Article Text

Abstract
Background Physical rehabilitation interventions aim to ameliorate the effects of critical illness-associated muscle dysfunction in survivors. We conducted an overview of systematic reviews (SR) evaluating the effect of these interventions across the continuum of recovery.
Methods Six electronic databases (Cochrane Library, CENTRAL, DARE, Medline, Embase, and Cinahl) were searched. Two review authors independently screened articles for eligibility and conducted data extraction and quality appraisal. Reporting quality was assessed and the Grading of Recommendations Assessment, Development and Evaluation approach applied to summarise overall quality of evidence.
Results Five eligible SR were included in this overview, of which three included meta-analyses. Reporting quality of the reviews was judged as medium to high. Two reviews reported moderate-to-high quality evidence of the beneficial effects of physical therapy commencing during intensive care unit (ICU) admission in improving critical illness polyneuropathy/myopathy, quality of life, mortality and healthcare utilisation. These interventions included early mobilisation, cycle ergometry and electrical muscle stimulation. Two reviews reported very low to low quality evidence of the beneficial effects of electrical muscle stimulation delivered in the ICU for improving muscle strength, muscle structure and critical illness polyneuropathy/myopathy. One review reported that due to a lack of good quality randomised controlled trials and inconsistency in measuring outcomes, there was insufficient evidence to support beneficial effects from physical rehabilitation delivered post-ICU discharge.
Conclusions Patients derive short-term benefits from physical rehabilitation delivered during ICU admission. Further robust trials of electrical muscle stimulation in the ICU and rehabilitation delivered following ICU discharge are needed to determine the long-term impact on patient care. This overview provides recommendations for design of future interventional trials and SR.
Trial registration number CRD42015001068.
- Exercise
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
What physical rehabilitation interventions are effective for patients during critical illness and when are they best delivered?
What is the bottom line?
Evidence confirming physical rehabilitation delivered in the early stages of critical illness in the intensive care unit (ICU) produce improvements in a range of outcomes is of moderate-to-high quality, but there is insufficient evidence of effects from interventions delivered post-ICU discharge.
Why read on?
This overview comprehensively examines the existing evidence for effectiveness of physical rehabilitation in patients with critical illness and provides informed recommendations for future trial design and systematic review conduct.
Introduction
The profound physical impairments associated with critical illness are now increasingly recognised. Acute peripheral skeletal muscle wasting and dysfunction occur rapidly during the early stages of intensive care unit (ICU) admission1 ,2 and contribute to the development of ICU-acquired weakness (ICU-AW). In the long-term, deficits in physical strength, functional performance and associated health-related quality of life are evident in survivors for many years following resolution of the original illness.3–5
Rehabilitation is the cornerstone of management of critical illness-related morbidity.6 Physical-based rehabilitation interventions aim to ameliorate the effects of ICU-AW and its sequelae, and are advocated across the patient recovery continuum.7 Within the ICU, physical rehabilitation typically centres around early mobilisation encompassing a hierarchy of increasingly functional activities,8 ,9 with potential adjunctive technologies including electrical muscle stimulation10 and cycle ergometry.11 Ward-based management emphasises progression towards levels of functional performance necessary to expedite hospital discharge, which can be enhanced by coordinated multidisciplinary therapy7 and input from generic rehabilitation assistants.12 Following hospital discharge, physical rehabilitation has been characterised by delivery of either home-based or hospital-based exercise rehabilitation programmes including combined strength, cardiovascular and functional components.13
The growing interest in physical rehabilitation for critical illness patients has led to an exponential rise in the volume of published data investigating effectiveness of interventions in recent years, accompanied by multiple systematic reviews (SR) and meta-analyses aiming to integrate available evidence and generate conclusions on the most beneficial therapeutic options. These reviews include those focusing on delivery of physical rehabilitation during the peri-ICU phase and also the subsequent recovery stages post-ICU discharge. However while valuable, these individual SR are often restricted to a relatively narrow field of questioning regarding a defined ICU population, intervention, outcome and timepoint. This specificity of focus precludes a broader overview of the existing evidence base for physical rehabilitation during recovery from critical illness and limits translation of findings into clinical practice. Variability in review methodology and quality may further influence robustness of any conclusions.
