Article Text

Abstract
Background Community-acquired pneumonia (CAP) may be complicated by atrial fibrillation (AF) but the underlying mechanism is still unclear. Nox2-derived oxidative stress has been suggested to favour AF.
Methods We consecutively enrolled 432 patients hospitalised for CAP. Nox2 activity, as assessed by serum levels of soluble Nox2 (sNox2-dp), was evaluated in each CAP patient. A 12-lead electrocardiography was repeated every 24 h. All patients were followed up until discharge.
Results Forty-one patients with CAP (9.5%) experienced a new episode of AF within 24–72 h after hospital admission. Patients who experienced AF showed higher blood levels of sNox2-dp compared to those who did not (35.2±15.1 vs 27.0±12.5 pg/mL; p<0.001). Pneumonia Severity Index score (p=0.014), history of paroxysmal AF (p<0.001) and sNox2-dp (p=0.019) were independently associated with AF. At discharge, serum sNox2-dp levels were significantly decreased in the entire cohort (27.8±13.0 vs 21.9±6.8 pg/mL; p<0.001). Twenty-three out of 41 CAP patients with AF returned to sinus rhythm (56%); patients who remained in AF showed significantly higher baseline and discharge levels of sNox2-dp compared to those without AF (p<0.001) or with the 23 AF patients who returned to sinus rhythm (p<0.05). In vitro study showed that platelets or leucocytes incubated with endotoxin, at concentrations similar to those found in the circulation of CAP patients, elicited Nox2 up-regulation, suggesting endotoxin as a trigger of oxidative stress.
Conclusions AF may be detected in the early phase of CAP and is associated with Nox2 activation, suggesting a role for oxidative stress in promoting this cardiac arrhythmia.
Trial registration number NCT01773863.
- Pneumonia
- Oxidative Stress
Statistics from Altmetric.com
Key messages
What is the key question?
Atrial fibrillation (AF) may complicate community-acquired pneumonia (CAP), but the underlying mechanism is still unclear.
What is the bottom line?
AF may be detected in the early phase of CAP and is associated with Nox2 activation.
Why read on?
The study suggests that infection-mediated Nox2-derived oxidative stress promotes AF in patients with pneumonia.
Introduction
Community-acquired pneumonia (CAP) is the most common infection leading to hospitalisation in intensive care units and the most common cause of death associated with infectious diseases.1 Acute cardiovascular events complicating the clinical course of pneumonia may be one of the causes of poor survival. Thus, respiratory tract infection is associated with an increased risk for vascular events such as myocardial infarction and stroke, which usually occur in the early phase of pneumonia.2 ,3 In addition, pneumonia is complicated by atrial fibrillation (AF), which may be a serious complication as it is associated with enhanced risk of stroke and mortality.4 ,5 The mechanism accounting for the enhanced risk of AF in pneumonia has never been explored. However, a growing body of evidence suggests that oxidative stress is a trigger for AF.6 Studies in humans demonstrated oxidant species overproduction in patients with AF and accumulation of oxidant products such as nitrotyrosine in the atrial appendage of AF patients, suggesting a potential relationship between oxidative stress and AF perpetuation.7 ,8 Several enzymatic pathways producing reactive oxidant species (ROS) such as myeloperoxidase, uncoupling NO synthase and Nox2, are implicated in the pathogenesis of AF.6 Nox2, which is the most important cellular producer of ROS,9 seems to have a key role as documented in the setting of cardiac surgery, where patients experiencing post-surgery AF showed higher values of myocardium Nox2 compared to controls.8 ,10 Based on the hypothesis that Nox2 may predispose to AF in CAP, we investigated the relationship between Nox2 activity and AF occurrence in patients hospitalised for pneumonia. Moreover, in order to explore the mechanism of pneumonia-related oxidative stress, we performed in vitro experiments to investigate if endotoxin production could elicit oxidative stress via Nox2 up-regulation.
Methods
Patient selection
The study was conducted at four University-Hospital Policlinico Umberto I centres in Rome. All patients with CAP admitted to the four units through the emergency department from October 2011 to June 2014 were prospectively recruited and followed up. Inclusion criteria were: (1) age ≥18 years; (2) clinical presentation of an acute illness with one or more of the following signs or symptoms suggesting CAP: presence of rales, rhonchi, bronchial breath sounds, dullness, increased fremitus and egophony, fever (>38.0°C), tachycardia, chills, dyspnoea, coughing (productive or unproductive cough) and chest pain; and (3) presence of new consolidation(s) on chest X-ray. Pneumonia was considered as CAP if it was diagnosed upon hospitalisation and the patient had not been discharged from an acute care facility within 14 days preceding clinical presentation.
