Article Text

Abstract
Rationale Sporadic lymphangioleiomyomatosis (LAM) is an orphan lung disease for which daily physical activity has not been studied so far and it is unclear whether a disease-specific impact beyond airflow limitation exists. Clinical correlates indicating reduced physical activity in addition to established parameters like airflow limitation and hypoxaemia are largely undetermined.
Method We measured physical activity (steps per day, SPD; physical activity level, PAL; minutes of moderate activity, MMA) in 34 women with LAM, 32 FEV1-matched female patients with COPD and 15 age-matched healthy women for 1 week using an accelerometer. In addition, we assessed lung function measurements, questionnaires for generic and respiratory health status (12-Item Short Form Survey, SF-12; St. George's Respiratory Questionnaire, SGRQ), dyspnoea (modified Medical Research Council dyspnoea scale, mMRC) and fatigue (Multidimensional Fatigue Inventory, MFI-20).
Results Patients with LAM (mean age 52.7 years, mean FEV1 62.7% predicted) showed reduced SPD, PAL and MMA (p<0.01) compared with healthy controls and reduced MMA (p=0.032) compared with female patients with COPD (mean age 65.2 years, mean FEV1 62.6% predicted). In multivariate regression analyses, adjusting for FEV1 and long-term oxygen therapy, either generic health status (SF-12 physical health) or fatigue (MFI-20) were the strongest independent predictors for SPD in patients with LAM (p=0.006 and p=0.004, respectively).
Conclusions Physical activity in daily life is substatially reduced in LAM, when compared with healthy controls and COPD - indicating a disease specific impact. The regular assessment of fatigue and generic health status may improve disease management in LAM by taking daily physical activity of patients with LAM more adequately into account.
- Rare lung diseases
- Exercise
Statistics from Altmetric.com
Sporadic lymphangioleiomyomatosis (LAM) is a rare lung disease that affects almost exclusively women. It is characterised by cyst formation leading to airflow limitation, ventilatory limitations and gas exchange impairment, resulting in dyspnoea and exercise intolerance.1 Daily physical activity is an important clinical outcome parameter in common lung diseases, such as COPD.2 However, rare lung diseases such as LAM have not been studied so far and a disease-specific contribution to daily physical activity beyond airflow limitation is uncertain. In LAM, fatigue is a highly prevalent feature that has been overlooked in the past3 and that might be associated with levels of daily physical activity in this debilitating disease, just like health status and dyspnoea. Here, we hypothesised that physical activity in patients with LAM is substantially lower than in healthy controls but comparable with patients with COPD. In addition, we hypothesised that clinical variables other than airflow limitation and hypoxaemia might be associated with physical activity in patients with LAM.
We measured physical activity in 34 female patients with LAM, 32 female patients with COPD and 15 healthy women for 1 week using an activity monitor (SenseWear Armband; BodyMedia, Pittsburgh, USA) measuring steps per day (SPD), physical activity level (PAL) and minutes of at least moderate activity per day (MMA), as previously described.2 We recruited patients with LAM (mean age 52.7 years, mean FEV1 62.6% predicted, long-term oxygen therapy (LTOT): n=12 (35%)) during the annual meeting of the German LAM patient group. Patients with COPD (mean age 65.2 years, mean FEV1 62.7% predicted, LTOT: n=6 (19%)) were derived from an existing cohort4 and matched for FEV1 and body mass index (BMI). Dyspnoea and health status were similar between groups. Healthy controls were recruited from our institutional database5 and matched for age and BMI (see online supplementary table E1 for detailed characteristics). All participants provided written informed consent (ethics approval AZ 038/12 II/AZ 185/08; German Clinical Trials Register Number DRKS00006170). Lung function parameters of patients with LAM were taken from the last available lung function report. Participants filled out questionnaires for generic and respiratory health status (12-Item Short Form Survey, SF-12; St. George's Respiratory Questionnaire, SGRQ), dyspnoea (modified Medical Research Council dyspnoea scale, mMRC) and fatigue (Multidimensional Fatigue Inventory, MFI-206) at home and sent them back together with the activity monitors at the end of the measurement.