The aim of this review was to conduct an overview of existing SR evaluating physical rehabilitation interventions for patients with critical illness across the continuum of recovery. The overview specifically aimed to address the following questions:
At which stage of the recovery continuum do physical rehabilitation interventions have the most effect?
Do particular patient populations gain more benefit from physical rehabilitation interventions than others?
Which type of physical rehabilitation interventions produce benefits (short-term and long-term) for post-critical illness patients?
What adverse events or harmful effects are experienced from receipt of any physical rehabilitation interventions?
Methods
Protocol and registration
The protocol for this overview, modelled on the Cochrane Collaboration approach14 and written using the Preferred Reporting Items for Systematic review and Meta-Analysis Procotol (PRISMA-P) guidelines,15 has been registered (National Institute of Health Research International Prospective Register of Systematic Reviews (PROSPERO) CRD42015001068, available at http://www.crd.york.ac.uk/PROSPERO/prospero.asp) and published previously.16
Eligibility
SR were eligible if they included and summarised the results of randomised controlled trials (RCTs) investigating the effect of any physical rehabilitation intervention following critical illness at any stage of the recovery continuum. Physical rehabilitation intervention reviews were included if they addressed: (1) exercise and/or mobility programmes for example, strengthening exercise to target specific muscles or functional activities such as lying to sitting over the edge of the bed, standing, stepping and walking; (2) use of cycle ergometers involving upper or lower limb pedalling at set levels of intensity or (3) the application of external adjuncts such as electrical muscle stimulation to enable activation of the muscle in patients unable to actively participate in rehabilitation. ‘Critical illness’ was defined as patients admitted to the ICU, irrespective of causal diagnosis but requiring invasive mechanical ventilation and multiorgan support. For reviews that included both RCTs and non-RCTs, we included the review only if we could extract the summary data from the RCTs. Further detail can be found in the online supplementary section E1.
Supplemental material
Data sources and search strategy
Data sources were searched as described in the protocol.16 There were no temporal or linguistic limitations applied and initial searches were conducted on 3 April 2015 and rerun on 29 October 2015. Full search strategies are included in the online supplementary section E2. There was no restriction on publication year for inclusion.
Overview procedure
Following removal of duplicate and non-relevant material (BC), two review authors (first search BC, LS; rerun BC, BO'N) independently screened search results based on abstract and title. Full-text systematic review selection, data extraction, synthesis and assessment of methodological quality within the overview were conducted as described in the protocol.16 Bespoke eligibility assessment and data extraction forms are presented in the online supplementary sections E3 and E4. Data extraction was conducted independently by two authors (BO'N and LS); information extracted included aims and rationale of the SR, stage of recovery continuum covered, types of studies included, population(s), intervention(s), comparator(s), primary and secondary outcomes (where specified), findings (effect size including 95% CI, results of pooling), date of last search and methods of quality assessment. Outcome measures were further categorised according to the WHO Classification of Functioning Disability and Health domains of ‘Impairment’, ‘Activity limitation’ and ‘Participation restriction’,17 with additional categories of ‘Adverse events/harms’ and ‘Healthcare utilisation’.
Quality of reporting and methodological quality of included reviews were appraised independently by two authors (BC and BB) using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)18 checklist and the Assessment of Multiple Systematic Reviews (AMSTAR) tool19 (see online supplementary section E5). The PRISMA checklist details criteria for optimum reporting of SR across Title, Introduction, Methods, Results, Discussion and Funding sections. The AMSTAR tool assesses the appropriate conduct of SR, for example, performance of duplicate study selection and data extraction and provision of characteristics of included studies. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach20 was used to assess overall quality of evidence for the interventions evaluated in included SR according to the outcomes identified. This approach assesses elements of risk of bias (methodological conduct), inconsistency (unexplained heterogeneity of results), indirectness (indirect population, intervention, control or outcomes) and imprecision (wide CIs) using the Cochrane Underlying Methodology.14 Where possible, we used information directly reported in the SR otherwise we graded the evidence.