Patients were excluded from the study if any of the following criteria applied: pre-existing permanent or persistent AF, severe sepsis or immunosuppression (HIV infection, chemotherapy, high dose of immunosuppressive agents such as prednisone), presence of malignancy, pregnancy or breast feeding, or healthcare-associated pneumonia.11 Among 581 evaluated patients, 149 were excluded because of permanent or persistent AF (n=69), severe sepsis or immunosuppression (n=21), presence of malignancy (n=25), or healthcare-associated pneumonia (n=34). Thus, 432 patients were enrolled in the study.
This study was conducted according to the principles stated in the Declaration of Helsinki. The institutional review board approved this prospective, observational study, which was registered at ClinicalTrials.gov (Identifier: NCT01773863).
Baseline assessment
Data on demographic characteristics and comorbidities were collected. Severity of illness at presentation was quantified by the Pneumonia Severity Index (PSI), a validated prediction score for 30-day mortality in patients with CAP.12 Immediately after diagnosis of CAP, routine blood laboratory tests including serum high-sensitivity cardiac troponin T (hs-cTnT) and arterial blood gases were performed. Thereafter, serum hs-cTnT was repeated every 12 h and a 12-lead ECG was repeated every 24 h.
Type 2 diabetes mellitus (T2DM), hypertension, history of coronary heart disease (CHD), dyslipidemia and chronic obstructive pulmonary disease (COPD) were defined as previously described.13 ,14 Persistent, permanent and paroxysmal AF was defined as previously reported.15
The presence of AF was determined by two cardiologists (CC and AC) who did not participate in patient recruitment and follow-up and were unaware of patients’ clinical and laboratory characteristics.
Therapeutic treatment at admission and during the hospital stay was recorded.
Study end-points
The primary study endpoint was to assess serum levels of sNox2-dp, a marker of Nox2 activity,16 in CAP patients presenting a new episode of AF during their hospital stay.
Laboratory variables
After supine rest for at least 10 min, blood was withdrawn from the antecubital vein of patients in the fasting condition, mixed in a vacutainer (Vacutainer Systems, Plymouth, UK) with or without 17 IU/mL of lithium and immediately centrifuged for 20 min at 2000 rpm at room temperature. Plasma and serum samples were stored at −80°C until use.
Samples were taken within 48 h of hospital admission and at hospital discharge (approximately 10 days after hospital admission).
Serum hs-cTnT measurement
Hs-cTnT levels were measured with the Elecsys 2010 (Roche Diagnostics, Indianapolis, Indiana, USA) in a dedicated core laboratory. According to the manufacturer, the 99th percentile cut-off point for hs-cTnT is 0.014 µg/L, and a coefficient of variation of <10% is achieved at 0.013 µg/L.17
Serum Nox2 measurement
To evaluate Nox2 activity, we measured soluble Nox2 (sNox2-dp) levels in serum. Briefly, sNox2-dp was measured by ELISA as previously described.16 The peptide was recognised by a specific monoclonal antibody against the amino acidic sequence (224–268) of the extra membrane portion of Nox2. Values were expressed as pg/mL; intra-assay and inter-assay coefficients of variation were 5.2% and 6%, respectively.
Endotoxin serum levels
Endotoxin (lipopolysaccharide, LPS) plasma levels were measured by ELISA in 130 of the 432 CAP patients; this sample had demographic and clinical characteristics similar to those of the entire population. Briefly, 100 µL of serum sample was plated for 2 h at room temperature. After incubation, samples were read at 450 nm. Values were expressed as pg/mL; intra-assay and inter-assay coefficients of variation were 8% and 10%, respectively.
Cellular oxidative stress
Blood samples were collected from three healthy subjects (1 female and 2 males, aged 56.3±1.5 years), who had fasted for at least 12 h. To obtain platelet-rich plasma (PRP), blood samples were drawn mixed with Na citrate 3.8% (ratio 9:1) and centrifuged for 15 min at 180×g. To avoid leucocyte contamination, only the top 75% of the PRP was collected according to Pignatelli et al.18 PRP samples were pre-incubated with or without Toll-like receptors 4 (TLR4) blocking peptide (Santa Cruz Biotechnology; 0.4 µg/mL) and then treated with LPS from Escherichia coli 0111:B4 (100–300 pg/mL) for 10 min at room temperature; samples were then centrifuged for 3 min at 3000×g.
