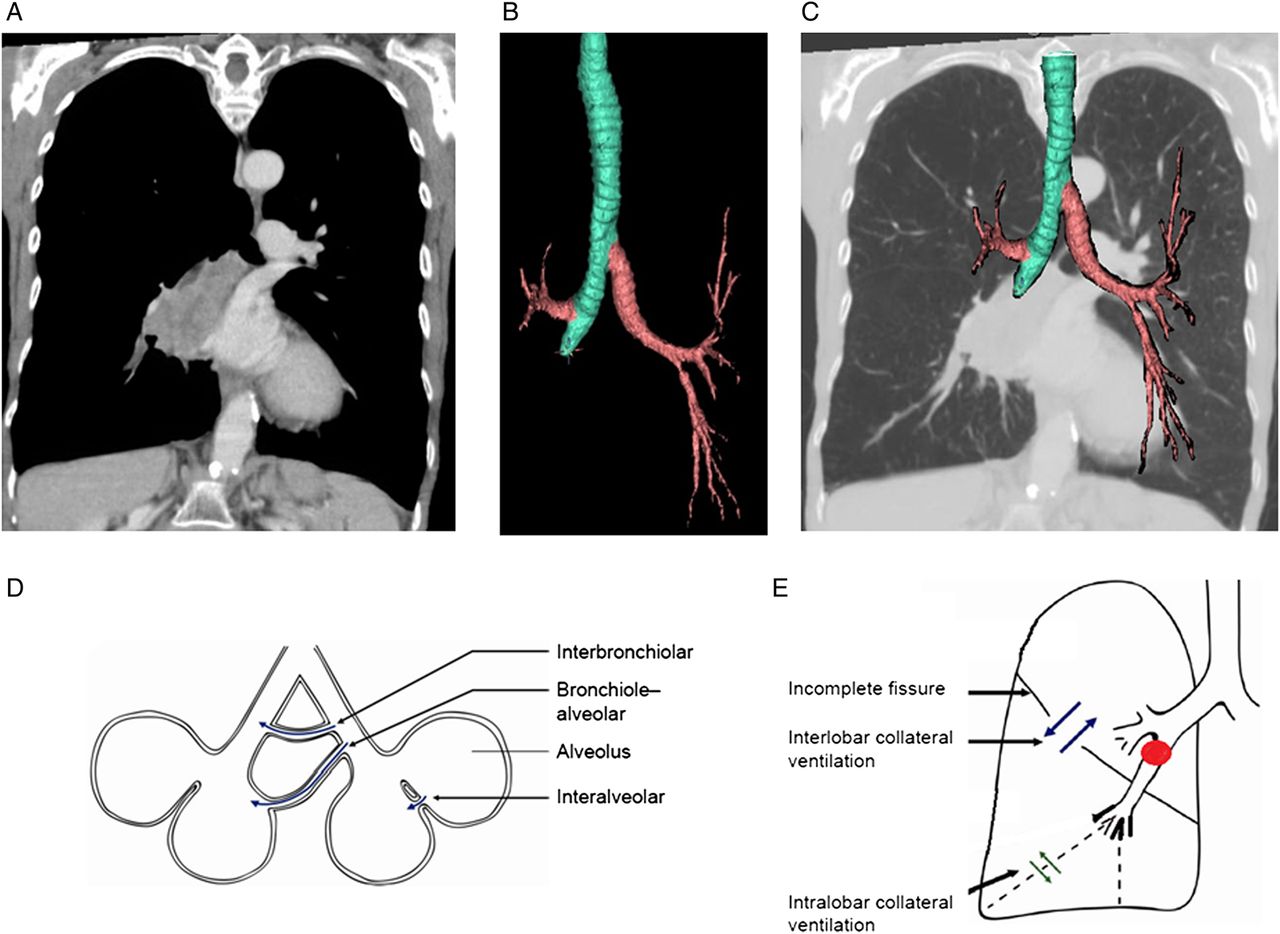
A 72-year-old female with extensive smoking history and severe emphysema presented with weight loss and failure to thrive. A large right hilar mass was found on a CT of the chest, figure 1A. Despite complete obstruction of the bronchus intermedius, there was full inflation of the right lung, figure 1B, C.

