Article Text

Abstract
Background There is limited data on the risk factors and phenotypical characteristics associated with spirometrically confirmed COPD in never-smokers in the general population.
Aims To compare the characteristics associated with COPD by gender and by severity of airway obstruction in never-smokers and in ever-smokers.
Method We analysed the data from 5176 adults aged 40 years and older who participated in the initial cross-sectional phase of the population-based, prospective, multisite Canadian Cohort of Obstructive Lung Disease study. Never-smokers were defined as those with a lifetime exposure of <1/20 pack year. Logistic regressions were constructed to evaluate associations for ‘mild’ and ‘moderate-severe’ COPD defined by FEV1/FVC <5th centile (lower limits of normal). Analyses were performed using SAS V.9.1 (SAS Institute, Cary, North Carolina, USA).
Results The prevalence of COPD (FEV1/FVC<lower limits of normal) in never-smokers was 6.4%, constituting 27% of all COPD subjects. The common independent predictors of COPD in never-smokers and ever-smokers were older age, self reported asthma and lower education. In never-smokers a history of hospitalisation in childhood for respiratory illness was discriminative, while exposure to passive smoke and biomass fuel for heating were discriminative for women. COPD in never-smokers and ever-smokers was characterised by increased respiratory symptoms, ‘respiratory exacerbation’ events and increased residual volume/total lung capacity, but only smokers had reduced DLCO/Va and emphysema on chest CT scans.
Conclusions The study confirmed the substantial burden of COPD among never-smokers, defined the common and gender-specific risk factors for COPD in never-smokers and provided early insight into potential phenotypical differences in COPD between lifelong never-smokers and ever-smokers.
Trial registration number NCT00920348 (ClinicalTrials.gov); study ID number: IRO-93326.
- Clinical Epidemiology
- COPD epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
What are the clinical characteristics and associated factors for COPD in never-smokers in the general population and are they different from those of COPD in ever-smokers?
What is the bottom line?
The results clearly showed that the COPD in never-smokers forms a substantial burden in the population; that there are gender-specific differences in never smokers with COPD and that there are physiological and radiographic differences between COPD in never-smokers compared with that in ever-smokers.
Why read on?
The study highlights the substantial burden of COPD among never-smokers and provides additional data on the sex differences profiling never-smokers COPD and early insight into phenotypical differences for COPD in lifelong never-smokers and ever-smokers.
Introduction
The occurrence of COPD in never-smokers is not widely appreciated, despite the fact that the relative burden of COPD in never-smokers is high in developing1 and developed countries,2 accounting for about 30%3–7 of all COPD in the community.
There is limited information on the risk factors associated with spirometrically confirmed COPD in never-smokers in the general population.5 ,8 ,9 and more data from population-based studies are needed.10
Risk factor exposures may differ between sexes.11 In developing countries, biomass fuel exposure has been consistently linked with chronic bronchitis and spirometrically defined COPD in women.10 ,12 Limited data from population-based studies suggest that there could be different clinical and gender-related risk exposure profiles between smoking and non-smoking COPD.6 ,13
There is uncertainty on the clinical relevance of COPD in never-smokers because of the lack of clinical data on never-smokers with irreversible airflow limitation in comparison to that in smokers. Such uncertainty raises doubt about whether irreversible airflow limitation in ever-smokers and never-smokers should be managed differently.10 ,14
Whether never-smokers with COPD share the phenotypes as their smoking counterparts is unclear. Few studies performed simultaneous evaluation of COPD in never-smokers and ever-smokers in the same study.6 ,7 Such evaluation would facilitate comparison of COPD in never-smokers with COPD in ever-smokers10 and provide insight into potential phenotypical differences in tobacco and non-tobacco related COPD at the population level. Hence, population-based studies using spirometry, including gender and systematic comparison of never-smokers and ever-smokers are needed to address this gap in our understanding of COPD in never-smokers.10
In this study, we analysed the data from the initial cross-sectional phase of the population-based, prospective Canadian Cohort of Obstructive Lung disease (CanCOLD) study. The primary objective was to determine the characteristics associated with COPD defined by postbronchodilator spirometry in never-smokers and ever-smokers in the general population. As a secondary objective, in a subgroup of the population cohort who had additional radiological and physiological data, we compared respiratory symptoms and exacerbations, plethysmographic lung volumes and DLCO abnormalities, and prevalence of emphysema on CT in never-smokers and ever-smokers, with and without COPD.