Polymorphonuclear leucocytes (PMNs) were isolated from the freshly drawn EDTA-blood of healthy subjects by dextran-enhanced sedimentation of red blood cells, Ficoll-Histopaque density centrifugation, lysis of remaining erythrocytes with distilled water and washing of cells with Hank's balanced salt solution (HBSS) in the absence of divalent cations. Finally, the cell pellet was suspended in 1 mL of HBSS at a final concentration of 1×106 cells/mL. PMNs were pre-incubated with or without TLR4 blocking peptide (Santa Cruz Biotechnology; 0.4 µg/mL) and then treated with LPS (100–300 pg/mL) for 10 min at room temperature; samples were then centrifuged for 3 min at 3000×g.
To measure ROS formation, cell suspensions were incubated with 2′,7′-dichlorofluorescin diacetate (DCF; 5 µM) for 15 min at 37°C. After incubation, platelets were stimulated with arachidonic acid (AA; 0.5 mM) or with LPS with or without TLR4; PMNs were incubated with phorbol 12-myristate 13-acetate (PMA; 10 µM) or with LPS with or without TLR4 for 10 min at room temperature. ROS production was expressed as a stimulation index (SI).
To evaluate Nox2 activity, the supernatant of agonists or LPS-treated cells was stored at −80° until use; sNox2-dp levels were measured as described above.
Statistical analysis
Categorical variables were reported as counts (percentage) and continuous variables were expressed as the mean±SD or median and IQR. Differences between percentages were assessed by the χ2 test or Fisher's exact test. Student's unpaired t test and ANOVA analysis were used for normally distributed continuous variables. Appropriate non-parametric tests (Mann–Whitney, Kruskal–Wallis tests and Spearman rank correlation test) were employed for all other variables.
The bivariate and multivariate effects of prognostic factors and treatments on the incidence of intra-hospital AF were assessed using logistic regression models. Wald CIs were obtained and tests for ORs and adjusted ORs were based on the estimated SEs. Our modelling strategy was mostly targeted at estimating the independent effect of sNox2-dp, adjusted for confounders and important risk factors. In addition to sNox2-dp, possible independent variables considered were: age, sex, PSI score, history of CHD or stroke, T2DM, hypertension, renal failure, COPD, history of paroxysmal AF, dyslipidemia, and use of statins, aspirin, ACE inhibitors and angiotensin receptor blockers (ARBs). Given the limited number of events, the relationship of interest has been adjusted for the three most relevant predetermined confounders, namely PSI, troponins and history of paroxysmal AF.
Only p values <0.05 were regarded as statistically significant. All tests were two-tailed and analyses were performed using the computer software packages IBM SPSS Statistics V.19.0 (IBM, Armonk, New York) and R V.2.15.2 (R Development Core Team, Vienna, Austria).
Sample size
The minimum sample size was calculated based on: (1) an expected rate of AF of 9%; (2) a relevant difference in sNox2-dp levels detected between groups (patients with or without AF) of |δ|≥7 pg/mL;19 (3) a standard deviation between groups of 9 pg/mL; and (4) a type-I error probability of α=0.05 and power 1−β=0.90. This resulted in a total of 389 patients.
Results
Nox2 activity in AF during hospitalisation and at discharge
During their hospital stay, 41 patients (9.5%) experienced a new episode of AF; the arrhythmia occurred in the early phase of hospitalisation, usually within 24–72 h of hospital admission. The clinical characteristics of patients with and without AF are summarised in table 1. Patients with AF were older and had a stronger history of stroke, CHD, hypertension, and paroxysmal atrial fibrillation (PAF). AF patients also showed higher levels of hs-cTnT and a higher PSI score. In addition, serum sNox2-dp levels were significantly higher in patients who experienced AF (table 1). Logistic regression analysis showed that PSI score, history of PAF and serum sNox2-dp were independently associated with AF after also adjusting for hs-cTnT (table 2).
Characteristics of the enrolled patients with CAP
Adjusted ORs of intra-hospital AF according to selected variables calculated by logistic regression analysis
Analyses of serum sNox2-dp were repeated at the end of hospitalisation (approximately 10 days after hospital admission). Compared to baseline values, serum sNox2-dp levels were significantly reduced (27.8±13.0 vs 21.9±6.8 pg/mL; p<0.001).
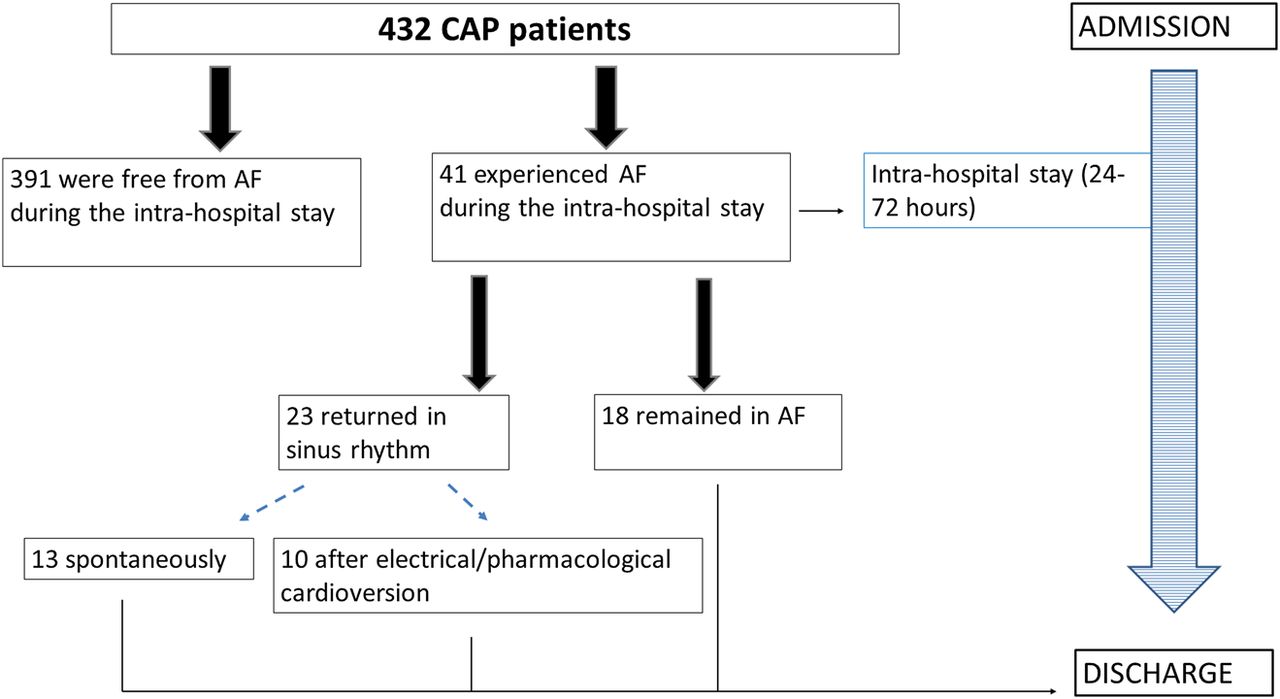
At discharge, 23 of the 41 AF patients were in sinus rhythm (13 spontaneously and 10 after electrical/pharmacological cardioversion), while 18 still had AF (figure 1). Patients who remained in AF at discharge showed the highest values of serum sNox2-dp both at baseline (p<0.001 vs patients without AF; p=0.035 vs patients with intra-hospital AF who returned to sinus rhythm; figure 2) and at discharge (p<0.001 vs patients without AF; p=0.019 vs patients with intra-hospital AF who returned to sinus rhythm). Conversely, no differences in serum sNox2-dp were found at discharge between patients who did not experience AF and patients who returned to sinus rhythm (figure 2).