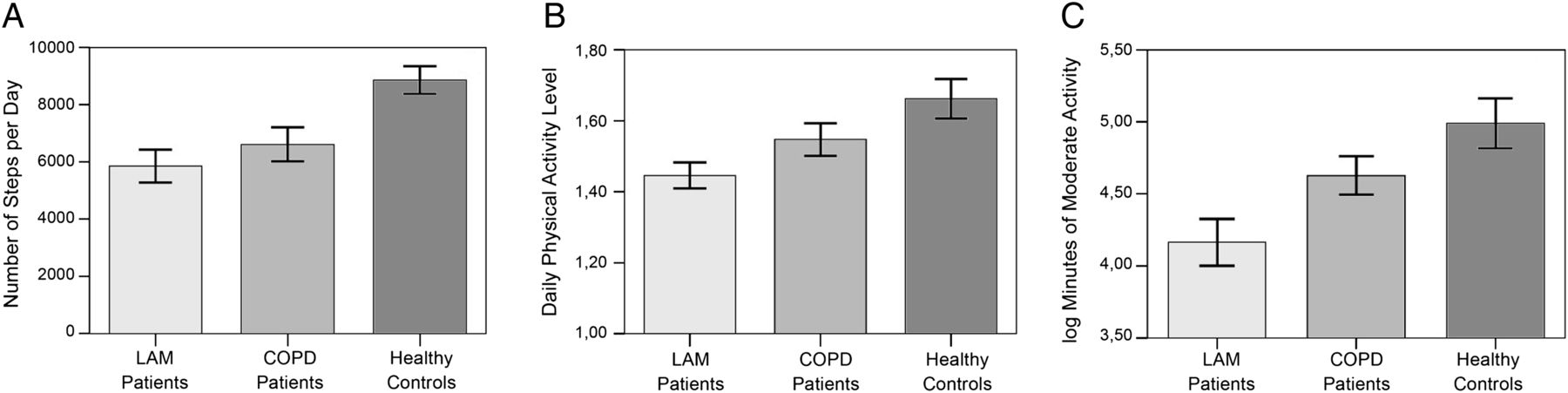
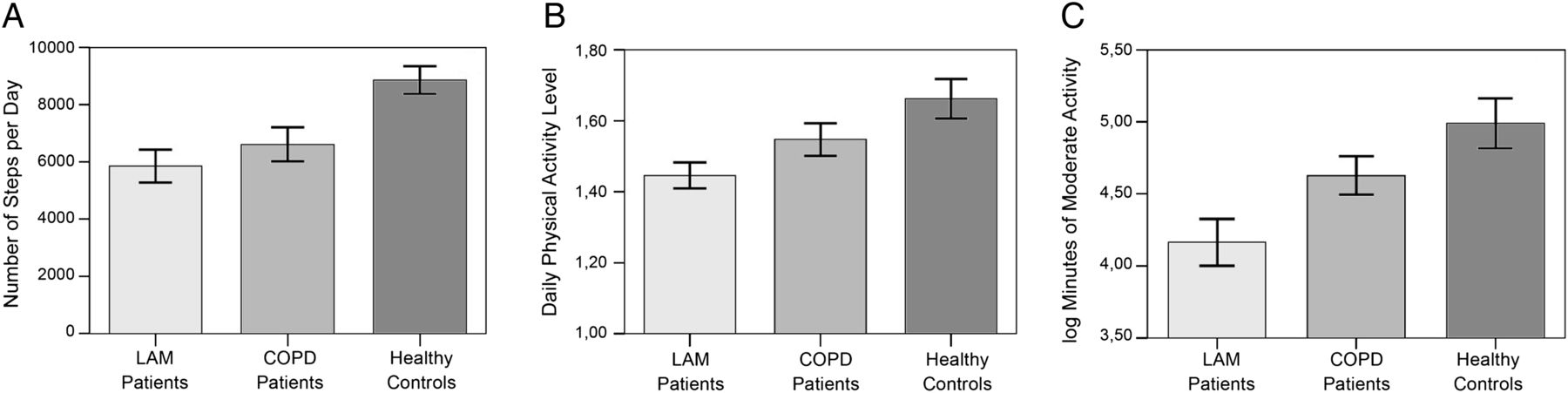
Compared with healthy controls, each of the three physical activity parameters (SPD, PAL and MMA) was significantly reduced in patients with LAM (figure 1). Unadjusted comparison between patients with LAM and COPD showed reduced MMA in LAM (figure 1), despite the significant age difference and equal dyspnoea and health status scores. Adjusted for age and LTOT as possible confounders, multivariate regression analyses showed significantly lower MMA and PAL in patients with LAM compared with COPD (p=0.006 and p=0.005, respectively), whereas SPD were not significantly lower (p=0.152) (online supplementary table E2). A potential explanation for this observation might be that patients with LAM walk at lower intensities compared with patients with COPD.
