Article Text

Abstract
The value of FENO measurements in patients with symptoms suggestive of asthma is unclear. We performed an observational study to assess the ability of FENO to diagnose asthma and to predict response to inhaled corticosteroids (ICS). Our findings suggest FENO is not useful for asthma diagnosis but is accurate at predicting ICS response.
- Asthma
- Asthma in primary care
- Exhaled Airway Markers
Statistics from Altmetric.com
Introduction
Data suggest that up to 40% of patients diagnosed and treated for asthma with inhaled corticosteroids (ICS) have no evidence that this treatment is needed.1 Overdiagnosis of asthma is common because symptoms of the condition are non-specific2 and there are no readily available tests to confidently exclude asthma.
Proposed National Institute for Health and Care Excellence (NICE) guidelines consider measurement of FENO levels in the diagnostic algorithm,3 although a recent meta-analysis concluded that the sensitivity and specificity of FENO was insufficient for accurate diagnosis.4 An alternative approach for the use of FENO in patients with symptoms suggestive of asthma is to identify individuals who are likely to have TH2 high inflammation and therefore likely to respond to ICS.5
We aimed to establish if FENO measurements can (1) accurately diagnose asthma in patients presenting to primary care and (2) reliably distinguish which patients will benefit from ICS treatment.
Methods
Adult patients with respiratory symptoms suggestive of asthma who were thought to require ICS treatment by their general practitioner (GP) were prospectively identified (see online supplementary data).
Supplementary tables
After consenting to the study (REC12/EM/0241), participants attended a baseline visit at which FENO (NIOX MINO; Aerocrine, Tolna, Sweden), spirometry, methacholine challenge, sputum induction for sputum cell count, asthma control questionnaire (ACQ) and asthma control test (ACT) were measured and those willing returned the following day for reversibility testing with 400 μg salbutamol inhaled via a spacer. Participants then started their GP-prescribed ICS, which was predominantly beclomethasone dipropionate (200 μg twice daily) via a metered dose inhaler, and returned at 4 and 12 weeks for repeat FENO, spirometry, methacholine challenge, ACQ and ACT.
Diagnosis of asthma was defined as one or both:
Reversibility of ≥12% and ≥200 mL in FEV1
Provocative concentration of methacholine (PC20) of ≤8 mg/mL
Response to ICS was predefined as a combination of two of any of the following objective criteria or one objective criterion and one subjective criterion from the following predetermined criteria:
Objective:
Increase in FEV1 from baseline of ≥12%
Increase in PC20 ≥ one doubling dose6
Decrease in FENO of ≥20% for baseline values >50 ppb or decrease of ≥10 ppb for baseline values ≤50 ppb7
Subjective:
Decrease in ACQ of ≥0.5
Increase in ACT of ≥3 points
Data were entered into Stata (Statacorp, Texas, USA) and receiver operator characteristics (ROC) analysis was carried out in Stata and GraphPad Prism.
Results
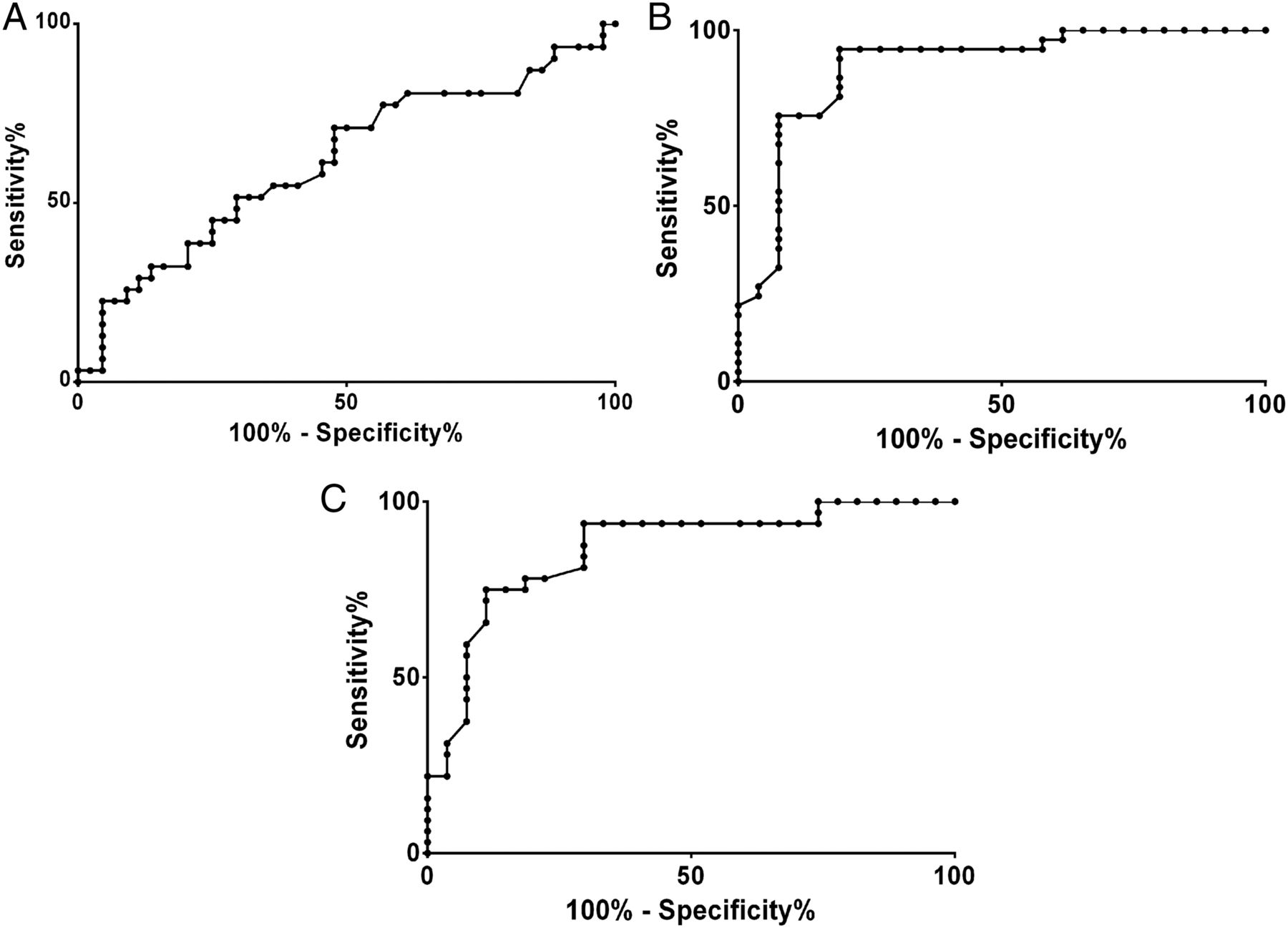
Seventy-seven participants were included in the study, of whom 74 completed the investigations (see online supplementary data for consort diagram). Demographic details are shown in table 1. A diagnosis of asthma was made in 28 out of 74 subjects (38%). Of these, 10 were diagnosed by reversibility criteria alone and 12 were diagnosed by PC20 alone, with 6 being positive on both investigations. The ROC curve to assess the utility of baseline FENO level as a diagnostic test for asthma had an area under the curve (AUC) of 0.62 (p=0.09) (figure 1).
Demographics and clinical characteristics of subjects with and without asthma

{kind=link}
(A) Receiver operator characteristic (ROC) curve analysis showing the sensitivity (%) and 100% specificity of FENO levels for asthma diagnosis. (B) ROC curve analysis showing the sensitivity (%) and the 100% specificity of FENO levels for predicting inhaled corticosteroids (ICS) response after 4 weeks of ICS treatment. (C) ROC curve analysis showing the sensitivity (%) and the 100% specificity of FENO levels for predicting ICS response after 12 weeks of ICS treatment.