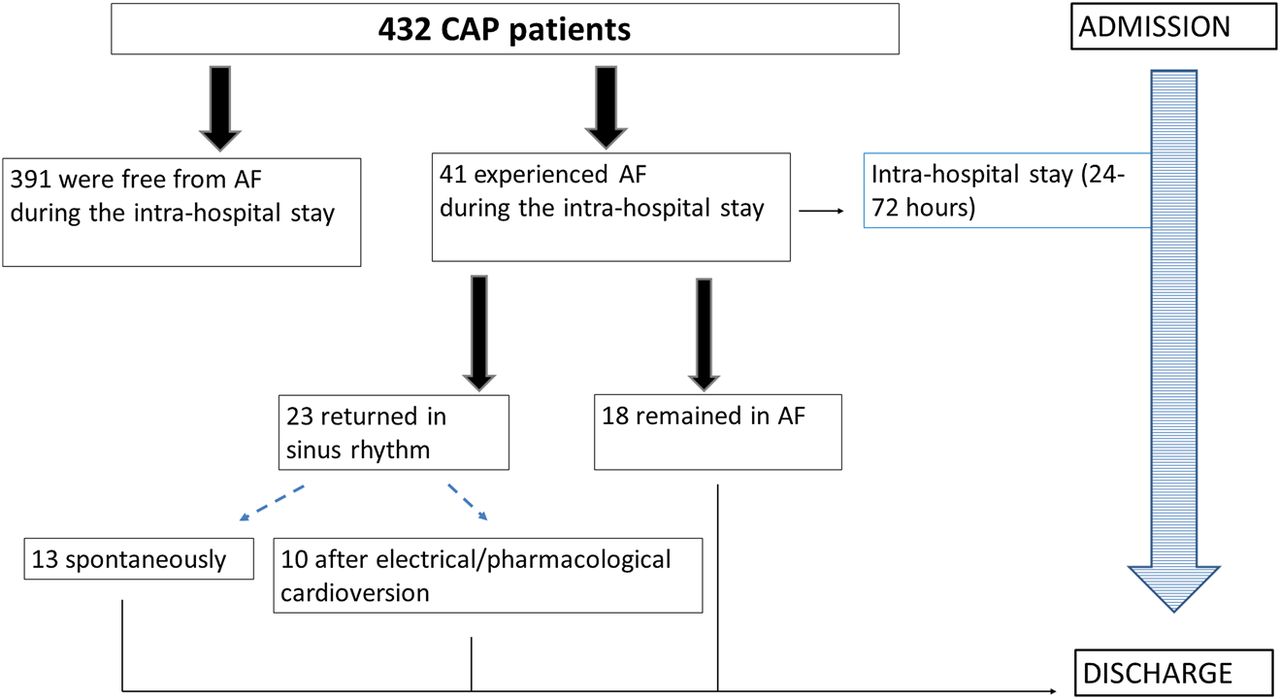
Study flow diagram. AF, atrial fibrillation; CAP, community-acquired pneumonia.
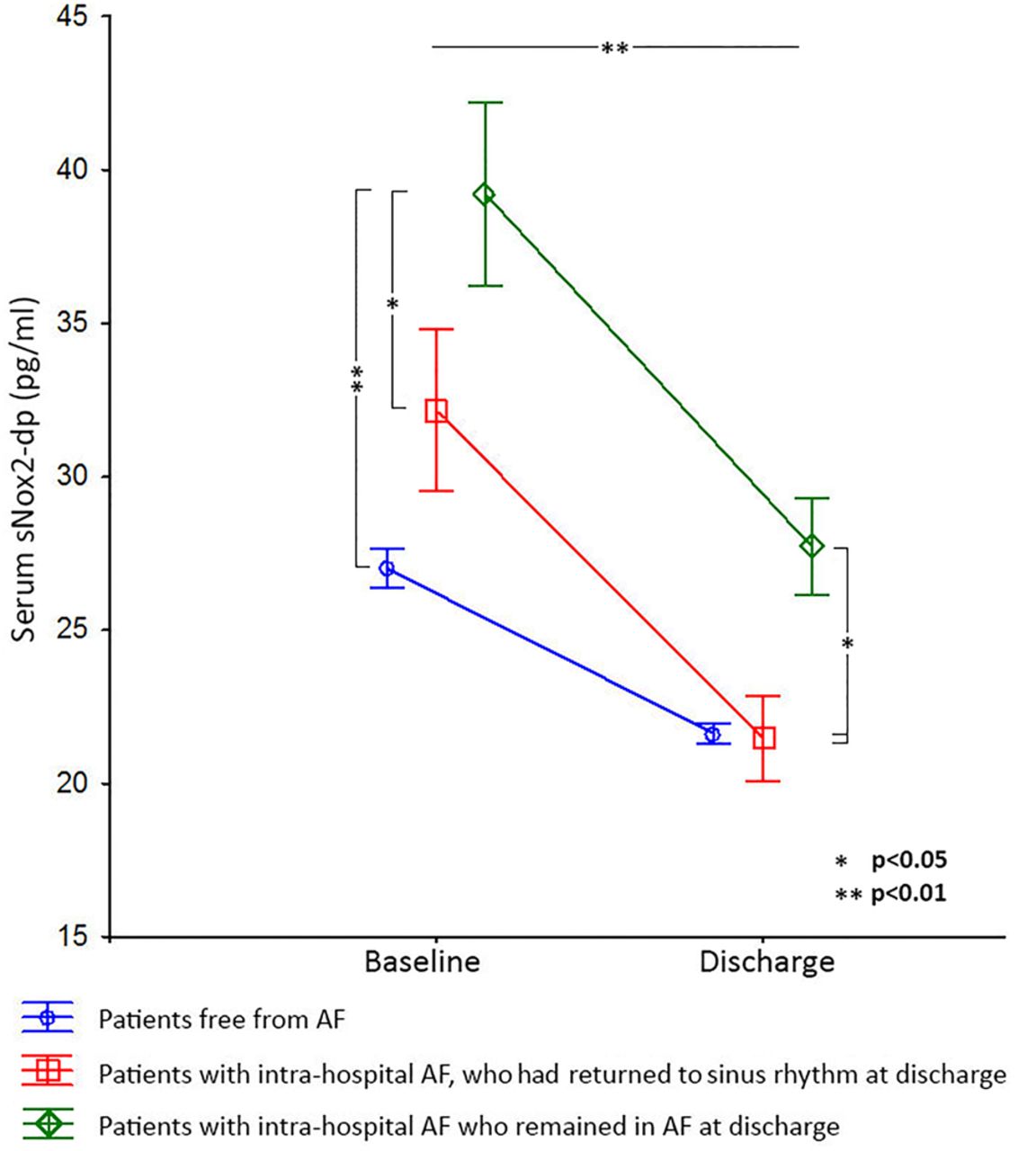
Baseline and discharge values of serum sNox2-dp according to the presence of atrial fibrillation during the hospital stay and at discharge. AF, atrial fibrillation.