{kind=link}
Physical activity of patients with lymphangioleiomyomatosis (LAM) (bright bar) compared with patients with COPD (light grey) and healthy controls (dark grey) expressed as mean±SE. (A) Number of steps per day (5852±3327 vs 6616±3351 vs 8863±1884; reduction by 12% vs 34%; p=0.360 and p=0.002, respectively). (B) Daily physical activity level (1.45±0.21 vs 1.54±0.26 vs 1.66±0.22; reduction by 24% vs 32%; p=0.087 and p=0.002, respectively). (C) Log transformed minutes of at least moderate activity per day (corresponding medians (IQR) were 61 (26–147) vs 107 (46–78) vs 153 (97–207); reduction of the median by 43% vs 60%; p=0.032 and p=0.006, respectively).
Supplementary table 2
MULTIVARIATE REGRESSION ANALYSES FOR THE PHYSICAL ACTIVITY OUTCOME PARAMETERS STEPS PER DAY, PHYSICAL ACTIVITY LEVEL AND MINUTES OF MODERATE ACTIVITY IN LAM COMPARED TO COPD
Airflow limitation, health status, dyspnoea and fatigue scores correlated best with SPD as outcome variable (online supplementary table E3). In multivariate regression analyses, adjusting for LTOT and FEV1, either SF-12 physical health or MFI-20 were the strongest independent predictors for SPD in patients with LAM (total R2=0.476, partial R2=0.178, p=0.006 and total R2=0.449, partial R2=0.207, p=0.004, respectively) (online supplementary table E4).
Supplementary table 3
AGE-ADJUSTED ASSOCIATIONS BETWEEN STEPS PER DAY AND CLINICAL VARIABLES (A-G) IN PATIENTS WITH LAM
Supplementary table 4
FINAL MULTIVARIATE MODELS (A/B) CONTAINING THE STRONGEST INDEPENDENT PREDICTORS FOR STEPS PER DAY IN PATIENTS WITH LAM
Measures on exercise capacity (eg, 6 min walking test) and associated hypoxaemia might explain further variance in the data. The lack of these measurements is a clear limitation of our study.
We show for the first time that physical activity in daily life is substantially reduced in LAM patients, when compared with healthy controls and COPD patients with similar functional limitation, dyspnoea and health status—indicating a disease-specific impact. The underlying processes, however, are to be elucidated in further studies. Although airflow limitation and hypoxaemia—as indicated by FEV1 and LTOT—are well-established predictors for impaired physical activity, we propose to include fatigue and generic health status into the standard clinical assessment of patients with LAM. Awareness and measurement of both features will help to improve adequate disease management in this debilitating disease.
Acknowledgments
The authors thank the patients of German LAM foundation (‘LAM Selbsthilfe e.V.’) for supporting this study. We thank Daniela Beissel for her excellent assistance with study logistics.
Footnotes
Contributors TB had full access to all of the data and takes full responsibility for the integrity of the data and the accuracy of the data analysis. TB: contributed to statistical analysis and interpretation of the data and drafting of the manuscript. HW: contributed to conception and design of the study, acquisition, analysis and interpretation of data and drafting of the manuscript. BW: contributed to statistical analysis and interpretation of the data and drafting of the manuscript. MG: contributed to statistical analysis and critically revised the manuscript. HM: contributed to conception and design of the study and critically revised the manuscript. KFR: contributed to conception and design of the study and critically revised the manuscript. HW: contributed to conception and design of the study and critically revised the manuscript. DK: contributed to conception and design of the study and critically revised the manuscript. AK: contributed to conception and design of the study, analysis and interpretation of data and drafting of the manuscript. All coauthors critically revised the article and gave final approval of this version to be published.
Funding The work was supported by ‘Wissenschaftliche Arbeitsgemeinschaft zur Therapie von Lungenerkrankungen’ (WATL e.V.).
Competing interests None declared.
Ethics approval Ethics Committee Schleswig-Holstein, Bad Segeberg, Germany; AZ 038/12 (II) and AZ 185/08.
Provenance and peer review Not commissioned; externally peer reviewed.