Article Text

Statistics from Altmetric.com
COPD is a growing problem worldwide, with a staggering high number of affected subjects1 and a huge burden for society in terms of days of work lost and healthcare costs.2 COPD is closely related to smoking, and continued smoking in patients with COPD is associated with further deterioration in lung function.3 Despite elaborate societal preventive measures and smoking discouragement campaigns, smoking prevalence is still high and adolescents and young adults still start smoking. Although WHO reports a declining smoking prevalence worldwide and in many countries, there were still over 1.1 billion people who smoked tobacco in 2015.4 A population-based cohort study (inclusion 2007–2009) in adults aged more than 40 years in the Netherlands, for example, showed that overall smoking prevalence was 23% and only 34% were never smokers.5 Population surveys from 2012 in the Netherlands in age 20+ showed a similar 23% of smokers and 18% of adolescents (10–19 years) reported to have smoked in the last 4 weeks.6 Hence, despite all the efforts, smoking is still universally present and COPD continues to rise in ‘cause of death’ tables. In 2012, it was ranked third after ischaemic heart disease and stroke.7
An early diagnosis of COPD is warranted for maximal intervention in an early phase, including improving health behaviour, physical activity, smoking cessation and potential pharmacological treatment. Unfortunately, the prevalence of underdiagnosis of COPD is universally high as shown by the international Burden of Obstructive Lung Disease (BOLD) study that systematically evaluated subjects older than 40 years in the general population using standardised spirometry.8 Case-finding in subjects with respiratory symptoms has been advocated,9 but current clinical practice guidelines recommend against screening for COPD in asymptomatic patients.10 Indeed, also a very recent systematic review yielded no direct available evidence to determine the benefits or harms of screening asymptomatic adults for COPD using questionnaires or pulmonary function testing.11
Interestingly, in this edition, Soumagne et al12 published results of a well-performed, methodologically sound, prospective controlled trial, in which they evaluated 20 asymptomatic and 20 symptomatic subjects with substantial smoking history and ‘lower limit of normal’ (LLN) defined persistent airflow limitation but normal FEV1. Also 20 matched subjects with normal lung function were included. Using cardiopulmonary exercise testing, the authors were able to demonstrate that subjects who consider themselves asymptomatic have poorer exercise capacity (although not abnormal), reduced inspiratory capacity during exercise and higher BORG scores at iso-exercise and in function of minute ventilation compared with the subjects with normal lung function.
Although it is well known that symptomatic subjects with mild COPD might suffer from dynamic hyperinflation, ventilator restraints and increased exercise-related dyspnoea,13 this has been less investigated in asymptomatic subjects. Against the background of case-finding of subjects at high risk to develop a full COPD syndrome, this study has clear additive value to the debate. We need to consider the following points.
First, this study emphasises the importance of the use of LLN to distinct pathophysiology from normal ageing, most certainly in a low symptomatic population. Divergent longitudinal outcomes have been noted on population level when subjects are evaluated to have airflow limitation based on a ‘fixed ratio’ or ‘LLN’ for FEV1/FVC. In the latter, a higher risk of premature death and/or prevalence of respiratory symptoms was demonstrated.14 The study by Soumagne et al corroborate this as their results were also divergent compared with a previous study in non-dyspnoeic ‘fixed ratio’ defined COPD GOLD 1 patients that showed that 6 min walk distance was not statistically different in comparison with controls.15
Second, this study puts the value of symptom self-assessment to discussion. The modified Medical Research Council (mMRC) score is a widely used, validated and important instrument to generally evaluate the amount of exercise-related dyspnoea. However, we need to consider the hazards of labelling patients asymptomatic on the basis of a crude mMRC score and need to consider insidious nature of symptom development and adaptations to minimise dyspnoea provocation by avoidance of activity. Indeed, in another study subjects with preclinical COPD (they did not know to have COPD and 48% had mMRC of zero points) were physically more inactive compared with their smoking non-COPD peers.16
Third: so what? If subjects do not suffer from any respiratory symptom, and report mMRC score of zero which means that they only experience dyspnoea with strenuous exercise, why would it be important to treat these patients? The main reason to prescribe bronchodilator therapy is to reduce symptoms, which are not present in the first place. Many issues beyond a possible improvement in maximal exercise should be considered: costs, side effects, long-term impact, among others that require new studies. No pharmacological intervention to date has shown to alter the decline in lung function or survival in COPD. In contrast, the treatment of (asymptomatic) hypertension is key in the prevention of development of heart disease and cardiovascular-related mortality.17 Yes, an aggressive approach towards smoking cessation is warranted, which is important for many other reasons (risk reduction for cancer, cardiovascular disease, etc). In this context, we also need to realise that to date, there is no strong evidence to support the premise that supplying smokers with spirometry results improves smoking cessation rates.11 Also, smokers with mild COPD are less likely to quit smoking compared with smokers with more severe COPD.18
Fourth, we need to differentiate ‘early disease’ from ‘low active disease’. Given that these subjects developed a (very) mild degree of airflow limitation after a minimum of 15 pack-years without impact on their daily life activities, it is unclear whether this will eventually result in a sudden rapid decline in lung function and increase in symptoms. From a research perspective, it is an interesting group for longitudinal follow-up. Possibly, (some of) these subjects are less susceptible for the harmful effects of cigarette smoke.