Patients were likely to be treated with heparins during hospitalisation (table 3). However, no significant differences in serum sNox2-dp were found at discharge between patients who were treated or not treated with heparins (21.8±6.8 vs 22.3±6.9 pg/mL; p=0.651).
Patient treatment at admission and during their hospital stay
In vitro study
In vitro experiments were performed to investigate if endotoxin (LPS) was able to up-regulate cellular oxidative stress. In order to stimulate cells with a concentration of LPS similar to that detected in the blood of patients with CAP, we first measured the concentration range of endotoxin in 130 of the 432 CAP patients; this sample had demographic and clinical characteristics similar to those of the entire population (not shown). In this subset, new intra-hospital AF incidence (10%) overlapped that of the entire cohort. The median value of serum LPS was 234 (IQR: 154–384) pg/mL. Bivariate analysis showed a strong correlation between baseline values of serum sNox2-dp and LPS levels (Rs=0.784; p<0.001).
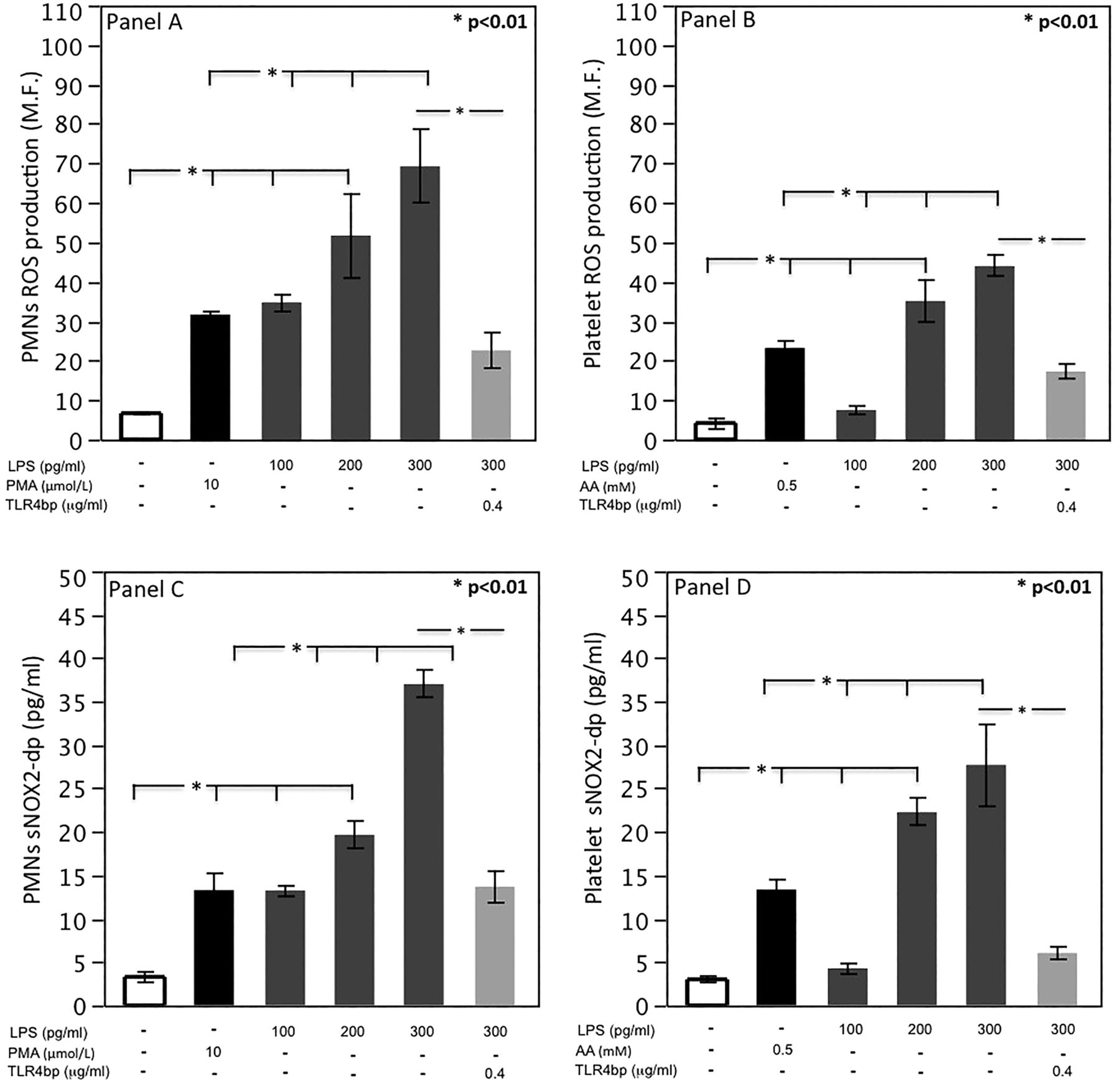
Using the same LPS concentration range as detected in the blood of CAP patients (100–300 pg/mL), we found that LPS increased ROS production and sNox2-dp activation of PMNs and platelets in a dose-dependent fashion compared to untreated cells (figure 3A–D). As LPS is known to stimulate cells via TLR4,20 we further verified the role of LPS in triggering cellular oxidative stress by incubating LPS-stimulated cells with a TLR4 inhibitor; in samples with the highest concentration of LPS, oxidative stress was blunted in PMNs and platelets incubated with TLR4 inhibitor (figure 3).

{kind=link}
{kind=link}
{kind=link}
Reactive oxidant species (ROS) production evaluated in polymorphonuclear leucocytes (PMNs) (A) and platelets (B) incubated with scalar concentrations of lipopolysaccharide (LPS) (100–300 pg/mL); sNox2-dp levels evaluated in PMNs (C) and platelets (D) incubated with scalar concentrations of LPS (100–300 pg/mL). AA, arachidonic acid.
Discussion
This study shows that in CAP patients AF occurs in the early phase of hospitalisation and is associated with the presence of endotoxin-mediated Nox2-dependent oxidative stress.
To the best of our knowledge, only one previous retrospective study analysed the incidence of AF in CAP patients and showed that about 10% of patients may experience this arrhythmia.5 Our report supports and extends this finding, confirming a similar incidence and underscoring that, as for myocardial infarction,21 such arrhythmia occurs essentially in the early phase of pneumonia and is observed mainly in patients with severe pneumonia. We also examined the behaviour of AF during pneumonia. Patients who experienced intra-hospital AF were older and had a stronger history of stroke and hypertension, thus suggesting that age and atherosclerotic burden may predispose to AF. Of note, more than 50% of patients who experienced AF returned to sinus rhythm spontaneously or after cardioversion, while the remainder showed persistent AF.
The fact that patients with a history of paroxysmal AF were at higher risk of experiencing AF during CAP is of particular interest, as it suggests that infections may represent a trigger for AF particularly in patients predisposed to AF. This finding help explain the results of Watanabe et al22 who, using 24 h Holter ECG, reported an increased incidence of paroxysmal AF episodes during the winter season when infections are more frequent. This association was corroborated by a study in a large US nationwide inpatient sample which reported more AF hospitalisations in winter months compared to summer months.23
Pneumonia per se may trigger AF as a consequence of direct myocardial damage; this is suggested by the higher blood levels of hs-cTnT in patients who experienced intra-hospital AF. In order to explore a possible mechanism accounting for the increased risk of AF in CAP, we focused on the potential role of oxidative stress as a trigger for AF.19 Previous studies have already documented a significant association between oxidative stress and AF, suggesting ROS have a potentially pathogenic role in eliciting this arrhythmia. In particular, Kim et al10 measured NADPH oxidase activity in the right atrial appendage of 170 patients undergoing coronary artery bypass surgery and found increased NADPH oxidase–ROS production in patients who developed AF after surgery, compared with those who remained in sinus rhythm. Furthermore, a meta-analysis on antioxidant use demonstrated their potential value in reducing AF risk.6 The present study reinforces this hypothesis by demonstrating that Nox2 was over-activated in the acute phase of CAP, particularly in patients who experienced AF. Of note, Nox2 activation was significantly decreased at discharge in patients who did not experience AF or who returned to sinus rhythm, while it remained elevated in those with persistent AF, suggesting a potential relationship between persistently elevated Nox2 activation and persistent AF.