Materials and methods
Study population
The data from 5176 people from the general population, aged 40 years and older were evaluated. Data were collected between August 2005 and May 2009, in a large cross-sectional multisite, population-based study on lung health, which constituted the cross-sectional phase of the prospective longitudinal CanCOLD study. The study was initiated in Vancouver as part of the Burden of Obstructive Lung Disease (BOLD) study15 and then completed in eight other Canadian cities. The sampling strategy and study protocol of the baseline cross-sectional part of the study were the same as that used in the international BOLD initiative, the full details of which have been published elsewhere.15 ,16
Briefly, random samples were drawn from census data from Statistics Canada (Survey and Analysis Section; Victoria, Canada) and comprised of non-institutionalised adults, aged 40 years and older in nine urban cities across Canada (Vancouver, Montreal, Toronto, Halifax, Calgary, Quebec City, Kingston, Saskatoon and Ottawa). Recruitment was conducted by Nordic Research Group (NRG) Research group (Vancouver, Canada) by random telephone digit dialling to identify eligible individuals15 ,16 who were invited to attend a clinic visit to complete interviewer-administered respiratory questionnaires and to perform prebronchodilator and postbronchodilator spirometry.15 ,16 The mean clinic visit participation rate was 74% (range 63–87%).16
Definitions
Ever-smokers and never-smokers
The whole cohort was stratified into ever-smokers and never-smokers. Never-smokers were defined as individuals who had not smoked in their lifetime, more than 1 cigarette per day for 1 year (<1/20 pack years).15
COPD and Non-COPD subgroups
Two spirometric definitions for COPD were used: (A) ‘COPD definition derived from the Global Initiative for Chronic Obstructive Lung Disease (GOLD)17 based on postbronchodilator FEV1/FVC <0.70; and (B) the alternative definition for COPD as FEV1/FVC <5th centile (lower limits of normal, LLN). Ever-smokers and never-smokers were stratified into ‘Non-COPD’ and ‘COPD’ subgroups defined by FEV1/FVC <0.7 (GOLD criteria) or by FEV1/FVC<LLN, for comparison of the associated factors for COPD. Severity of COPD subgroups was further defined as mild (FEV1%pred ≥80%) or moderate-severe (FEV1%pred <80%). The reference equations derived from Hankinson et al18 were used in the spirometric definitions.
Exposures
Passive smoking at home was evaluated by asking the question: “has anyone living in your home (besides yourself) smoked a cigarette, pipe, or cigar in your home during the past two weeks.”
Biomass fuel exposure was defined as a lifetime exposure of 10 years or greater from the use of indoor fire using (1) coal or coke; (2) wood, crop residues or dung as the primary means of cooking or heating (details in online supplementary file).
Physiological and CT measurements
A subset of individuals who had CT scans of thorax and full lung function tests were assessed to determine the frequencies of emphysema, chronic respiratory symptoms and exacerbations and physiological measures of lung volumes and transfer factor (DLCO/Va).19 We had information on respiratory symptoms and exacerbations in 4890 subjects (2292 never-smokers and 2598 ever-smokers); pulmonary function testings in 977 subjects (456 never-smokers and 521 ever-smokers) and CT scans in 835 subjects (394 never-smokers and 441 ever-smokers). The grading of CT scans was done by two senior radiologists independently and blinded to the COPD or smoking status of subjects. Visually defined emphysema score was computed by the summation of the scores of the upper, middle and lower zones of right and left lungs on the CT scan using the method described in the COPDGene study.20
All participants gave written informed consent.
Statistical analysis
All statistical analyses were performed using SAS V.9.1 (SAS Institute, Cary, North Carolina, USA). A two-sided p<0.05, with adjustment for multiple comparisons using the Holm-Bonferroni correction was considered statistically significant.
Descriptive statistics are shown as counts and percentages for categorical data and means and SDs for continuous variables, unless otherwise stated.
Comparisons of variables between ever-smokers and never-smokers and between ‘non-COPD’ and ‘COPD’ were performed using Kruskal-Wallis test and χ2 test for continuous variables and categorical variables, respectively. Unweighted and weighted prevalences of COPD were calculated by smoking status for men and women.
To address the determinants for COPD, multivariable logistic regression models (parsimonious and full) were constructed to evaluate associations in all never-smokers and all ever-smokers; separately by sex and by COPD severity qualified by post- bronchodilator FEV1% predicted ≥80% and <80%. Covariates in the model included: age, body mass index (BMI) and years of education; exposure to organic dust, inorganic dust, biomass fuel (cooking or heating), environmental/passive tobacco smoke; history of childhood hospitalisation; cardiovascular comorbidity (heart disease, hypertension or diabetes); asthma and TB (details in online supplementary file).
Results
Of 5176 participants, 4893 (94%) individuals had spirometric measurements, which satisfied the American Thoracic Society (ATS) acceptability and repeatability criteria21 and were used in the analysis in the study.
Characteristics of never-smokers and ever-smokers in the study population
The study population comprised 47% never-smokers and 53% ever-smokers.
Table 1 shows the demographic characteristics and exposure types and use of respiratory medications in the whole cohort stratified by smoking status. Compared with ever-smokers, never-smokers were younger, included more women, had lower BMI, had more years of education, had lower frequencies of exposure to inorganic dust and noxious gases or vapours at work, and comorbidities, but had similar frequencies of self-reported physician diagnosis of asthma and TB, and use of respiratory medications
Demographic, exposure and clinical characteristics of the study population by smoking status (never-smokers vs ever-smokers)
Prevalence of COPD in never-smokers and ever-smokers by sex
Never-smokers accounted for 29% of all COPD identified by spirometry in the study.