CT of the chest. (A) Coronal cut in mediastinal windows showing a large right hilar mass. The mass measured 4.1×4.5 cm and involved the right hilum and subcarinal mediastinum. There was complete encasement and endobronchial obstruction of the bronchus intermedius. (B) Airway segmentation using VIDA|vision software demonstrating the complete endobronchial obstruction of the bronchus intermedius. (C) Three-dimensional segmented airway overlaid on a coronal cut CT of the chest in lung windows. This image demonstrates that, despite the complete obstruction of the bronchus intermedius, there was full inflation of the right lung. (D) Three different pathways for collateral ventilation (adapted with permission from Koster and Slebos4). (E) Schematic figure illustrating the role of intra- and interlobar collateral ventilation (adapted with permission from Koster and Slebos4).
The finding of full lung inflation, despite complete obstruction of a central anatomical airway, demonstrates the importance and the extent of collateral ventilation in emphysema. Collateral ventilation is defined as ‘the ventilation of alveolar structures through passages or channels that bypass the normal airways’.1 Collateral ventilation occurs to a much greater extent in emphysematous lungs, as here collateral ventilation resistance is often lower than airway resistance.1 There are three possible pathways for collateral ventilation to take place, figure 1D. The first pathway consists of interalveolar communication (<5 μm in diameter) of air through the pores of Kohn. A second pathway is through accessory communication channels (30 μm in diameter) between the distal bronchioles and alveoli. The third, and likely most important pathway (80–150 μm in diameter), contains accessory respiratory bronchioles between the bronchioles of adjacent lung segments. Collateral ventilation was first only described as intralobar collateral ventilation. However, there is also interlobar collateral ventilation across incomplete fissures, figure 1E.
A possible therapy for select patients with severe emphysema is bronchoscopic lung volume reduction, which can include the insertion of one-way endobronchial valves. The goal of one-way endobronchial valves is to induce atelectasis in the most diseased lobe(s) and thus reduce hyperinflation. This reduction in hyperinflation improves respiratory mechanics and increases elastic recoil with improved expiratory airflow. If successful, this technique can lead to significant clinical improvements in select patients with emphysema. However, to achieve clinical success with one-way valve treatment, it is important to achieve complete lobar atelectasis. Thus, the absence of interlobar collateral ventilation is a precondition for therapeutic success. If a fissure is complete, there is most probably no interlobar collateral ventilation. However, incomplete fissures can occur during fetal development. Incomplete fissures are common, with a reported prevalence of 17%–85% for the right major fissure, 19%–74% for the left major fissure and 20%–90% for the minor fissure. A surrogate or indirect method to assess for the possibility of interlobar collateral ventilation is quantitative CT image-based fissure analysis.2 The presence of fissural defects on quantitative CT image analysis can predict interlobar collateral ventilation.2 Furthermore, interlobar collateral ventilation is associated with radiologically homogeneous emphysema.3
A quantitative image analysis in our patient showed relatively homogenous distribution of emphysema in the right lung and fissure integrity of the right upper lobe fissure of only 64%, figure 2. This case illustrates the extent of interlobar collateral ventilation in severe emphysema and the additional information provided by quantitative CT image analysis.

{kind=link}
{kind=link}
Quantitative analysis of the CT scans of the chest via VIDA|vision software. (A) Summary schema showing % emphysema low-attenuation areas (LAA) with attenuation values -950 Hounsfield units [HU] or less and fissure integrity (FI) by lobe. (B) Summary schema showing the lobar distribution of emphysema. The size of the spheres is reflecting the extent of low attenuation area clusters in each respective lobe. (C) Display of fissures with the dark blue shows detectable fissures, whereas the green represent fissure defects.
LLL, left lower lobe; LUL, left upper lobe; RUL, right upper lobe; RML, right middle lobe; RLL, right lower lobe.
Footnotes
Contributors SK, SB, RMR and ME contributed in the writing and revision of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.