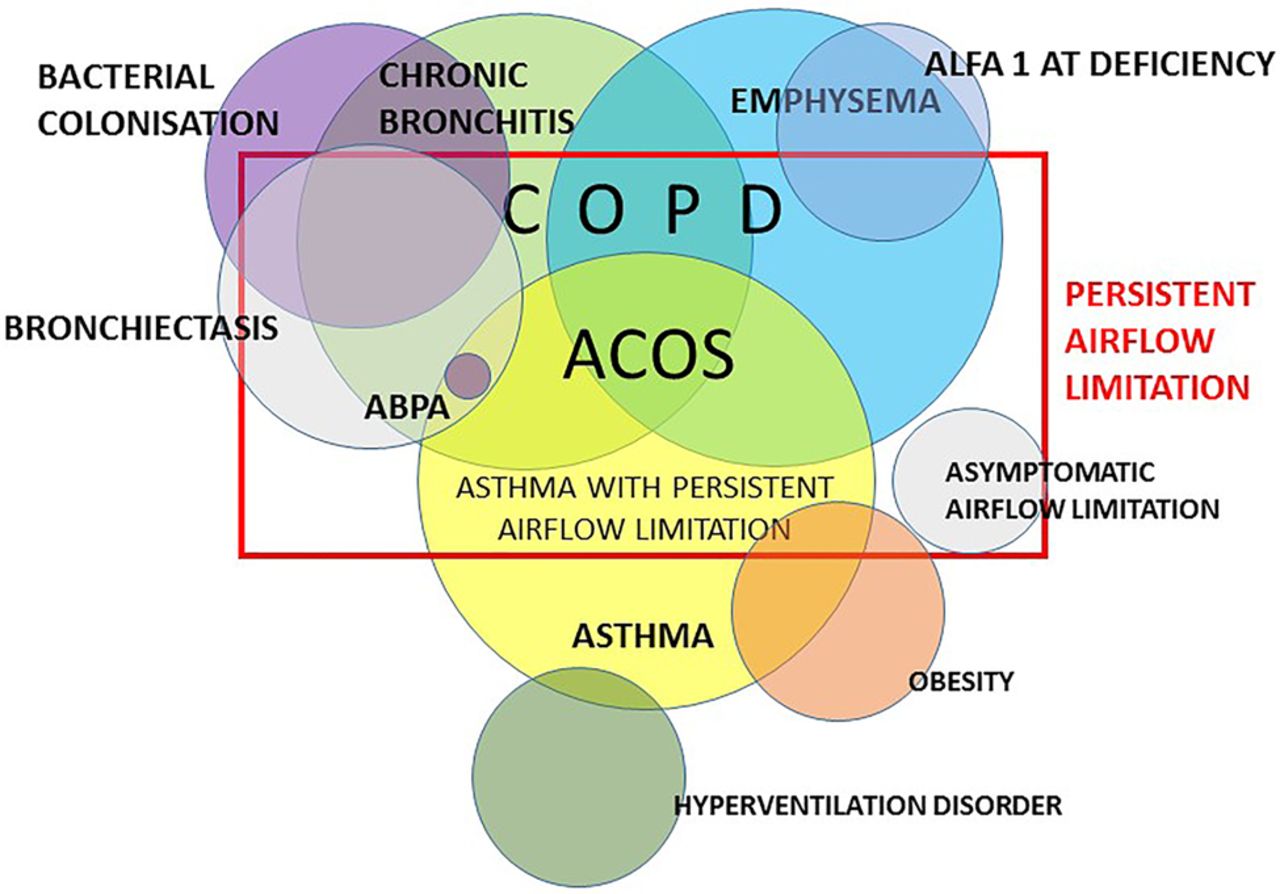
Fifth, we do not need to overestimate the value of spirometry in identifying subjects at risk. Of notice, a report of the recently published Subpopulations and Intermediate Outcome Measures in COPD Study cohort study showed that current or ex-smokers with respiratory symptoms (>10 points on the COPD assessment test) but with normal spirometry (FEV1/FVC >0.7 and FVC >LLN) have exacerbations, activity limitation and evidence of airway-wall thickening on high-resolution CT.19 Hence, ‘asymptomatic’ subjects with airflow limitation may have exercise limitation and more pronounced symptoms during exercise, but symptomatic subjects without airflow limitation may have COPD characteristics.12 ,19 Taken together, it is clear that it remains a challenge to position the role of spirometry for early intervention as subjects with airflow limitation may consider themselves asymptomatic, and on the other hand, normal spirometry results may potentially falsely reassure symptomatic subjects with a clinical ‘COPD syndrome’. Indeed, in strict sense, FEV1/FVC is just a physiological measurement, which may be part of the characterisation of different clinical disease expressions, but doubtfully a disease in itself (figure 1). Hence, the presence of airflow limitation always needs to be interpreted within a clinical context.

{kind=link}
Persistent airflow limitation in view of clinical disease expressions. ABPA, allergic bronchopulmonary aspergillosis; ACOS, asthma COPD overlap syndrome; ALFA 1- AT deficiency, alpha 1-antitrypsin deficiency.
In conclusion, airflow limitation below the LLN has consequences, regardless of the degree of symptom scores. Asymptomatic subjects, or subjects who consider themselves asymptomatic, with airflow limitation still might have lower exercise capacity and increased symptoms during exercise. This information might be important to put the self-evaluation of symptoms into perspective and strengthen the approach towards changing health behaviour. On the other hand, caution needs to be advocated to consider pharmacological treatment in asymptomatic patients, and persistent airflow limitation always needs to be evaluated within its clinical context.
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Chronic obstructive pulmonary disease