Results
Search results
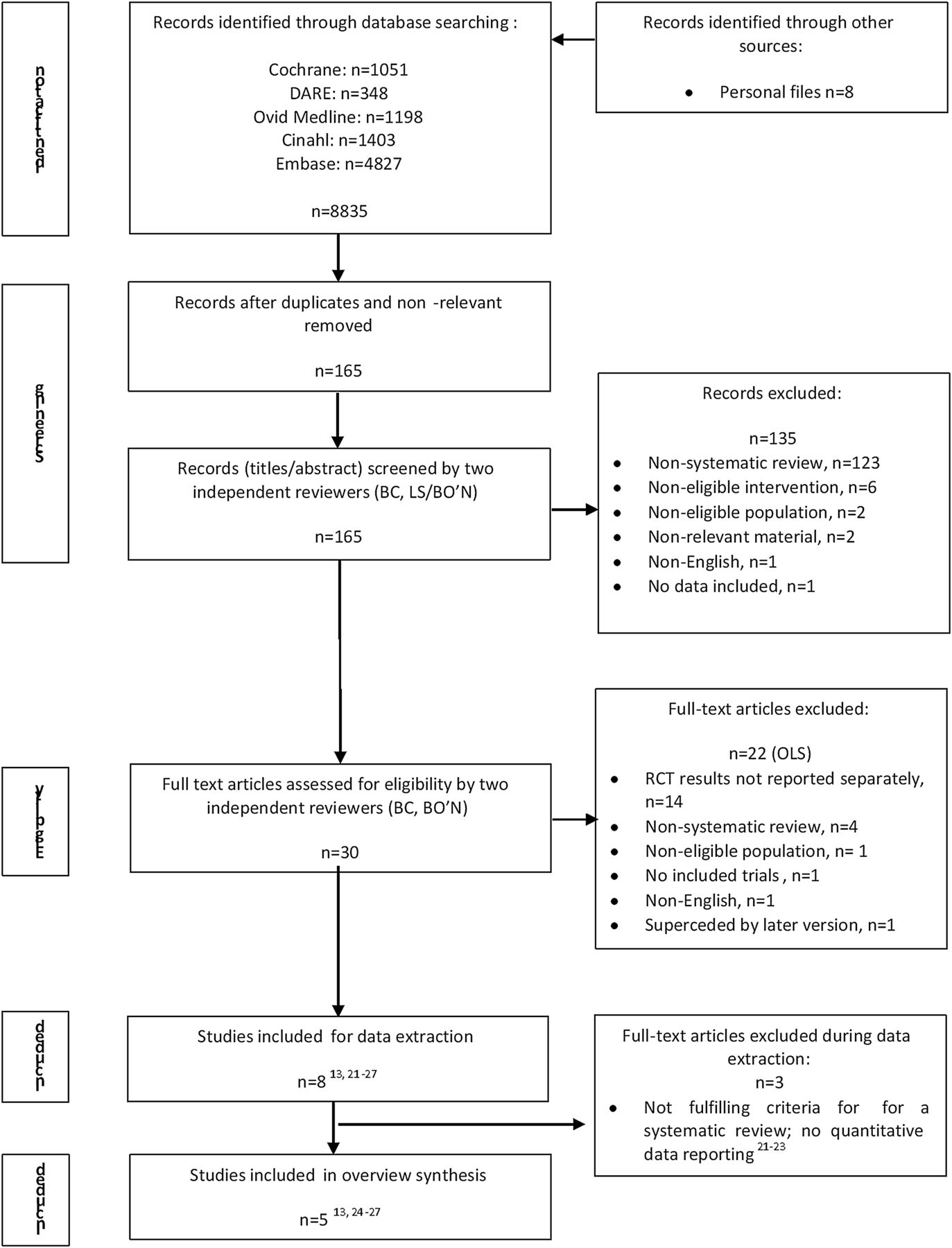
There were 8835 potentially eligible studies, with a further 8 articles identified through the authors' personal libraries (figure 1). Following de-duplication and removal of non-relevant material, and abstract screening, a total of 30 articles underwent full-text screening for inclusion. Twenty-two SR were subsequently excluded (see online supplementary section E6). Complete agreement between the two independent reviewers was evident for eligibility of full-text articles (percentage agreement=100%, κ=1.0). Arbitration by a third reviewer was not required. Three SR were further excluded during the data extraction stage.21–23 No meaningful data could be extracted from these reviews as they reported only a narrative summary and did not include or synthesise the results from included studies.