A previous study from our group demonstrated that illness severity is a key factor for Nox2 up-regulation, suggesting that infection may favour cardiac involvement, but the underlying mechanism was not elucidated.24 In order to explore this issue, we hypothesised that endotoxin may directly elicit oxidative stress by up-regulating Nox2. Thus, we incubated PMNs and platelets with LPS concentrations similar to those found in the circulation of CAP patients and demonstrated that LPS alone was able to up-regulate Nox2 in a dose-dependent fashion and that this effect was blunted by blocking TLR4. This finding suggests that infection-related endotoxin causes oxidative stress via Nox2 up-regulation by a direct interaction between endotoxin and PMN or platelets via TLR4 receptors;20 this is in accordance with other studies showing Nox2 up-regulation by LPS.25
The study has implications and limitations. Patients with severe pneumonia or previous paroxysmal AF are at higher risk of AF and should be carefully monitored. AF occurs in the early phase of the disease, suggesting that infection may trigger AF via an endotoxin-mediated mechanism. Lack of Holter monitoring is a limitation of the study and, hence, we may have underestimated the real incidence of intra-hospital AF.
The precise pathway through which endotoxin-mediated Nox2 activation favours AF has not been investigated in the present study and needs to be further explored. Analysis of serum Nox2 maximally reflects the activity of Nox2 in blood cells,16 while no data are provided for Nox2 in other cells or tissue such as myocardium; therefore, we can only suppose but not prove that Nox2 is up-regulated by LPS in the myocardium of patients with CAP. Furthermore, we cannot exclude that other enzymes generating ROS such as myeloperoxidase or uncoupling NO synthase may also be implicated.6
In conclusion, in the early phase of disease, some patients with pneumonia experience AF, which persists in approximately 40% of cases. Patients with severe infection are at high risk and need to be carefully monitored. Nox2 up-regulation is associated with the occurrence of AF and endotoxin-mediated oxidative stress may be implicated in AF occurring during CAP.
References
Footnotes
Collaborators SIXTUS (thromboSIs-related eXTra-pulmonary oUtcomeS in pneumonia) study group: Simona Battaglia, MD, Giuliano Bertazzoni, MD, Elisa Biliotti, MD, Tommaso Bucci, MD, Cinzia Myriam Calabrese, MD, Marco Casciaro, MD, Andrea Celestini, MD, Paolo De Marzio, MD, Lucia Fazi, MD, Laura Giordo, Elisa Manzini, Sergio Morelli, MD, Daniele Pastori, MD, Pasquale Pignatelli, MD, Giulio Francesco Romiti, Elisabetta Rossi, MD, Eleonora Ruscio, Maria Gabriella Scarpellini, MD, Luisa Solimando, Filippo Toriello (Department of Internal Medicine and Medical Specialties, Sapienza University of Rome, Rome, Italy); Maurizio De Angelis, MD, Rozenn Esvan, MD, Lucia Fontanelli Sulekova, MD, Cristiana Franchi, MD, Stefania Grieco, MD, Marco Rivano Capparuccia, MD (Infectious and Tropical Diseases Unit, Department of Clinical Medicine, Sapienza University of Rome, Rome, Italy); Paolo Marinelli, MD, Michela Mordenti, MD, Paolo Palange, MD, Alessandro Russo, MD (Department of Public Health and Infectious Diseases, Sapienza University of Rome, Rome, Italy).
Contributors FV, RCan, CC, RCar: conception and design; the SIXTUS study group: acquisition of data; FV, RCan, RCar, CN, AF: analysis and interpretation of data; FV, RCan, CC, GT, MF, AF: drafting the manuscript or revising it for important intellectual content; all authors and the SIXTUS study group: final approval of the version to be published.
Funding This work was supported by a grant from Sapienza University of Rome (Progetto Universitario 2012, grant no. C26A12KWYB) to FV.
Competing interests None declared.
Ethics approval The institutional review board and ethics committee approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.