The prevalence of airflow obstruction was 6.43% in never-smokers and 15.28% in ever-smokers when FEV1/FVC <5th centile, LLN criteria was used. Of ever-smokers with COPD, 62% had moderate-severe airflow obstruction (FEV1%pred <80%) compared with 43% of never-smokers with COPD (p<0.05).
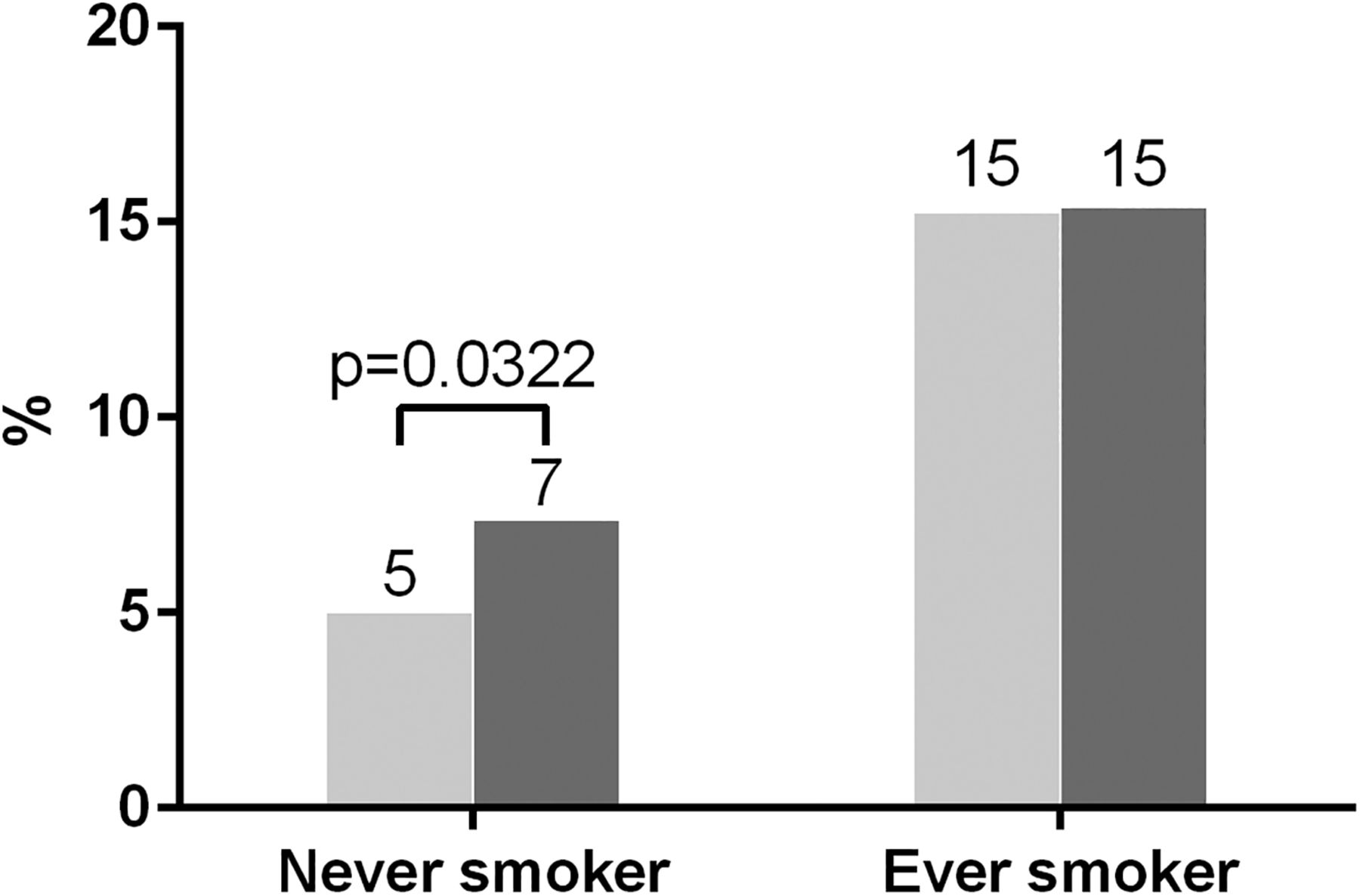
Figure 1 shows that COPD in never-smokers was more likely to affect women (7.4%) compared with men (5.0%) (p<0.0322). In contrast, COPD rates among smokers were similar for women and men.

Weighted prevalence (%) of COPD (FEV1/FVC<LLN) by sex, in never-smokers and ever-smokers. Pale column=men, dark column=women. LLN, lower limits of normal.
Factors independently associated with COPD in never-smoking men and women
Table 2 shows the adjusted OR and 95% CI from the multivariable logistic regression analyses for determining the ‘risk factors’ associated with COPD (defined by FEV1/FVC<LLN). In never-smokers with COPD of all severity, the common independent associations were older age and a history of asthma. For mild COPD, fewer years of education was a discriminative factor in men and passive smoking at home and cardiovascular comorbidities (heart disease or systemic hypertension or diabetes) were discriminative factors in women. For moderate and severe COPD, the additional common ‘risk factor’ was childhood hospitalisation for respiratory disease, while exposure to biomass fuel used for heating purposes for at least 10 years was a discriminative factor in women. Using the alternative definition for COPD (FEV1/FVC <0.7) and grading of mild (FEV1%pred ≥80%) and moderate-severe (FEV1%pred <80%), the results (not shown) remained unchanged.
Adjusted OR (aOR) for independent predictors associated with risk of different severity of COPD defined by lower limits of normal in male and female never-smokers
Factors associated with COPD in ever-smokers
There was no sex-related difference in risk factors for COPD in ever-smokers. Table 3 shows that the independently associated factors for COPD of all grades of severity (mild, moderate and severe) in ever-smokers were older age, pack years >20 and a self-reported history of physician diagnosed asthma. Low BMI was an associated factor for mild COPD while fewer years of education was an associated factor for moderate and severe COPD.
Adjusted OR (aOR) for independent predictors associated with risk of different severity of COPD defined by lower limits of normal in male and female ever-smokers
Comparison of clinical, physiological and structural characteristics of COPD in never-smokers with COPD in ever-smokers
Figures 2⇓–4 show the comparisons of COPD versus non-COPD for (A) respiratory symptoms including exacerbations and self-reported ever asthma (figure 2); (B) respiratory physiology (figure 3); and (C) visually defined emphysema, bronchiolitis and bronchiectasis on CT scans for never-smokers and ever-smokers (figure 4). Regardless of smoking status, individuals with COPD compared with those without COPD had more frequent respiratory symptoms of chronic cough, chronic phlegm, dyspnoea on exertion, wheeze in the last year; more likely to have previous experiences of respiratory exacerbations, and increased residual volume/total lung capacity ratio. Ever-smokers with COPD had increased total lung capacity, reduced transfer factor (DLCO/Va) and increased frequency of visually defined emphysema on CT scan compared with never-smokers with COPD. The prevalence of radiological bronchiectasis on CT was not significantly increased in COPD in smokers and non-smokers (details in online supplementary table S4).

Comparison of the proportion (%) of non-COPD and COPD subgroups who had respiratory symptoms (dyspnoea, chronic cough, chronic phlegm, ever-wheeze, exacerbation), history of exacerbations and ever-asthma in 2292 never-smokers (2131 non-COPD (grey column) and 161 COPD (black column)) (upper part of figure); and in 2598 ever-smokers (2202 non-COPD (grey column) and 396 COPD (black column)) (lower part of figure). An exacerbation was defined as ‘a period of worsening of breathing problems that got so bad that it interfered with usual daily activities or caused the individual to miss work’. *Proportion (%) in ever-smoking COPD significantly greater than that in never-smoking COPD (additional details in online supplementary table S4).

Comparison of respiratory physiology measurements residual volume/total lung capacity (%), functional residual capacity (FRC) (litres) and DLCO/Va (mL/min/mm Hg/l) in 456 never-smokers (346 non-COPD (grey column) and 110 COPD (black column)) (upper part of figure)); and in 521 ever-smokers (312 non-COPD (grey column) and 209 COPD (black column)) (lower part of figure). *Measurements in ever-smoking COPD significantly different from that in never-smoking COPD (additional details in online supplementary table S4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of thoracic CT scan findings: the proportion (%) of non-COPD and COPD subgroups with presence of visually defined emphysema, bronchiolitis and bronchiectasis in 394 never-smokers (308 non-COPD (grey column), 86 COPD (black column)) (upper part of figure); and in 441 ever-smokers (273 non-COPD (grey column) and 168 COPD (black column)) (lower part of figure). *Proportion (%) in ever-smoking COPD significantly greater than that in never-smoking COPD (additional details in online supplementary table S4).
Discussion
We have found similarities and differences in the characteristics of COPD between never-smokers and ever-smokers. First, we showed in this population study that never-smokers accounted for nearly 30% of the total burden of COPD in the community and that never-smokers with COPD were predominantly women. Second, the factors independently associated with COPD in never-smokers for men and women included increasing age, a diagnosis of asthma and severe childhood respiratory disease while passive smoking and exposure to biomass fuel heating were independent factors for COPD in women. No gender-specific difference in associated factors for COPD was found in ever-smokers, in whom COPD was similarly linked with increasing age, a diagnosis of asthma, severe childhood respiratory disease, but additionally, with increasing lifetime exposure (pack years) to cigarette smoking. Finally, in a preliminary evaluation of a subset of the cohort to assess phenotypical differences in COPD, we showed that COPD in never-smokers and ever-smokers had a similar respiratory symptoms profile but were different in radiological and physiological presentations.
The finding in this study that nearly 30% of all people diagnosed with COPD have never smoked was consistent with reported proportions of 25–30% in USA,5 Europe4 ,7 and China.1 ,6 As 47% of our study population were never-smokers, and 10% of these had COPD, this would translate into an overall population prevalence of 4.7% or 1.08 million individuals with airway obstruction in a population of about 23 million Canadians aged 40 years or older. Notably, about 70% were women, suggesting that women could be more susceptible to non-smoking risk factors associated with COPD.11 ,22 We did not observe this gender distribution in COPD for ever-smokers, conceivably due to the overriding effect of tobacco smoke exposure in the causation of COPD.
The finding of sexual dimorphism in risk factors for COPD is intriguing. A positive history of environmental tobacco smoke exposure (passive smoking) and prolonged (>10 years) exposure to biomass fuels combustion for heating were factors independently associated with COPD in women. Biomass fuel combustion had been clearly linked with the occurrence of COPD in women in developing countries such as India2 and China1 but to our knowledge had not been reported in the developed countries of North America or Western Europe. Our finding that exposure to biomass fuel combustion was related to moderate and severe COPD in Canada cautioned against the general assumption that the risk of biomass fuel exposure was not a relevant risk factor for COPD among women in developed countries.23 ,24 However, it is unclear what biomass exposure represents in Canada, where the exposure frequencies of 11–14% seem to be higher than that (5%) quoted for developed countries.25 Conceivably it could be a surrogate for poverty or social economic status,12 or could be due to behavioural, environmental and lifestyle differences between men and women though differences in biological or genetic predisposition could not be excluded.11 ,22 ,26 Further clarification requires studies on detailed and seasonal household air quality data and longitudinal follow-up data.
A pivotal finding in this study is that a history of asthma is the most consistent independently associated factor for COPD regardless of smoking status. Long-standing asthma and the risk for COPD as defined by the presence of non-fully reversible chronic airway obstruction has been well documented in smokers and never-smokers.10 Individuals with chronic asthma have a greater than normal rate of decline in lung function with age, further magnified by presence of smoking.24 ,27 The findings in this study that self-reported concurrent doctor-diagnosis of asthma occurred in 36% of all COPD in never-smokers and 30% of COPD in ever-smokers, are consistent with published proportions of between 15% and 55% of patients with COPD, a combination which could alternatively be labelled as the ‘asthma-COPD overlap syndrome’.17
In our study population, a history of childhood hospitalisation for respiratory illness was also a significant predictor of COPD irrespective of smoking status, presumably through the negative effect on lung function described in several studies which found an adverse association between early childhood lung infections and FEV1.17 Such childhood ‘disadvantages’ which collectively could also include maternal smoking during childhood, poverty and low socioeconomic status, might be as important as heavy smoking in predicting lung function and increasing the individual's risk of developing COPD.28
Finally, the paucity of phenotypical data in never-smokers with chronic airflow obstruction had long cast doubt on aligning COPD in never-smokers with COPD in ever- smokers.10 ,14 In the Copenhagen General Population Study on outcomes of COPD, Thomsen et al29 reported increased risk of respiratory hospitalisations but not of total mortality for never-smoking individuals with COPD compared with smokers with COPD. To our knowledge, physiological and CT characteristics of COPD in never-smokers versus ever-smokers from the general population had not been systematically studied. In a preliminary comparative analysis of clinical variables, respiratory physiology and visual scores from multiple detector computed tomography scan of the lungs in individuals with and without COPD in never-smokers and ever-smokers, we found that there were phenotypical differences between COPD in never-smokers and ever-smokers in the general population. It is intriguing that respiratory symptoms such as chronic cough, chronic phlegm and wheeze and exertional dyspnoea are features of COPD regardless of smoking status though more frequent in ever-smokers. The burden of respiratory exacerbations, an outcome29 and a phenotypical feature for COPD,30–32 was also equally prevalent in ever-smokers and never-smokers with COPD.
The key differences appeared to be physiological and radiological. Although never-smokers and ever-smokers with COPD had lung hyperinflation and air trapping, never-smokers with COPD were less likely to have emphysema on CT scan and hence by default labelled as ‘airway predominant phenotype’20 compared with smokers with COPD who were more likely to have a reduced diffusing capacity and emphysema, hence ‘emphysema predominant phenotype’. These initial findings provide some insight into potential phenotypical differences31 ,33 but should be interpreted with caution and await validation from longitudinal data of the study.
Limitations
There are potential limitations in this study. First, the ideal definition for COPD remains controversial.34 ,35 In this analysis, we had used two spirometric definitions of airflow obstruction as study definitions of COPD, namely the GOLD definition: and the alternative definition, (LLN), but chose to present results from the LLN definition. COPD disease severity was assumed in each case by the level of FEV1% predicted.8 ,35 Another limitation is that, in our analysis, a doctor diagnosis of asthma was self-reported rather than from health records and hence could be affected by recall bias. We did not exclude individuals with asthma from the analysis as asthma was equally prevalent in ever-smokers and never-smokers. Hence, some of the patients we were labelling as COPD may have had fixed airflow obstruction and remodelling related to long-standing asthma, and some may have had poorly controlled asthma which was not completely reversed with bronchodilators. Another caveat is the weak definition of passive smoking. Lastly, only cross-sectional data were used in the analysis. Hence these findings should be interpreted with caution as confirmation would require data from the longitudinal phase of the study.
Conclusion
In summary, the study confirmed the substantial burden of COPD among never-smokers, defined the common and gender-specific risk factors for COPD in never-smokers and provided early insight into potential phenotypical differences in COPD between lifelong never-smokers and ever-smokers. The establishment of phenotypical differences for COPD in never-smokers and ever-smokers could provide clearer outcomes needed for better COPD management and for clinical trials to evaluate novel treatments for COPD.
Acknowledgments
The authors thank the men and women who participated in the study and individuals in the CanCOLD Collaborative research Group: Executive Committee: Jean Bourbeau, (Mcgill University, Montreal, QC, Canada); Wan C Tan, J Mark FitzGerald; D D Sin. (UBC, Vancouver, BC, Canada); D D Marciniuk (University of Saskatoon, Saskatoon, SASK, Canada) D E O'Donnell (Queen's University, Kingston, ON, Canada); Paul Hernandez (University of Halifax, Halifax, NS, Canada); Kenneth R Chapman (University of Toronto, Toronto, ON, Canada); Robert Cowie (University of Calgary, Calgary, AB, Canada); Shawn Aaron (University of Ottawa, Ottawa, ON, Canada); F Maltais (University of Laval, Quebec City, QC, Canada); International Advisory Board: Jonathon Samet (the Keck School of Medicine of USC, California, USA); Milo Puhan (John Hopkins School of Public Health, Baltimore, USA ); Qutayba Hamid (McGill University, Montreal, Qc, Canada); James C Hogg (UBC James Hogg Research Center, Vancouver, BC, Canada). Operations Center: Jean Bourbeau (PI), Carole Baglole, Carole Jabet, Palmina Mancino, Yvan Fortier, (University of McGill, Montreal, QC, Canada); Wan C Tan (co-PI), Don Sin, Sheena Tam, Jeremy Road, Joe Comeau, Adrian Png, Harvey Coxson, Miranda Kirby, Jonathon Leipsic, Cameron Hague (University of British Columbia James Hogg Research Center, Vancouver, BC, Canada). Economic Core: Mohsen Sadatsafavi (University of British Columbia, Vancouver, BC). Public Health core: Teresa To, Andrea Gershon (University of Toronto) Data management and Quality Control: Wan C Tan, Harvey Coxson, (UBC, Vancouver, BC, Canada); Jean Bourbeau, Pei-Zhi Li, Jean-Francois Duquette, Yvan Fortier, Andrea Benedetti, Denis Jensen (Mcgill University, Montreal, QC,Canada), Denis O'Donnell (Queen's University, Kingston, ON, Canada. Field Centers: Wan C Tan (PI), Christine Lo, Sarah Cheng, Cindy Fung, Nancy Ferguson, Nancy Haynes, Junior Chuang, Licong Li, Selva Bayat, Amanda Wong, Zoe Alavi, Catherine Peng, Bin Zhao, Nathalie Scott-Hsiung, Tasha Nadirshaw (UBC James Hogg Research Center, Vancouver, BC); Jean Bourbeau (PI), Palmina Mancino, David Latreille, Jacinthe Baril, Laura Labonte (McGill University, Montreal, QC, Canada ); Kenneth Chapman (PI), Patricia McClean, Nadeen Audisho, (University of Toronto, Toronto, ON, Canada); Robert Cowie (PI), Ann Cowie, Curtis Dumonceaux, Lisette Machado(University of Calgary,Calgary, AB, Canada); Paul Hernandez (PI), Scott Fulton, Kristen Osterling (University of Halifax, Halifax, NS, Canada ); Shawn Aaron (PI), Kathy Vandemheen, Gay Pratt, Amanda Bergeron (University of Ottawa, Ottawa, ON, Canada); Denis O'Donnell (PI), Matthew McNeil, Kate Whelan (Queen's University, Kingston, ON, Canada); Francois Maltais (PI), Cynthia Brouillard (University of Laval, Quebec City, QC, Canada); Darcy Marciniuk (PI), Ron Clemens, Janet Baran (University of Saskatoon, Saskatoon, SK, Canada).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Collaborators CanCOLD Collaborative Research Group (listed in acknowledgements).
Contributors WCT contributed to the conception and design of the study, the acquisition of the data, the analysis of the data and the writing. She assembled the data set and takes responsibility for the integrity of the data and the accuracy of the data analysis. JB, JMF, RC, KRC, PH, SDA, DDM, DEO, FM, CH, JL and JR contributed to the acquisition of the data and the writing and revision of the article. ASB and JCH contributed to the conception, design of the study and the revision of the article. DDS, MK, HC contributed to the analysis and interpretation of the data and the writing of the article. All authors approved the final version of the manuscript.
Funding The Canadian Cohort of Obstructive Lung Disease (COLD/CanCOLD) is funded by the Canadian Institute of Heath Research (CIHR/Rx&D Collaborative Research Program Operating Grants- 93326); the Respiratory Health Network of the FRSQ; the Canadian Respiratory Research Network (CRRN); the Canadian Institutes of Health Research (CIHR)—Institute of Circulatory and Respiratory Health; Canadian Lung Association (CLA)/Canadian Thoracic Society (CTS); British Columbia Lung Association; industry partners Astra Zeneca Canada, Boehringer-Ingelheim Canada, GlaxoSmithKline Canada, Merck, Novartis Pharma Canada, Nycomed Canada, Pfizer Canada; The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests WCT and JB report unrestricted educational grants from GSK, Pfizer, BI, AZ for the epidemiological COLD study; grants from funding for the operations of CanCOLD Longitudinal Epidemiological Study from the Canadian Institute of Heath Research (CIHR/Rx&D Collaborative Research Program Operating Grants93326) with industry partners AZ Canada, BI Canada, GSK Canada, Merck, Novartis Pharma Canada, Nycomed Canada, Pfizer Canada, outside the submitted work. WCT also received personal fees from GSK board membership. DDM, an employee of the University of Saskatchewan, received funding from the Canadian Institutes of Health Research (via McGill University) to undertake this research. KRC reports grants from Novartis, grants from Almirall, grants from Boehringer Ingelheim, grants from Forest, grants from GSK, grants from AstraZeneca, grants from Amgen, grants from Roche, grants from CSL Behring, grants from Grifols, grants from Genentech, grants from Kamada, during the conduct of the study; others from CIHRGSK Research Chair in Respiratory Health Care Delivery, outside the submitted work. P H reports grants from Canadian Institute Health Research, during the conduct of the study; grants and personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Merck, Novartis, Takeda, Grifols, CSL Behring, Pfizer, Almirall outside the submitted work. FM received fees for speaking at conferences sponsored by Boehringer Ingelheim, GlaxoSmithKline and Novartis and Grifols. He received research grants for participating in multicentre trials sponsored by GlaxoSmithKline, Boehringer Ingelheim, Astra Zeneca, Nycomed and Novartis. He received unrestricted research grant from Boehringer Ingelheim and GlaxoSmithKline. He holds a CIHR/GSK research chair on COPD. DDS reports personal fees from Almirall, personal fees from AstraZeneca, grants from AstraZeneca, personal fees from Novartis, personal fees from Amgen, outside the submitted work; SDA, ASB, JCH, JMF, CH, JL, JR, MK, HC, DEO and RC have no conflicts of interest to declare.
Ethics approval The study was approved by the respective university and institutional ethical review boards :UBC/ PHC Research Ethics Board, P05-006 (Vancouver); Biomedical-C Research Ethics Board, BMC-06-002 (Montreal); UHN REB, 06-0421-B (Toronto); Capital Health Research Ethics Board, CDHA-RS/2007-255 (Halifax); Conjoint Health Research Ethics Board, ID21258 (Calgary); DMED-1240-09 (Kingston); 2009519-01H (Ottawa); Bio-REB09-162 (Saskatoon); CER20459 (Quebec City).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data sharing is available via the CANCOLD process through WCT (e mail: wan.tan@hli.ubc.ca) and JB (e mail: jean.bourbeau@mcgill.ca).