A response to ICS was seen in 27 out of 67 subjects (40%) after 4 weeks and 28 out of 60 subjects (47%) after 12 weeks. Of the 28 subjects with asthma, 16 (57%) had a response to ICS after 4 weeks, with 12 of them having sustained this response after 12 weeks. Of the non-asthmatic subjects, 11 also demonstrated a response to ICS after 4 weeks. The ROC curve for baseline FENO level as a predictor of ICS response after 4 weeks had an AUC of 0.89 (p<0.0001) (figure 1). The optimal FENO cut-off point for predicting non-response to ICS was <27 ppb (negative predictive value 93%) and for predicting response was >33 ppb (positive predictive value 92%). FEV1, PC20 and blood eosinophil count did not perform as well as predictors of ICS response with AUCs between 0.32 and 0.67 (see online supplementary data).
The ability of FENO level to predict steroid response after 12 weeks was consistent with response at 4 weeks (ROC AUC=0.86 p<0.0001) (figure 1).
Discussion
Our results suggest that FENO measurement in people presenting to primary care with symptoms suggestive of asthma is more useful at predicting response to ICS than diagnosing asthma. Although our cohort was relatively small we feel our results demonstrate that using FENO to diagnose asthma needs further investigation before being recommended in guidelines.
The poor sensitivity and specificity of FENO in diagnosing asthma may be due to the heterogeneity of the condition with different inflammatory subtypes expressing high or low levels of TH2 inflammation.5 Hence the true utility of this test may be in detecting the presence of underlying TH2 inflammation to guide appropriate treatment with ICS, as also suggested previously by Smith et al.8 The finding that only 57% of subjects with confirmed asthma responded to ICS further highlights the limitations of this diagnostic label.
Our study was subject to several limitations including the lack of a formal measure of ICS adherence and the definition of asthma and ICS response. Defining asthma is notoriously problematic owing to the lack of a confirmatory gold standard; defining response to ICS is also difficult. Our chosen response criteria are likely to be ‘over-sensitive’ in detecting a response, but are therefore less likely to miss potential responders. We included a fall in FENO which is not used routinely but was frequently the only objective change in patients with a subjective improvement in cough and has the advantage of being easily performed in primary care. Also, it has previously been established that a reduction in TH2 inflammation is associated with a reduced risk of exacerbations,5 ,9 bringing some validity to this approach.
We propose that FENO measurement in patients with symptoms suggestive of airways disease could be used to identify patients in whom ICS response is highly unlikely. This could avoid unnecessary ICS treatment and encourage further investigation of the cause of the symptoms and, therefore, more effective treatment.
Footnotes
Twitter Follow Glenn Hearson at @NottinghamRRU
Contributors TWH had full access to all the data in the study, is the guarantor of the content of the manuscript, including the data and analysis, and takes responsibility for the integrity of the data and the accuracy of the data analysis, including any adverse effects. TWH, TMM and EW were co-applicants on the NIHR research for patient benefit grant. MJM, EW and WG-T contributed substantially to data collection. Sputum samples were processed by GM. MJM, EW, GH, TMM, DES and TWH contributed substantially to the study design, data analysis and interpretation and the writing of the manuscript.
Funding This paper summarises independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit Programme (Grant Reference Number PB-PG-1010-23145).
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Ethics approval National Research Ethics Committee East Midlands—Derby 1 (Ref 12/EM/0241).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves