Article Text

Abstract
Background Treatment of pulmonary exacerbations (PEx) in cystic fibrosis (CF) varies widely with no consensus on management practices or best indicators of therapeutic success. To design trials evaluating PEx treatment factors, we characterise the heterogeneity of PEx care in adults and paediatrics, and correlate it with measures of clinical response including short-term and long-term lung function changes, change in symptom severity score and time to next intravenous antibiotic therapy.
Methods Data were used from a prospective observational study of patients with CF ≥10 years of age enrolled at six sites between 2007 and 2010. All were started on intravenous antibiotics for a clinically diagnosed PEx. Analysis of variance, logistic and Cox regression were used to examine the association of treatment factors with short-term and long-term clinical response.
Results Of 123 patients with CF (60% women, aged 23.1±10.2 years), 33% experienced <10% relative improvement in FEV1 during treatment, which was associated with failing to recover baseline lung function 3 months after treatment (OR=7.8, 95% CI 1.9 to 31.6, p=0.004) and a longer time to next intravenous antibiotic (HR=0.48, 95% CI 0.27 to 0.85, p=0.011). Symptom improvement was observed but was not associated with subsequent lung function or time to next antibiotic therapy, which had a median recurrence time of 143 days.
Conclusions Immediate symptomatic or respiratory response to PEx treatment did not have a clear relationship with subsequent outcomes such as lung function or intravenous antibiotic-free interval. These results can inform future research of treatment regimens for PEx in terms of interventions and outcome measures.
Trial registration NCT00788359 (www.clinicaltrials.gov).
- Cystic Fibrosis
Statistics from Altmetric.com
Key messages
What is the key question?
How do varying treatments for pulmonary exacerbation (PEx) in cystic fibrosis (CF) correspond with clinical response, including symptom severity, short-term and long-term lung function, and time to next PEx?
What is the bottom line?
Across multiple centres, the patient clinical characteristics and treatment factors that are associated with short-term clinical improvement differ from those associated with subsequent lung function recovery and time to next acute event treated with intravenous antibiotics.
Why read on?
This is the only multicentre evaluation of clinically defined PEx in both paediatric and adult CF patients to examine a comprehensive set of clinical responses for determining an outcome measure for future studies of exacerbation therapies.
Introduction
Infection, inflammation and structural damage of the lung are characteristic of cystic fibrosis (CF). Daily symptoms of chronic infection are punctuated with acute episodes of increased cough, fatigue, physical findings and other signs including rapid drop in lung function called a pulmonary exacerbation (PEx). Such events are associated with mortality,1 ,2 reduced quality of life,3 unrecoverable loss of lung function2 ,4 and increased healthcare costs.5 There were >15 000 PEx recorded in the CF Foundation (CFF) National Patient Registry (NPR) in 2012, affecting nearly 40% of patients with CF at least once.6 Treatment for PEx varies across patients and centres,7 but often includes a combination of intravenous, inhaled or oral antibiotics8 in conjunction with increased airway clearance therapy, inhaled mucolytics or corticosteroids. Location (inpatient or outpatient) and duration of therapy may differ by factors such as patient gender,9 ,10 age,11 PEx history, disease severity, microbiology, physician goals and patient preferences.12
Recent guidelines cite scarce evidence to support common treatment regimens for PEx management,13 highlighting the need for research in this area. While studies have examined different short-term14–16 and long-term4 ,17 ,18 outcomes of PEx, and factors associated with them, there is no consensus on the most relevant or useful measure of PEx management success or failure.
Physicians generally treat to alleviate signs and symptoms or recover lost lung function,19 but little is understood about the implications of failing to achieve those immediate goals in patients with CF. To inform clinical care and research aimed at improving PEx treatment regimens, we analysed data from a multicentre, prospective study of PEx to characterise the heterogeneity of treatment factors and correlate them with measures of clinical response, including symptom severity, short-term and long-term lung function, and time to next PEx. Specifically, we aimed to determine the association between immediate symptom and lung function response with subsequent need for intravenous antibiotics and ultimate pulmonary function recovery.
Materials and methods
Patients and study design
Patients with CF 10 years and older being started on two or more intravenous antibiotics for a clinically diagnosed PEx using criteria outlined by a CFF Consensus Conference20 were eligible to enrol in the observational study conducted at six adult and paediatric CF centres between 2007 and 2010.21 Study protocol encouraged at least 10 days of antibiotic administration and mucus clearance in accordance with CF Care Guidelines,13 but all other treating factors, including location, concomitant administration of inhaled or oral antibiotics or systemic steroids, were at physician's discretion. Spirometry22 and sputum cultures were performed at time of enrolment (within 24 h of intravenous initiation) and approximately 10–14 days later. (FEV1) per cent predicted of normal was calculated.23 ,24 Participants completed the CF Respiratory Symptom Diary (CFRSD)25 for each day up to 21 days.
Variables and outcomes
The diagnosis of PEx was made by clinician but verified with a scoring algorithm (score excluding change in FEV1 at admission ≥2.6).26 Short-term outcomes are those that occur during treatment of the PEx or within 30 days of completion: lung function non-response to treatment was categorised as <10% relative improvement in FEV1 (L) from enrolment visit (intravenous antibiotic initiation) to follow-up visit 10–14 days later—within 10 days of end of intravenous therapy. This represents ‘immediate response’11 regardless of a patient's ‘baseline’ or ‘sick decline’, and is calculated as a relative change to account for FEV1 at the time of admission. The Chronic Respiratory Infection Symptom Score was applied to the CFRSD to calculate a severity score from 0 to 100 (100 being most severe).27 Change in symptom score was calculated from enrolment visit to end of intravenous therapy or last completed CFRSD (up to 21 days after intravenous initiation), whichever came first.
Study data were merged with CFFNPR to determine other clinical factors including: CF-related diabetes (CFRD), respiratory microbiology, best FEV1 per cent predicted in the preceding 6 months and history of intravenous antibiotic episodes in the preceding 6 months. Interim clinical outcomes (those occurring within 3 months of PEx treatment completion) and long-term outcomes (those occurring >3 months after intravenous treatment) were also obtained from the CFFNPR. Best FEV1 per cent predicted in the 3 months following study PEx treatment was ascertained to determine 90% recovery of best FEV1 from 6 months prior4 and represents ‘baseline recovery’. Time to next intravenous antibiotic episode (initiated ≥7 days after end of intravenous therapy for study PEx) was calculated and censored at the time of last encounter.
Statistical analyses
Summaries including mean and SD are reported for treatment factors and clinical outcomes by age group (<18 or ≥18 years), t tests and Fisher's exact test compare age groups. Analysis of variance, logistic and Cox regression were used to explore the association of clinical characteristics and treatment factors with symptom response and FEV1 change <10% during intravenous antibiotic treatment, recovery of pre-PEx FEV14 and time to next intravenous antibiotic episode. Backward selection with significance level 0.30 to remain in model was applied to eliminate covariates from the full model, which included women, age ≥18 years, CFRD, Pseudomonas aeruginosa-positive, methicillin-resistant Staphylococcus aureus (MRSA)-positive, FEV1 per cent predicted <50% at PEx start, 10% drop in FEV1 per cent predicted at initiation of study PEx treatment (‘sick decline’), steroid use, oral or inhaled antibiotic use for PEx treatment, MRSA active drug for PEx treatment (doxycycline, linezolid, minocycline, rifampin, tigecycline, vancomycin or trimethoprim/sulfamethoxazole), duration of intravenous antibiotics (<10 days, 10–14 days or >14 days) and history of intravenous antibiotics in the preceding 6 months. A relaxed 0.30 criterion was used to allow non-significant covariates in the model that stabilise estimates of other parameters.28 Immediate lung function non-response (<10% relative improvement in FEV1 (L) during treatment) and change in symptom score27 were then added to the models for (1) failure to recover baseline FEV1 (2) time to next intravenous antibiotic. Model coefficient estimates including OR and HRs are reported with 95% CIs. Reported p values are two-sided and considered exploratory; no adjustments were made for multiple comparisons. No sample size estimates were performed. Analyses were performed using SAS (V.9.2, SAS Institute, Cary, North Carolina, USA, 2009), and R (V.2.15, The R Foundation for Statistical Computing, Vienna, Austria, 2012).
Results
A total of 123 patients with CF (60.2% women) were treated with intravenous antibiotics for a diagnosed PEx (table 1). Average age was 23.1 years (SD=10.2) and FEV1 per cent predicted (%) at admission was 55.8% (SD=20.9). Patients with paediatrics (10–17 years old) made up 35% (n=43) of the cohort, and best FEV1 in 6 months prior was on average (SD) 83.1% (18.3) in children and 53.2% (19.7) in adults. P. aeruginosa was more prevalent in adults (75.0% vs 44.2%, p=0.001), while methicillin-sensitive Staphylococcus aureus (MSSA) (28.8% vs 27.9%, p=0.9) and MRSA (28.8% vs 39.5%, p=0.23) were similar in adults and children.
Demographics and baseline characteristics
PEx treatment
PEx treatment features are in table 2 by age. None of the patients with paediatrics were treated exclusively at home, and adults were treated on average 4.2 days longer than those under 18 years (95% CI 1.5 to 6.9, p=0.003). Intravenous tobramycin was the most commonly prescribed antibiotic in combination; paediatric patients were more likely to get a MRSA active antibiotic (65.1% vs 45.0%, p=0.039), and 16.3% overall received systemic corticosteroids.
Pulmonary exacerbation treatment by age group
PEx outcomes
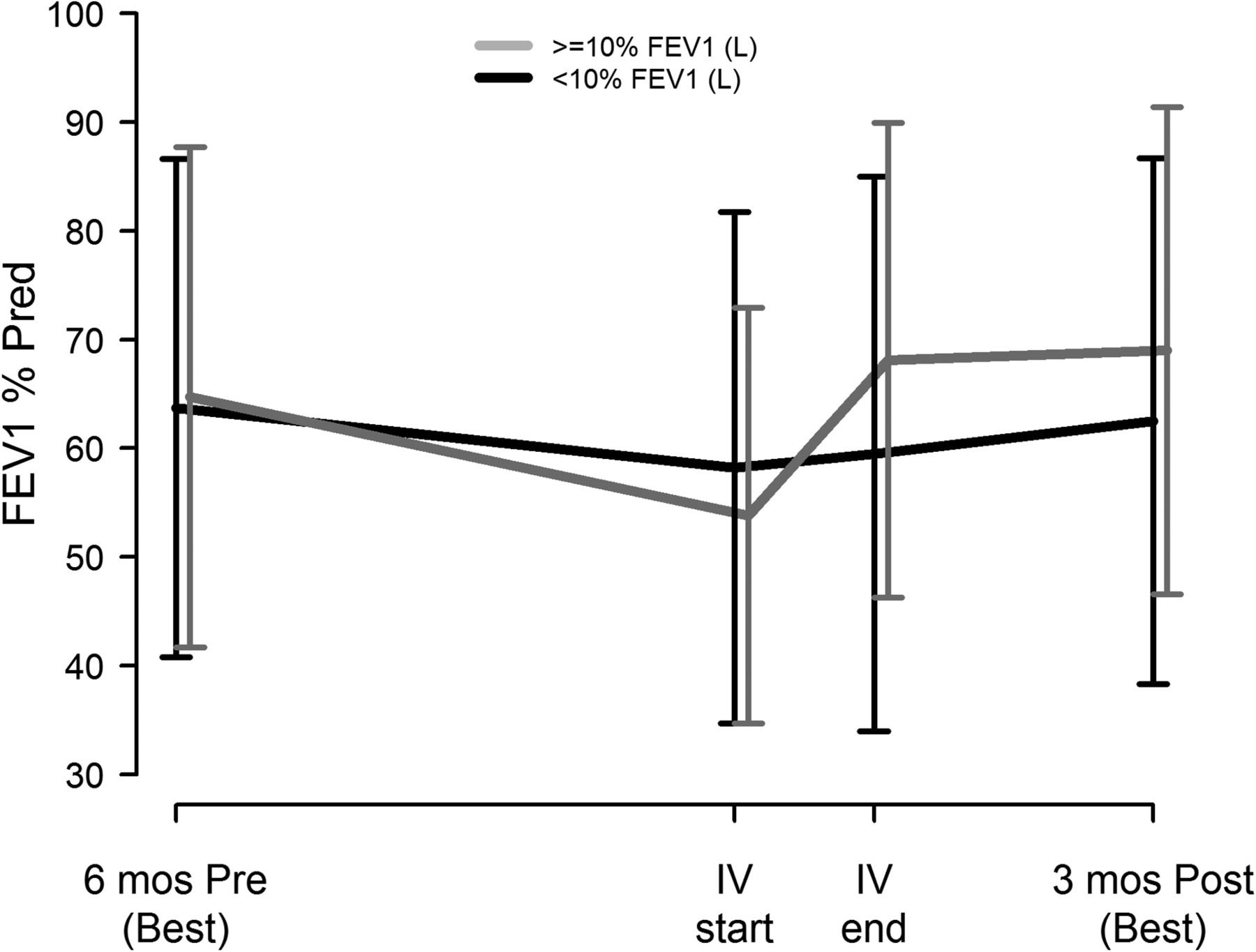
Online supplementary figure S1 shows enrolment and follow-up for each of the outcomes. Table 3 summarises short-term and long-term clinical outcomes by age group. Among the 102 participants with spirometry at enrolment and at or near the end of intravenous antibiotic treatment, 73% had lung function measured within ±2 days of intravenous end, 93% were within a week; two had PFTs not within 10 days of intravenous end and were removed from the calculations. There was marked improvement in immediate FEV1 response in the younger patients (5.9% predicted more than adults, 95% CI 2.3 to 9.5, p=0.002) (figure 1), while both age groups had similar response in symptom severity, baseline FEV1 recovery in subsequent 3 months and intravenous antibiotic need (by 30, 90 and 180 days) after treatment for study PEx. The Kaplan–Meier curves (figure 2) for time to next intravenous antibiotic did not significantly differ by age group (p =0.74).
Clinical response by age group and overall

Lung function by age group. FEV1% of predicted mean±1SD for paediatric participants (black lines, n=37) and adult participants (gray lines, n=71): best during 6 months (mos) before study pulmonary exacerbations (PEx), at time of intravenous (IV) initiation for PEx, at end of intravenous for PEx and best during 3 months after study PEx.
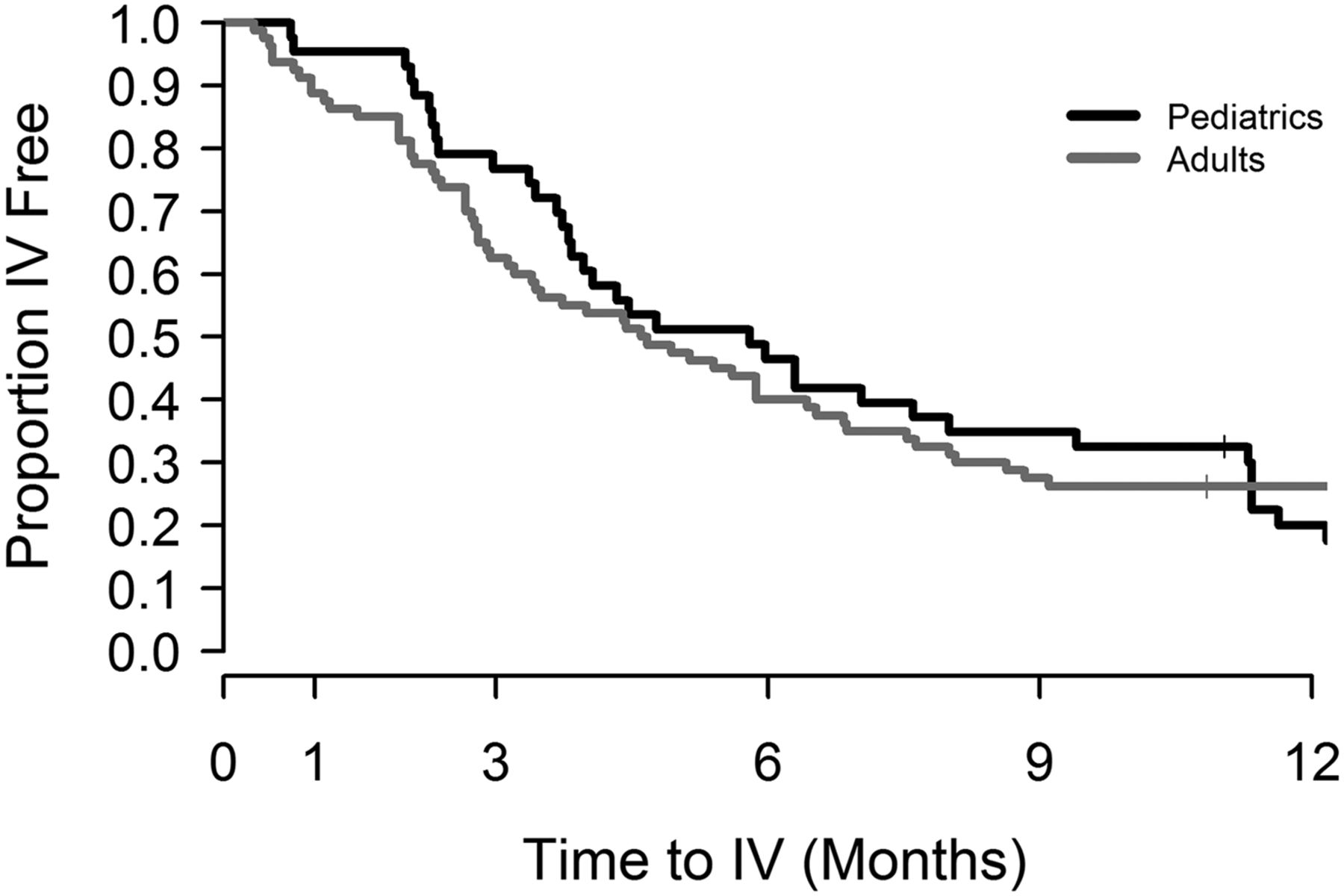
Kaplan–Meier survival curves for time to next intravenous antibiotic episode by age group. Proportion intravenous antibiotic free by time (after study pulmonary exacerbations) in paediatric (black lines, n=43) and adult participants (gray lines, n=80).
Association of demographic, clinical and treatment factors with outcomes
Figure 3 shows the association of clinical and treatment factors with each of the clinical responses (p<0.30). MRSA was associated with a diminished symptom severity reduction (average 8.8 point increase, 95% CI 1.8 to 15.8, p=0.015), while treatment choices such as steroids (−12.0 points, 95% CI −19.7 to −4.3, p value=0.003), oral/inhaled antibiotics and MRSA active drugs were associated with larger reductions in symptom severity. Longer treatment durations (10–14 days and >14 days as compared to <10 days) were associated with less symptom improvement but not statistically significant.

Factors associated with short-term and long-term outcomes of pulmonary exacerbations (PEx) treatment. (A) Multivariate regression coefficients (Reg. Coeff) and 95% CIs for demographic (DEMOG), clinical (CLIN) and treatment (TRT) factors associated with Chronic Respiratory Infection Symptom Score (CRISS) symptom score (– is an improvement). (B) Multivariate ORs and 95% CIs for factors associated with <10% immediate response in FEV1 (L) during treatment. (C) Multivariate ORs and 95% CIs for factors associated with <90% baseline (Base.) FEV1 recovery. (D) Multivariate HRs and 95% CIs for factors associated with time to next intravenous antibiotic (abx). Factors with p <0.30 were dropped from model and not estimated or plotted in figure. Base FEV (<50%), FEV1 per cent predicted at time of PEx; CFRD, cystic fibrosis-related diabetes; FEV1 Drop, FEV1 drop ≥10% presenting for PEx; MRSA, methicillin-resistant Staphylococcus aureus colonised at time of PEx; MRSA active drug, use of doxycycline, linezolid, minocycline, rifampin, tigecycline, vancomycin or trimethoprim/sulfamethoxazole; Oral or Inh, use of oral or inhaled antibiotics during treatment for PEx; Pa=P. aeruginosa colonised at time of PEx; 10–14 days, total duration of intravenous antibiotic therapy compared with reference <10 days; >14 days, total duration of intravenous antibiotic therapy compared with reference <10 days.
Immediate FEV1 non-response was associated with use of oral/inhaled antibiotics (OR=3.5, 95% CI 1.2 to 10.6, p=0.027) and longer treatment duration (>14 days compared with <10 days, p=0.021), whereas a drop of 10% FEV1 at admission had a protective effect and was associated with a reduced odds of failure to recover (OR=0.30, 95% CI 0.11 to 0.81, p =0.017). CFRD was the only covariate with a common, though weak, association with both immediate FEV1 response (p=0.221) and recovery of baseline FEV1 (p=0.257). History of intravenous antibiotics was the only factor significantly associated (OR=4.8, 95% CI 1.2 to 18.4, p=0.023) with non-recovery of baseline FEV1 post treatment.
The hazard of subsequent intravenous antibiotic was significantly increased by history of intravenous episodes (HR=2.7, 95% CI 1.8 to 4.1, p<0.001) and low FEV1 at admission (HR=2.4, 95% CI 1.5 to 3.9, p<0.001), whereas longer treatment duration was associated with a reduced time to next exacerbation (10–14 days: HR=0.50, 95% CI 0.29 to 0.889, p=0.018; >14 days: HR=0.38, 95% CI 0.20 to 0.70, p =0.002).
Short-term response and subsequent outcomes
Change in symptom score was not associated with recovery of baseline lung function (p=0.49) or time to next intravenous antibiotic (p=0.69) when added to the multivariate logistic and Cox regression models presented in figure 3 and online supplementary table S1, respectively. Immediate non-response in FEV1 (<10% during treatment) significantly increased the odds of non-recovery of baseline (OR=7.8, 95% CI 1.9 to 31.6, p=0.004); no other covariates were significantly associated with post-PEx recovery when adjusted for short-term FEV1 response. Among those with immediate FEV1 response, 95% recovered baseline by 3 months, whereas among those who had <10% improvement during treatment, 73% recovered baseline. Figure 4 shows lung function by short-term FEV1 responder status.

Lung function by immediate FEV1 response with treatment. FEV1% of predicted mean±1 SD for participants with <10% relative FEV1 (L) response during pulmonary exacerbations (PEx) treatment (black lines, n=35) and participants ≥10% relative FEV1 (L) response during treatment (gray lines, n=67): best during 6 months (mos) before study PEx, at time of intravenous (IV) initiation for PEx, at end of intravenous for PEx and best during 3 months after study PEx.
In contradiction, short-term FEV1 non-response significantly decreased the risk of subsequent intravenous antibiotic event (HR=0.48, 95% CI 0.27 to 0.85, p=0.011) along with other significant factors that increased the risk: being a woman (HR=1.8, 95% CI 1.1 to 3.1, p=0.032), history of intravenous antibiotic event (HR=2.8, 95% CI 1.6 to 4.8, p<0.001) and low FEV1 at start of study PEx (HR=2.0, 95% CI 1.2 to 3.4, p=0.01). Figure 5 shows the Kaplan–Meier curves to next intravenous antibiotic episode by short-term FEV1 responder status (p=0.07).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curves for time to next intravenous (IV) antibiotic episode by immediate FEV1 response with treatment. Proportion intravenous antibiotic free by time (after study pulmonary exacerbations (PEx)) in participants with <10% relative FEV1 (L) response during PEx treatment (black lines, n=35) and those with ≥10% relative FEV1 (L) response during treatment (gray lines, n=67).
Discussion
CF PEx are managed with a wide array of treatment regimens that may be based on patient or clinician preference, pathogen isolation, historical response or trajectory of response to treatment for the current PEx. In general, the short-term goals of treatment are to resolve symptoms and recover lost lung function, but there may also be long-term goals, such as preservation of lung function and prevention of subsequent acute events. We show, across multiple centres, that patient clinical characteristics and treatment factors that were associated with short-term clinical improvement differed from those associated with subsequent lung function recovery and time to next acute event treated with intravenous antibiotics. In addition, immediate symptom resolution and lung function response did not have a clear relationship with longer term clinical outcomes.
To our knowledge, this is the first study to examine the multifactorial association between clinical and treatment features with patient-reported symptoms during a PEx. Improvement (ie, reduction in symptom score) was seen in nearly all patients; however, presence of MRSA was related to a diminished effect while steroids were significantly associated with a greater effect. This is contrary to a small randomised trial of steroids in children with CF that failed to see an effect of steroids on symptoms.29 Treating to improve patient signs and symptoms is a hallmark component of PEx management; however, it may not be indicative of downstream clinical outcomes. A CF symptom score during PEx30 has been associated with extending intravenous antibiotic duration17 and time to next PEx,31 but not when adjusting for other factors—similar to the findings of this study. The antibiotic course may be extended because of seeming lack of symptom improvement, but it is unclear if there are advantages to longer treatment that outweigh cost, time and potential toxicities.
The other common goal of PEx treatment is recovery of lost lung function. Nearly 90% of this sample recovered baseline lung function—higher than the 75% observed in the Registry from 2003 to 2006.4 We found that failure to improve FEV1 during treatment was associated with failure to recover pre-PEx lung function in the subsequent 3 months; however, in contradiction, short-term FEV1 non-response was associated with longer time to next intravenous antibiotic episode. Perhaps the patients with the highly variable, oscillating swings in lung function–large drops and big gains with treatment are easier to identify as requiring treatment for exacerbation,32 while those who are less responsive to intravenous antibiotics may be less likely to be admitted again for intravenous treatment when it did not appear to improve the patient's lung function. This analysis specifically examined the association of relative FEV1 improvement during treatment for PEx and subsequent ‘baseline recovery’ while adjusting for ‘sick decline’ and lung function at admission. An alternative short-term metric would be recovery of baseline lung function (best 6 months prior) at the end of treatment; however, such a measure would confound ‘sick decline’ rather than letting the analysis tease out any effect. Also, the calculation of baseline recovery includes the FEV1 measured at end of treatment (which is often the highest in the 3 months post-intravenous therapy); these measures of ‘immediate response’ and ‘recovery of baseline’ guaranteed mutually exclusive endpoints.
Extending the PEx-free interval is an important feature of CF disease management because these acute events have been shown to have long-term detrimental effects.1 ,18 ,33 For this reason, time to next intravenous antibiotic course or PEx is a common and useful endpoint in clinical trials of chronic therapies34 ,35; however, it could be argued that because the majority of these events occur 4–6 months after treatment, they are too far downstream and confounded by factors not related to the acute management of the preceding PEx to serve as useful outcomes when studying success or failure PEx treatment regimens. Similarly, long-term lung function decline has been explored within the context of PEx; however, for studying PEx treatment regimens, an immediate outcome is necessary for both practicality and to reduce the influence of confounding factors. Several studies have shown the detrimental effect of exacerbation on long-term lung function in CF.4 ,18 These study data support those findings (history of intravenous antibiotics significantly increased the risk of failing to recover baseline lung function) and likely demonstrate that recurrent PEx events and underlying phenotype such as CFRD and MRSA colonisation are responsible for persistent respiratory decline more than a particular treatment regimen or response.
The inclusion criteria of this study required dual systemic, intravenous antibiotic therapy and thus likely excluded patients treated solely for MRSA infection (either because of exclusively oral or mono-therapeutic choices). Thereby, inference here applies only to CF exacerbations that required systemic dual therapy. The PEx guidelines found insufficient evidence to necessitate two antibiotics when P. aeruginosa is suspected, but neither was there support for less than two, and thus yielded to standard practice of two.13 P. aeruginosa prevalence in this study is consistent with the general CF population.6 PEx treatment guidelines also cited insufficient evidence of either benefit or harm from acute steroid use to treat CF exacerbations.13 While this study found some moderate benefit from steroid use, interpretations should be exercised with caution because of the potential for indication bias in a non-randomised study. The question of acute corticosteroids for treating CF PEx is of tremendous interest and would benefit from carefully controlled, randomised research.
There were limitations to our analysis of this observational study, one being that treatments may have been proxy for baseline clinical features or confounded with response. For example, duration was a treatment factor in this analysis; however, antibiotic regimens often changed and extended mid-course presumably for reasons of clinical non-response, therefore treatment was confounded with outcomes and has been treated as such in other studies.15 ,17 Additions or changes to the treatment may have been related to microbial susceptibility testing or convenience/preference. For these reasons, it is challenging to interpret the relationship between treatment factors and outcomes. This multisite paediatric and adult study augmented with CF NPR data yields generalisable findings for short-term and long-term PEx outcomes—perhaps at the expense of increased heterogeneity resulting from site variability, irregular spirometry timing and unmonitored supplemental data. Lastly, all our statistical models were estimable and coefficients were stable; however, the sample size is moderately small and no adjustments were made for multiple comparisons, therefore associations and p values should be interpreted with caution.
Symptom resolution and immediate improvement in FEV1 are meaningful measures of acute PEx therapy, and we show them to be more associated with treatment features than long-term measures. Short-term non-response in symptoms or lung function during treatment was not clearly related with subsequent PEx; however, immediate FEV1 response does appear to be associated with recovery of baseline lung function. Also, some of the contradictory results we observed support the use of a composite response15 of short-term clinical features to serve as a trial outcome (eg, lung function or symptom improvement without additional intravenous antibiotics within a month of the initial treatment). A larger cohort may support or refute our results, while randomised controlled studies of PEx treatment will ultimately produce the evidence necessary to improve the overall well-being of patients with CF.
Acknowledgments
We would like to thank the Cystic Fibrosis Foundation for the use of CF Foundation Patient Registry data. Additionally, we would like to thank the patients, care providers and clinic coordinators at CF Centers throughout the USA for their contributions. We also recognise the three anonymous peer reviewers whose suggestions greatly improved this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Correction notice This article has been corrected since it was published Online First. The provenance and peer review statement has been corrected.
Contributors SLH, SDS and PAF designed the study, SLH, VT, SDS, CHG, DBS, BCM and PAF contributed substantially to the data analysis and interpretation, and the writing of the manuscript.
Funding This research was supported by Cystic Fibrosis Foundation Therapeutics (SAGEL07B0, SAGEL11CS0, HAMBLE10A0, HELTSH13A0), the National Institutes of Health (NIDDK P30 DK089507, KL2 TR000428), the SCTR Institute at the Medical University of South Carolina (NIH UL1 TR000062), NCATS Colorado CTSI (NIH UL1 TR000154) and the University of Wisconsin-Madison ICTR (NIH UL1 TR000427).
Competing interests None declared.
Patient consent Obtained
Ethics approval All participating site Institutional Review Boards and the primary site of analysis: Seattle Children's Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Study data can be requested through SDS or the Cystic Fibrosis Foundation Therapeutics Development Network.