Article Text

Statistics from Altmetric.com
Imaging and bronchoscopic findings
A 43-year-old woman presented with cough and gradually aggravating exertional dyspnoea of 5 months’ duration. She had undergone a hysteromyomectomy for myoma uteri 3 years previously. Chest CT revealed a tightly packed elongated endobronchial soft tissue mass completely obstructing the right intermediate bronchus and a solitary round nodule, 3.6 cm×2.6 cm in size, in the medial basal segment of right lower lobe (figure 1). Bronchoscopy demonstrated total occlusion of the right intermediate bronchus by a smooth and polypoid tumour (see figure 2 and online supplementary video). A biopsy from endobronchial tumour revealed uniform and dense proliferation of spindle tumour cells with round to oval nuclei, and immunohistochemistry showed that the tumour cells were negative for smooth muscle actin and positive for vimentin and CD10. Transvaginal ultrasonography showed that the uterus was 11.1 cm×7.9 cm×7.8 cm in size with two heterogeneous echogenic masses, 9.4 cm×4.4 cm and 4.5 cm×3.6 cm in size, respectively. The patient was diagnosed as having endobronchial metastasis from endometrial stromal sarcoma (ESS). The endobronchial mass was resected through snare electrocautery and cryotherapy during flexible bronchoscopy with resolution of the obstruction. Therefore, the patient's cough and dyspnoea disappeared.
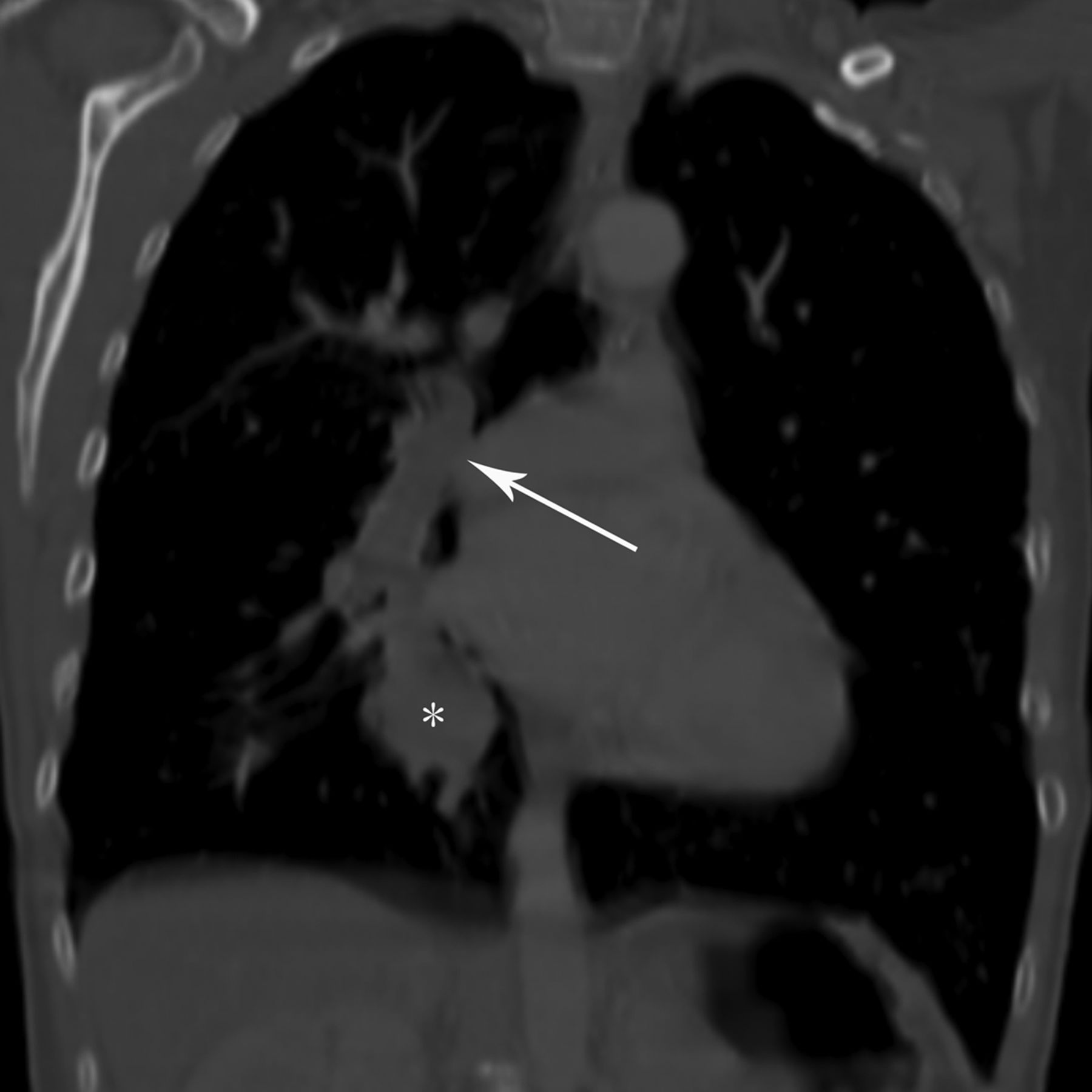
Contrast-enhanced CT of the chest shows a solitary mass completely obstructing the right intermediate bronchus (arrow) and a solitary round nodule in the medial basal segment of right lower lobe (*).

{kind=link}
{kind=link}
Bronchoscopy reveals a smooth and polypoid tumour completely obstructing the right intermediate bronchus.
ESS is an uncommon gynaecological malignancy, and it makes up an estimated 0.2% of all uterine cancers with an annual incidence of 1–2 per million women.1 The common metastatic sites are regional lymph nodes, and ESS occasionally metastasises to liver and lung.2 To the best of our knowledge, our patient is the first case of endobronchial metastasis from ESS. Consequently, our case reminds physicians to consider the possibility of endobronchial metastasis from uterine sarcoma. In our patient, the tumour has been a relatively slow process, and she remains almost asymptomatic after the interventional therapy, transcatheter arterial chemoembolisation and radiotherapy for endobronchial and pulmonary metastases from uterus.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online video
Footnotes
Contributors Conception and design: X-QX and YX, drafting the manuscript for important intellectual content: X-Q, Y-HL, Y-LL and X-WW.
Funding This work was supported by Science and Technology Program for Public Wellbeing of Yunnan Province (No. 2014RA020).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.