Article Text

Statistics from Altmetric.com
A 24-year-old man was referred to the haematologists for investigation of unexplained anaemia on the background of a 6-month history of exertional breathlessness, mild cough and night sweats. Investigations revealed iron-deficiency anaemia (haemoglobin 94 g/L), thrombocytosis and markedly elevated inflammatory markers (C-reactive protein (CRP) 235 mg/L). A CT scan of his chest identified a large expansile filling defect within the left main pulmonary artery, almost entirely occluding the left-sided pulmonary circulation, which had high-grade 18F-fluorodeoxyglucose (FDG) uptake on a subsequent positron emission tomography (PET) CT (figure 1).
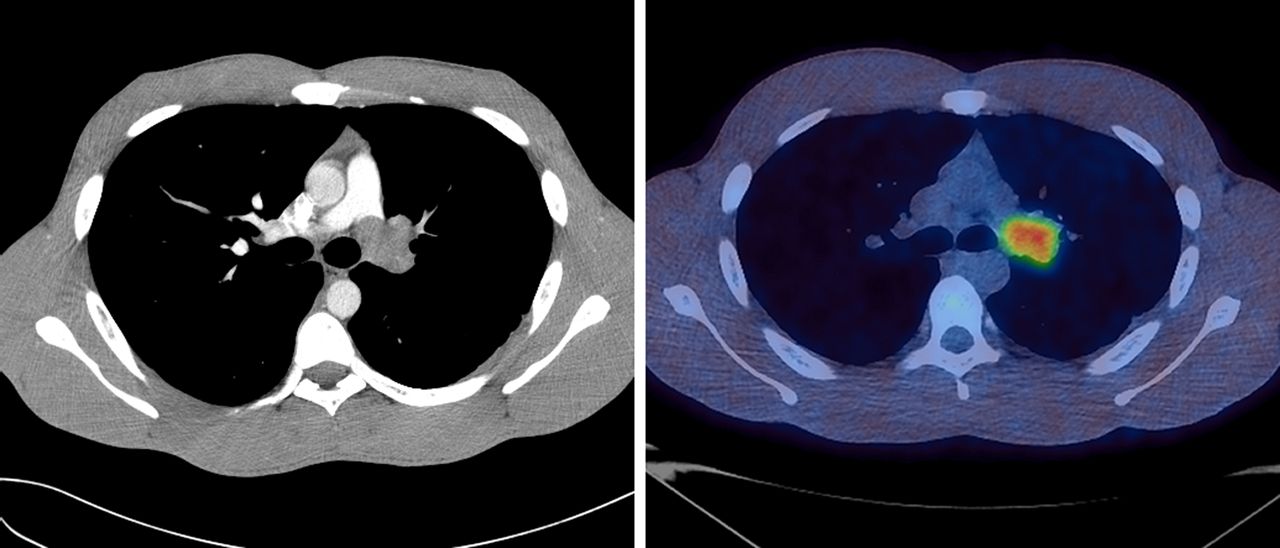
CT pulmonary angiogram and positron emission tomography CT merged image showing high-grade 18F-fluorodeoxyglucose (FDG) uptake in a 35 mm lesion within the left main pulmonary artery.
The lesion was assessed via endobronchial ultrasound (EBUS), which identified a hyperechoic soft tissue mass within the left main pulmonary artery (figure 2). EBUS-guided transbronchial needle aspiration (TBNA) of the lesion was performed without complication and rapid on-site cytological evaluation confirmed a cellular aspirate. Subsequent cytological analysis revealed large sheets of fibrotic stroma intimately admixed with small delicate vessels, spindle-shaped cells and a prominent lymphoplasmacytic infiltrate, consistent with a diagnosis of an inflammatory myofibroblastic tumour (figure 3). The lesion was subsequently surgically excised and histological evaluation of the tumour confirmed the diagnosis. The patient has recovered well with an uncomplicated postoperative period. At 4 weeks following the resection, the anaemia had resolved (Hb 132 g/L), the platelet count was normal and the CRP had fallen to 35 mg/L.
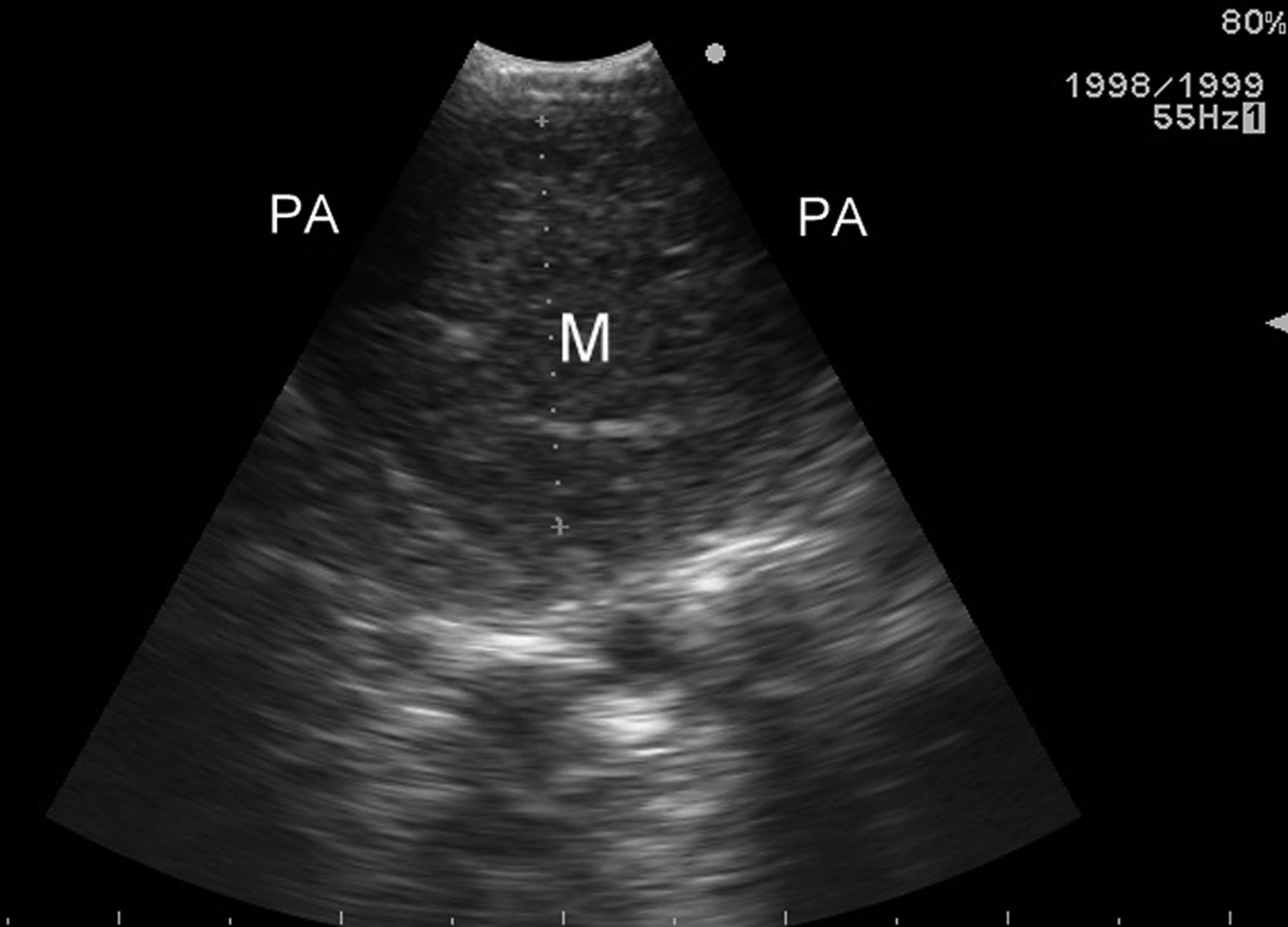
Endobronchial ultrasound image showing a hyperechoic soft tissue mass (M) within the left main pulmonary artery (PA).

{kind=link}
{kind=link}
{kind=link}
Scanning magnification view of microbiopsy fragments of the lesion obtained at endobronchial ultrasound identifying cytologically bland spindle cells and a variably myxoid stroma.
Inflammatory myofibroblastic tumours are extremely rare and represent a spectrum of inflammatory pseudo-tumours. They occur most commonly in children and young adults, and there remains an ongoing controversy as to whether these lesions are inflammatory or truly neoplastic. They typically arise in the lung but can occur in diverse extrapulmonary locations. Surgical excision is the treatment of choice and is often the route to a final diagnosis in view of common diagnostic uncertainty following biopsy.1 In 50% of cases, chromosomal translocations of anaplastic lymphoma kinase (ALK) are present and in those patients with ALK positivity on immunohistochemical staining, crizotinib (an ALK inhibitor) has been reported to be an effective treatment.2 Our patient's excision sample underwent fluorescence in situ hybridisation (FISH) and PCR, which identified no evidence of ALK rearrangements. Recurrence rates following complete excision of lung inflammatory myofibroblastic tumours are low, with a 5-year survival of >90%.3
Mass lesions within the pulmonary artery are rare and robust evidence supporting techniques for their assessment is therefore lacking. PET-CT scanning has been shown in a small study to provide excellent diagnostic accuracy when differentiating malignant pulmonary artery lesions from thromboembolic disease, with abnormal FDG uptake on PET being entirely indicative of a malignant lesion.4 Similarly, there is very little assessment of safety or efficacy relating to the use of EBUS-TBNA for the sampling of pulmonary artery lesions. A recent review5 identified 10 case reports of EBUS-TBNA for intravascular lesions, all of which yielded a diagnostic sample and reported no complications. This limited evidence supports the use of EBUS-TBNA for the safe diagnostic sampling of intravascular pulmonary artery lesions.
Footnotes
Contributors All authors wrote, revised and approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.