Flow diagram summarising systematic review selection. OLS, online supplementary material; RCT, randomised controlled trial.
Included systematic reviews and characteristics
Five SR were eligible for inclusion13 ,24–27 (table 1). Reviews were published between 2013 and 2015, with the most recent search date for included studies reported as 15 May 2014.13 A total of 24 relevant individual RCTs were included within the five SR, ranging between 225 and 1026 overall (see online supplementary section E7). Six RCTs overlapped across two of the included SR, and two further additional RCTs overlapped across three of the included SR. Three SR included a meta-analysis: one review assessed the effect of early physical rehabilitation and electrical muscle stimulation on the primary outcome of incidence of critical illness polyneuropathy or myopathy,25 one review assessed effect of physical therapy (multiple interventions) across a range of clinical outcomes26 and one review did not specify their primary outcome, but assessed the effect of neuromuscular electrical stimulation (NMES) on quadriceps muscle strength.27 All reviews used an objective scale to assess methodological risk of bias in their included studies.
Characteristics of included systematic reviews
Three SR focused solely on physical rehabilitation interventions delivered within ICU.25–27 One review included all stages of the recovery continuum,24 and another the post-ICU discharge stage only.13 There was overall consistency across all five SR with regard to target populations, which broadly centred on adult patients who had been admitted to the ICU with critical illness. However, individual SR reported varying levels of summary detail for characteristics of included patient populations (see online supplementary section E8). Interventions included physical or exercise-based therapy13 ,24–26 or NMES.27 Further detail of the included interventions described in included SR is reported in the online supplementary section E9. Outcome measures used to determine effectiveness of interventions within RCTs of included SR varied considerably and only three reviews specified their primary outcomes.13 ,24 ,25 Outcomes classified as reflecting ‘Impairment’17 tended to be adopted in reviews, where interventions were delivered in the ICU. Outcomes related to healthcare utilisation featured in four out of the five reviews.13 ,25–27 Three SR reported adverse events.13 ,25 ,27
Assessment of methodological quality of included systematic reviews
Median (IQR) PRISMA and AMSTAR scores were 17.0 (16.5–25.0)/27 and 7.0 (6.3–9.0)/11, respectively. Percentage agreement between the two reviewers for scoring items on the PRISMA checklist was 70.4 (66.7–85.2)% and 72.7 (59.1–81.8)% for AMSTAR items. Any disagreements were resolved through consensus and no additional reviewer was required for arbitration. Two SR, scoring highest for PRISMA scores, also scored the greatest AMSTAR scores and were classified as high quality;13 ,25 these were both Cochrane reviews. Results are reported in table 2 and online supplementary section E10.
Results for PRISMA and AMSTAR quality appraisal of included systematic reviews
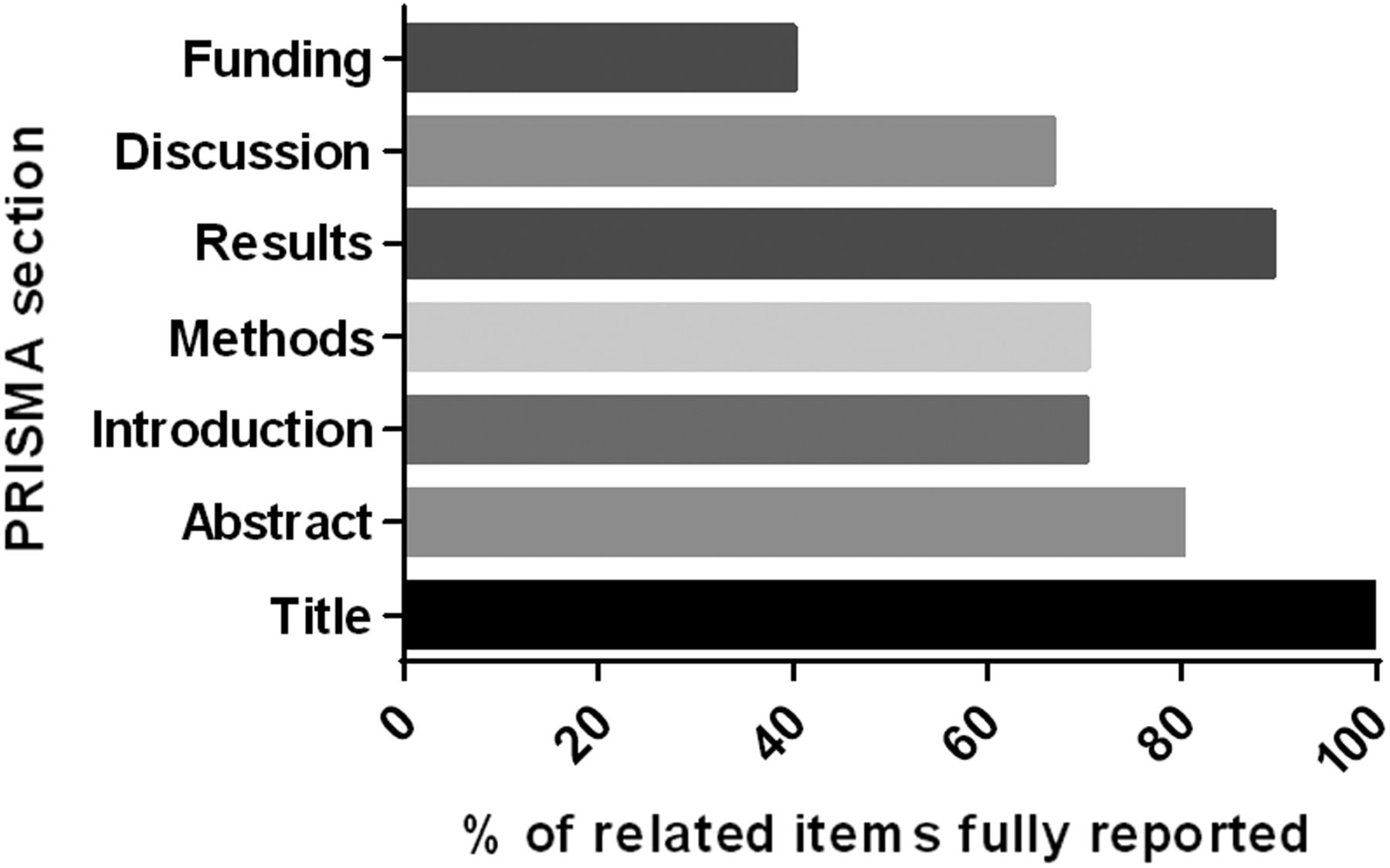
When the individual sections of the PRISMA checklist were analysed (Title, Abstract, Introduction, Methods, Results, Discussion and Funding), the ‘Title’ section was most comprehensively completed across all included reviews (100%), and ‘Funding’ the least well completed (40%) (figure 2). Figure 3 presents the frequency of each AMSTAR item that was addressed across the included SR. Items poorly completed were publication of a priori protocols, consideration of publication status as an inclusion criterion, assessment of publication bias and declaration of conflicts of interest.

Summary of PRISMA checklist section items reported across all included reviews. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.

{kind=link}
{kind=link}
{kind=link}
Summary of completion of AMSTAR items across all included reviews. For full AMSTAR item descriptors, see online supplementary section E5. AMSTAR, Assessment of Multiple Systematic Reviews.
Findings of included systematic reviews
The main findings and conclusions from each included SR are presented in the online supplementary section E11. Three SR reported benefits from delivery of early (during ICU) physical rehabilitation interventions comprising a variety of exercise, mobilisation, ergometry and muscle strengthening strategies24–26 (see online supplementary table E11). Outcomes were typically short-term, for example, peripheral muscle strength at ICU discharge, duration of mechanical ventilation, ICU length of stay (see online supplementary table E14). However, due to the heterogeneity of individual study designs and intervention protocols, it is not possible to specify a more precise therapeutic prescription. One SR reported favourable effects from electrical muscle stimulation.27 The only SR that focused on post-ICU discharge rehabilitation was unable to conclude effectiveness of any intervention.13 Only two SR evaluated adverse events associated with physical rehabilitation interventions delivered in the ICU and post-ICU discharge, and no serious adverse events were reported.13 ,25 One review reported that delivery of electrical muscle stimulation had no effect on prevention of complications, but no other specific adverse events related to the intervention itself were examined.27
GRADE summary of evidence
The summary of evidence is presented in table 3 for physical therapy interventions and table 4 for NMES interventions conducted in the ICU. We report the pooled effect sizes or other data that were directly reported in the original SR. The GRADE data extraction tables are provided in the online supplementary section E12. For physical rehabilitation interventions delivered in the ICU, there was high-quality evidence of effect for critical illness polyneuropathy and myopathy (Impairment), quality of life (Participation restriction) and ICU length of stay, hospital length of stay and hospital mortality (Healthcare utilisation). The quality of evidence for peripheral and respiratory muscle strength and respiratory function was low. For NMES interventions conducted in ICU, the quality of evidence for critical illness polyneuropathy/myopathy and muscle structure was low and for muscle strength was very low. As only one SR evaluated physical therapy interventions in the post-ICU period, results are reported according to the original SR13 (table 5). Quality of evidence for outcomes was either low or very low.
Summary of findings: intervention: physical rehabilitation; comparison: usual care
Summary of findings; intervention: NMES
Summary of findings; intervention: physical rehabilitation
Discussion
The aim of this review was to conduct an overview of existing SR to synthesise the current state of the evidence for physical rehabilitation interventions for critically ill patients delivered across the recovery continuum. We identified five SR for inclusion of either high or moderate quality, three of which included meta-analyses. The majority of reviews focused on interventions delivered during the early stage of the recovery continuum during ICU admission, with favourable effects from physical exercise-based strategies and electrical muscle stimulation on short-term outcomes. Only one review solely examined the post-ICU discharge stage and was unable to demonstrate a benefit from interventions delivered at this time. While overviews of SR have previously been conducted in other areas of clinical practice, the current overview is novel and timely in examining the evidence within the field of rehabilitation during critical illness, which has grown exponentially in recent years, and which has the advantage of allowing comparison and contrast of individual reviews to provide a précis of evidence at these different levels.28 Furthermore, we have been able to establish recommendations for future interventional study design and SR conduct.
Findings related to overview questions
Stage of the recovery continuum where physical interventions have most effect
Our results support the findings for effectiveness of physical rehabilitation interventions delivered during the ICU stay for patients with critical illness. We would suggest that there is currently no requirement for further SR on physical interventions delivered within the ICU, until the existing evidence base is supplemented by a volume of new trial data measuring functional outcomes, for example, Moss et al29 or investigating electrical muscle stimulation, an ‘in-ICU’ intervention that still requires further evidence (table 6). Future studies would benefit by including long-term follow-up in addition to short-term assessment. Further studies are required to evaluate physical rehabilitation interventions delivered post-ICU discharge including the composition of such rehabilitation interventions. The review focusing on this stage of recovery highlighted a number of outstanding studies that were not included, but which would be evaluated when fully published and included in a future update of the review.13 The results of this may yet help to inform the direction of post-ICU discharge rehabilitation research.
Recommendations and rationale for future research
Patient populations gaining greater benefit from physical rehabilitation interventions
Included reviews were broadly consistent with regard to eligible populations. However, the heterogeneity within the more detailed patient characteristic data that each review reported precluded us from identifying a specific population that gained greater benefit from physical rehabilitation interventions. Identifying target populations that respond to specific interventions may have positive impact on efficiency of rehabilitation resource utilisation. Epidemiological studies may be of benefit to characterise patient cohorts that respond to different therapies, for example, those with multiple comorbidities30 or demonstrate particular features associated with ICU admission such as a defined duration of mechanical ventilation or degree of muscle wasting.
Physical rehabilitation interventions producing short-term and/or long-term benefit
Physical rehabilitation and NMES interventions delivered early during critical illness and ICU admission were found to be most effective at improving short-term outcomes. In these instances, initiation of intervention varied from within 72 hours of ICU admission to between 7 and up to 30 days of mechanical ventilation delivery. However, the GRADE quality of evidence for these outcomes was inconsistent and varied between very low and high. One SR reported a benefit on long-term physical function although interventions were commenced at varying stages across the recovery continuum and the duration and timepoints of follow-up were inconsistent across included studies.24 In the future, defining what constitutes early rehabilitation is vital to facilitate interpreting the effects of interventions at this stage of recovery.
Adverse events or harmful effects of physical rehabilitation interventions
Only two reviews, one examining physical rehabilitation interventions within the ICU and the other post-ICU discharge, reported adverse events. Based on findings from these reviews, there appear to be minimal risks associated with delivery of interventions. However, the majority of SR did not report this outcome, either due to choice of outcome measure selection or because none of the included studies within that review reported these data. We strongly recommend that all future RCTs report the frequency and nature of adverse events pertaining to the intervention under examination or explicitly indicate, if there were no adverse events. Furthermore, all future SR, regardless of stage of the recovery continuum under investigation, should include the incidence of adverse events as an outcome measure. Furthermore, we recommend that safety criteria for commencing or stopping rehabilitation should be reported to allow a more comprehensive review of methodology to facilitate comparison in future RCTs and SR.
Critique of the overview method
This overview of SR represents a novel approach to synthesising the existing evidence base of physical rehabilitation during critical illness. We adopted a number of strategies to strengthen our review methodology. We developed a robust protocol, modelled on the process outlined by the Cochrane Collaboration for undertaking an overview of this kind14 and reported in line with recent guidelines.15 This protocol was registered on an international database (PROSPERO), and fully published a priori.16 Our search strategies were comprehensive, and we undertook duplicate screening, data extraction and quality assessments. In addition to the validated AMSTAR instrument for rating methodological quality,19 we further examined the proportion of items reported by each systematic review from the recommended PRISMA checklist,18 and applied the GRADE approach20 to summarising the quality of evidence.
There are several potential limitations to our review. We only included SR that included RCTs or where RCT findings were reported distinctly from non-RCT findings. This was the most common factor accounting for ineligibility and therefore contributed to the volume of evidence we were subsequently able to evaluate and base our conclusions on. To this end, we excluded a number of recent SR in the field, for example, studies by Parry et al31 and Li et al.32 We acknowledge a large volume of observational cohort data investigating physical rehabilitation in critical illness exists; many of these data that echo our findings have been reported in other SR that were also excluded.33 However, RCT represent the most rigorous study design to evaluate the effectiveness of an intervention and are the only data that can contribute to meta-analyses. In addition, we found considerable overlap between RCT evaluated in included and excluded SR in this overview, and where RCT did not overlap, their findings were in keeping with the results of the overview. By strictly adhering to our overview design, we have been able to focus on assimilating the findings from reviews where this was examined and reported. Clear delineation of reporting of findings from RCTs and observational study designs in a systematic review would facilitate interpretation of conclusions based on the relative weight of evidence from each category. Furthermore, we intended to appraise the quality of evidence at the level of each systematic review and for that reason we did not retrieve data from systematic review authors or primary RCTs included in reviews. This is in keeping with guidance for overview conduct,14 and as also evident in overviews from other clinical topics.34
Our overview contains SR of varying methodological quality in terms of reporting and conduct. While use of the PRISMA checklist18 to quantify the quality of review reporting is not a validated method, collecting these data along with AMSTAR scores19 allowed us to identify the main areas of SR where reporting detail was lacking. A more recent revised version of the AMSTAR tool (AMSTAR-R) has been published that provides a greater level of criterion detail for each quality item,35 this updated scoring system does not provide thresholds to classify overall quality.36 Our adoption of the GRADE approach was novel and important when developing our conclusions and recommendations to address the relative quality of evidence.20
We reran our searches such that this overview is current as of October 2015. However, due to the time-lag between the last date of a search conducted in a systematic review and its publication, there is the potential for more recent RCTs to have been published but not yet included in a systematic review. The authors are aware of a number of such RCTs.12 ,29 ,37–40 Individual review of these publications was beyond the scope and purpose of the current overview,14 and we have identified the last search date of included SR for readers' awareness of the currency of findings. We acknowledge that at present the volume of evidence for post-ICU discharge physical rehabilitation is lacking with only one published SR, which in itself is a limitation for this stage of recovery. That said, the aim of this overview was to include SR across the recovery continuum. Identifying that the post-ICU discharge phase requires greater focus of attention in the design and conduct of future trials is particularly important in the context of established critical care research priorities.41 We are the authors of one of the included SR.13 While our clearly defined eligibility criteria ensure transparent and justified inclusion of this review, and quality appraisal and data extraction were performed independently, in duplicate and using objective tools where applicable, it is possible that this introduces potential bias through insufficient independence when examining this review. That said, dual (co)authorship is increasingly typical in the conduct of overviews where expert authors may publish frequently in a particular field, and no standards have been agreed to comprehensively address this issue.42 Furthermore, as a Cochrane review, this review was subject to rigorous scrutiny during its conduct, reporting and editorial process, and data extraction pertained only to published data. Finally, due to the small number and variation in included reviews, we were unable to perform the intended subgroup and sensitivity analyses as planned in our original protocol.16
Recommendations for future research
The process of conducting this overview has informed a number of suggested recommendations for consideration with regard to the design and conduct of future trials of physical rehabilitation interventions, which are outlined in relation to the Evidence, Population, Intervention, Comparison, Outcome, Time stamp framework43 (table 6). With regard future SR in this clinical area, to ensure transparency of conduct we recommend these should be prospectively registered on a relevant database in addition to a priori publication of the full protocol in line with recognised guidelines.15 If applicable, outcome data and quality appraisal findings from RCT and non-RCT study designs should be reported separately to enhance clarity of interpretation; RCT data can contribute to meta-analyses and determine true effectiveness of an intervention. We recommend authors provide completed PRISMA18 and AMSTAR19 checklists as online supplementary material available for readers to encourage greater robustness in the reporting and methodological appraisal of reviews. In particular, based on the findings of this overview, PRISMA items related to the Introduction, Methods, Discussion and Funding sources, and AMSTAR items related to a priori Design, Eligibility, Conclusions, Methods of meta-analysis, Publication bias and Declaration of conflicts of interest should be more comprehensively addressed. This overview also identified Cochrane reviews as the highest quality. We would advise future authors to adopt Cochrane methodology where possible as a strategy to underpin review conduct and reporting.
Conclusion
This overview is the first to synthesise the systematic review evidence for physical rehabilitation interventions for patients with critical illness across the recovery continuum. Our findings confirm evidence of benefit in short-term outcomes from interventions delivered in the early stages of critical illness while in the ICU, but there is currently no evidence to conclude benefit from interventions delivered post-ICU discharge. Quality of evidence from these SR is inconsistent. We have made a number of research recommendations for design and conduct of further interventional trials and SR.
References
Footnotes
BC, BO'N, LS and BB denote equal authorship.
Contributors All authors contributed to conception and design of the overview, development of search strategies and construction of PROSPERO review registration. All authors contributed to data analysis and interpretation, and drafted, revised and agreed on the final manuscript for submission.
Funding BC's salary was funded by the Lane Fox Respiratory Unit Patient Association (LFRUPA), Guy's and St. Thomas' NHS Foundation Trust. BC is supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St. Thomas' NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. The Enhanced Recovery After Critical Illness Programme Group additionally includes: Stephen Brett, Michael Grocott, Nicholas Hart, Simon Baudouin, Danielle Bear, Stephen Bonner, Rebecca Cusack, Mark Foster, David Griffith, Robert Hatch, Sallie Lamb, Nazir Lone, Daniel F McAuley, Kathryn McDowell, Judith Merriweather, David Parkin, Natalie Pattison, Laura Price, Pamela Ramsay, Stephen Shepherd, Dorothy Wade, Timothy Walsh and Liesl Wandrag.
Competing interests The authors acknowledge they are the coauthors of one of the included systematic reviews in this overview.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves