Article Text

Abstract
Background Pleural malignant mesothelioma (MM) is a deadly tumour predominantly associated with asbestos exposure. A reliable diagnostic and prognostic marker for MM will significantly enhance clinical care and is an area of intense research. Soluble mesothelin is the most studied and an FDA-approved biomarker for MM. A recent report showed promising results using fibulin-3 as a new diagnostic marker. The aim of this study was to compare the utility of fibulin-3 versus mesothelin, singly or in combination.
Methods Fibulin-3 and soluble mesothelin were determined by ELISA in the plasma and pleural fluid of 153 patients presenting with a pleural effusion including 82 with MM, 36 with non-MM malignant effusions and 35 with benign effusions. Biomarker concentrations were determined in the plasma of an additional 49 cases with benign asbestos-related disease.
Results Mesothelin provides better diagnostic accuracy than fibulin-3 for MM whether measured in plasma or pleural effusion: area under the curve (AUC) for plasma was 0.822 (95% CI 0.76 to 0.87) compared with 0.671 (0.61 to 0.73), respectively, and for pleural fluid AUC was 0.815 (0.74 to 0.87) compared with 0.588 (0.51 to 0.67), respectively. Effusion fibulin-3 was an independent significant prognostic factor for survival in MM patients; HR 2.08 (1.14 to 3.82), p=0.017. MM patients with effusion fibulin-3 levels below the median survived significantly longer than those with levels above the median (14.1 vs 7.9 months, p=0.012). Mesothelin and neutrophil to lymphocyte ratio were not significant prognostic markers.
Conclusions Soluble mesothelin is a superior diagnostic biomarker for MM compared with fibulin-3, whereas fibulin-3 provides superior prognostic information compared with mesothelin.
- Mesothelioma
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key message
What is the key question?
-
How does the diagnostic accuracy of the newly proposed malignant mesothelioma biomarker fibulin-3 compare with the ‘gold standard’ biomarker, soluble mesothelin?
What is the bottom line?
-
While fibulin-3 levels are elevated in the plasma of mesothelioma patients compared with controls, soluble mesothelin has a much greater diagnostic accuracy and fibulin-3 levels in pleural effusions are not specific for mesothelioma.
Why read on?
-
Despite the academic and public interest in fibulin-3 as a new malignant mesothelioma biomarker, to date, mesothelin remains the most clinically useful mesothelioma biomarker.
Introduction
Malignant mesothelioma (MM) is an asbestos-induced, incurable and aggressive tumour, predominantly of the pleura.1 ,2 Better diagnostic tools are needed to diagnose MM.3 ,4 Diagnosis is protracted, requiring repeat biopsies that add to patient discomfort and risk, and health system utilisation and expense.5 ,6 MM patients generally present with a pleural effusion; however, pleural effusion can also arise as a result of other cancers and over 60 benign conditions. Thus, a tumour marker sensitive and specific for MM would aid diagnosis by indicating the need for a biopsy of the pleura at an earlier stage. Timely diagnosis would provide the opportunity to offer treatment to patients at an earlier time when tumours are smaller, localised and more accessible, potentially changing outcomes. This has yet to be extensively studied in MM.
No blood-based marker is routinely used in clinical practice to diagnose MM. Mesothelin was identified as a potential MM biomarker over 10 years ago showing, at a 95% specificity, a sensitivity of 84% for advanced MM.7 At the same high specificity, sensitivity was reduced to 50% at diagnosis.8 Recently, a new highly promising biomarker for MM was reported, fibulin-3,9 a secreted glycoprotein which is highly upregulated in glioma where it has been shown to promote tumour growth and invasion,10 possibly via phosphorylation of epidermal growth factor receptor and downstream activation of AKT and mitogen-activated protein kinase.11 Plasma fibulin-3 had a sensitivity of over 96% for MM at a specificity of 95%, and pleural effusion fibulin-3 had a sensitivity of 84% and specificity of 93%. Pleural effusion fibulin-3 was also an independent prognostic marker for survival in MM patients who underwent cytoreduction surgery.9
We directly compared the diagnostic and prognostic accuracy for MM of both markers, individually and together, in the same samples taken near the time of diagnosis with samples from patients with common conditions which are typically considered in the diagnostic differential. Prognostic variables for MM patients including the European Organisation for Research and Treatment of Cancer (EORTC)12 and Cancer and Leukaemia Group B (CALGB)13 scoring systems and the recently described neutrophil to lymphocyte ratio14 were also compared with the biomarkers in prognostic models for overall survival in MM patients.
Materials and methods
Case and control selection
Samples were sourced from the Australian Mesothelioma Tissue Bank which prospectively collects biospecimens from consenting patients presenting at respiratory and asbestos review clinics at Sir Charles Gairdner and Hollywood Hospitals. MM cases were identified with samples available from within 1 month either side of clinical diagnosis, prior to treatment and the diagnosis was confirmed by the Western Australian Mesothelioma Registry which reviews and verifies all MM cases diagnosed in the state.15 Where available, tumour histology, tumour stage, EORTC prognostic group,12 CALGB prognostic group,13 neutrophil to lymphocyte ratio,16 treatment and survival were recorded for MM patients.
Controls with either benign or non-MM malignant effusions or with benign asbestos-related disease (ARD), who had a matching plasma sample available within 7 days of their effusion, were randomly selected. All samples were collected between October 2007 and September 2012.
Final diagnosis in all patients was confirmed by experienced pathologists and included clinical follow-up until death or for an average of 17 and 13 months for benign and malignant controls, respectively, to confirm that the clinical pattern matched the diagnosis. Effusions were classified as being malignant on the basis of cytological and immunohistochemical features in the context of imaging findings consistent with an invasive pleural malignancy.17 ,18 Non-malignant effusions were classified as exudates or transudates by Light's criteria.19 This study was approved by the human ethics committees of Sir Charles Gairdner Hospital and Hollywood Hospital, Perth, Western Australia.
Blood samples were collected into EDTA plasma tubes and processed within 2 h or alternatively were stored at 4°C overnight before processing. Samples were centrifuged at 400 g for 10 min and the supernatant was aliquoted and stored at −80°C. Effusions were collected without preservative, centrifuged for 10 min at 400 g and the supernatant was stored at −80°C.
Fibulin-3 assay
Fibulin-3 concentrations were determined using an ELISA (USCN Life Science Inc. Houston, Texas, USA). Plasma and effusion samples were diluted 1:4 and 1:40 respectively in the supplied diluent. Fibulin-3 values of ≥53 and ≥346 ng/mL in plasma and effusions respectively were considered positive for MM.9 Samples below the manufacturer's stated limit of detection were reported as 0.15 ng/mL.
Mesothelin assay
Mesothelin concentrations were determined following the manufacturer's instructions using the MESOMARK kit (Fujirebio Diagnostics, Malvern, Pennsylvania, USA). A mesothelin value of ≥2.5 nM was considered positive for MM.20 ,21 A cut-off value for pleural effusion mesothelin of 20 nM was previously established.22 Results below the manufacturer's limit of detection were reported as 0.1 nM.
All ELISAs for mesothelin and fibulin-3 were performed on coded samples by two separate trained technicians who were unaware of the patient's diagnosis or of the result obtained for the alternative analyte measured by the other technician, for each sample. The results and quality control standards for each assay were independently reviewed.
Statistical analysis
Sample size calculations were based on estimates from previous studies. Plasma fibulin-3 was reported to have a sensitivity of 97% for MM patients9 and we assumed a more conservative sensitivity of 80% based on the common finding that replication studies are less sensitive than the study they are replicating. Mesothelin has a sensitivity of 50% in MM patients at diagnosis.8 A sample size of 36 (per group) was estimated to provide 80% power, at α level of 5% to compare sensitivities when the true sensitivities are 50% and 80%. A survival power analysis estimated that 80 MM patients would be sufficient to detect an HR of 2.0 difference in survival between two groups dichotomied on high or low fibulin-3, with a power of 80% and α level of 5%, assuming a median survival of 9 and 20 months of follow-up.
A random sampling algorithm was used to select cases and controls (Microsoft Excel 2010, Redmond, Washington, USA). Statistical analyses were performed using IBM SPSS statistics V.20 (Armonk, New York, USA). Summary results were reported as the median and IQR and the patient groups were compared using the non-parametric tests procedure, with adjustment for multiple comparisons using the Dunn–Bonferroni method. Correlations were performed using the Spearman's correlation function. Standardised scores using the mean and SD of natural logarithm transformed results from benign controls were used to combine fibulin-3 and mesothelin results. Logistic regression to predict case/control status was used to determine the weight to be given each marker, which was then linearly added to give a combined biomarker value. Cox regression survival analysis was performed using the Cox regression procedure using log(10) transformed biomarker values. For multivariable analysis, EORTC and CALGB prognostic groups and treatment were excluded because they are measures derived from combinations of other factors included in the model. Survival analysis was also performed using the Kaplan–Meier product limit procedure with patients dichotomised into groups based on median biomarker concentration.
Results
Patient characteristics
This patient cohort included 82 patients with newly diagnosed pleural MM; eight with sarcomatoid, 13 with biphasic, 32 with epithelioid histology and 29 diagnosed from pleural fluid immunocytology.23 ,24 The non-MM individuals included 49 patients with benign asbestos-related pulmonary diseases (asbestosis and/or pleural plaques) (ARD); 35 patients with non-malignant effusions (20 had exudative effusions, eight had transudate effusions and seven with equivocal or unknown effusion biochemistry); and 36 people who presented with effusions due to other malignancies (18 with primary lung cancer, three each with breast, blood-based, and ovarian cancer, two each with melanoma, pancreatic and prostate cancer and one each with colon cancer, sarcoma and unknown primary) (table 1). There was no significant difference in age between the groups. As is typical, there were significantly more men in the ARD and MM groups (p<0.05).
Patient characteristics and biomarker levels
Fibulin-3 levels in plasma
Plasma fibulin-3 of MM patients collected within 1 month of diagnosis ranged from 8.6 to 307 ng/mL (figure 1A). Fibulin-3 levels were significantly higher in the plasma of patients with MM than patients with benign disease (p<0.01) and other malignancies (p<0.001). At the previously reported threshold of 52 ng/mL, plasma fibulin-3 had a sensitivity of 22% (18/82) and specificity of 95% (114/120). In post hoc analysis, at a threshold of 29 ng/mL, plasma fibulin-3 had a sensitivity of 48% (39/82) and specificity of 71% (85/120). Receiver operating characteristic (ROC) curves were generated to assess the ability of the marker to distinguish patients with MM from other patients in this study; the area under the curve (AUC) for fibulin-3 was 0.671 (95% CI 0.606 to 0.732). There was no statistical difference in fibulin-3 levels with different MM histologies (figure 1C) or tumour stage (data not shown).
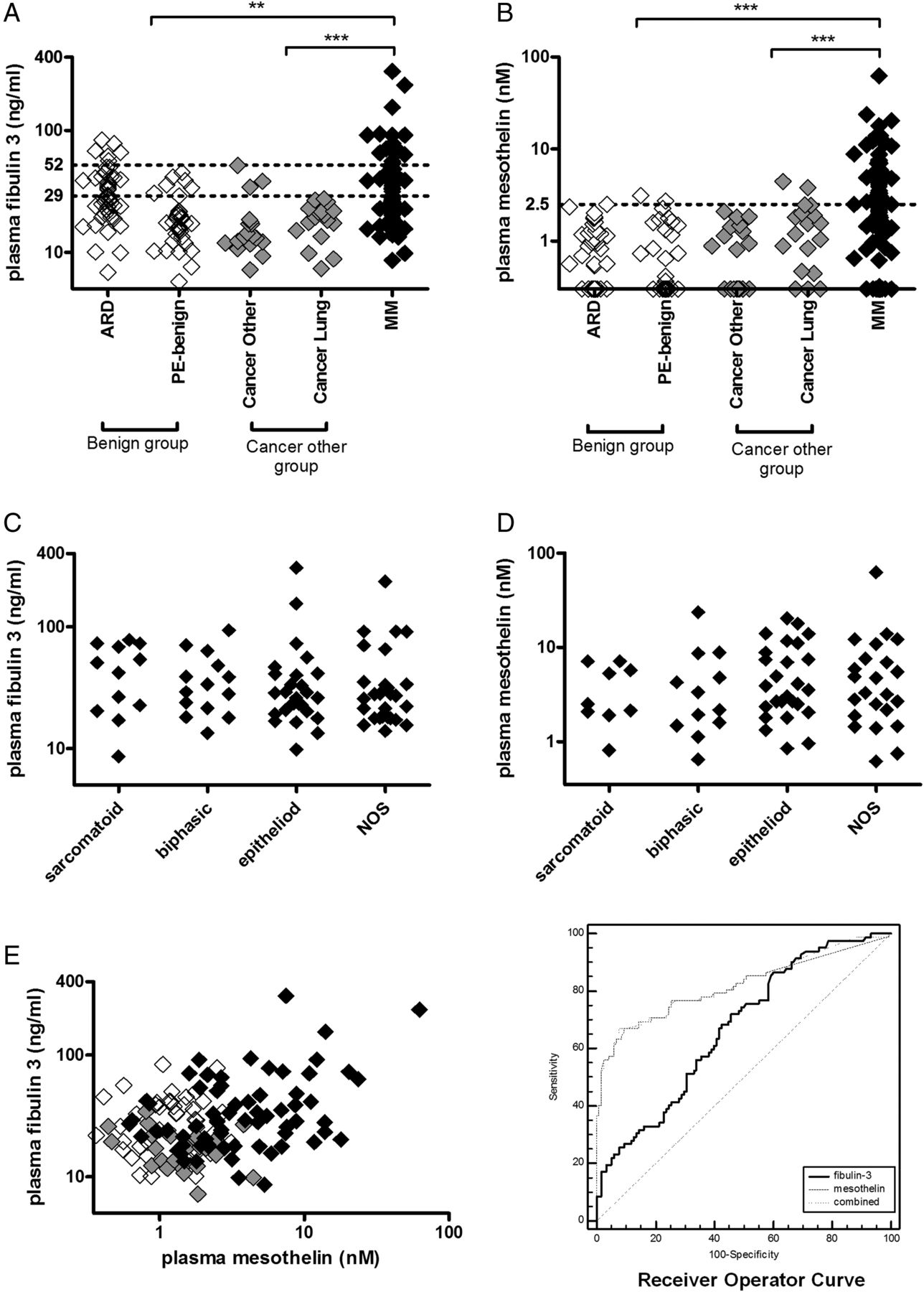
Biomarker concentrations in plasma. (A and B) Fibulin-3 (A) and soluble mesothelin (B) in plasma of patients with asbestos-related disease (ARD), benign pleural effusions (PE-benign) and malignancies (MM, lung cancer and other). Horizontal dashed lines indicate threshold cut-offs at the indicated values; (C and D) fibulin-3 (C) and soluble mesothelin (D) in plasma of MM patients segregated by tumour histology (NOS, not otherwise specified); (E) bivalent scatterplot of plasma fiblun-3 and mesothelin in patients with MM (closed diamonds), benign conditions (open diamonds) and non-MM malignancies (grey diamonds); and (F) receiver operating characteristic curve showing accuracy of plasma biomarkers in differentiating patients with MM (n=82) from all other patients in the study (n=121). Significant difference between indicated cohorts: ** p<0.01; *** p<0.0001. MM, malignant mesothelioma.
Soluble mesothelin levels in plasma
In the same set of samples, the plasma mesothelin level in MM patients ranged from undetectable to 62 nM (figure 1B). Plasma mesothelin levels were significantly higher in patients with MM than the patients with benign disease (p<0.001) and patients with other malignancies (p<0.001). At the 2.5 nM threshold, plasma mesothelin had a sensitivity of 56% (46/82) and specificity of 96% (115/120). There was no relationship between the levels of mesothelin and the histological subtype of the patients’ MM (figure 1D). There was a significant correlation between plasma fibulin-3 and mesothelin levels in MM patient plasma rs=0.3602 (p<0.001) but not in non-MM patients (figure 1E). The AUC for plasma mesothelin of 0.816 (0.755 to 0.867) was significantly higher than for fibulin-3 (p=0.003) (figure 1F). Using a logistic regression model, the diagnostic capabilities of fibulin-3 and mesothelin were combined generating a ROC curve with an AUC of 0.822 (95% CI 0.762 to 0.872). Combining fibulin-3 and mesothelin with this approach offers no diagnostic advantage over mesothelin alone (figure 1F).
Fibulin-3 levels in pleural effusion
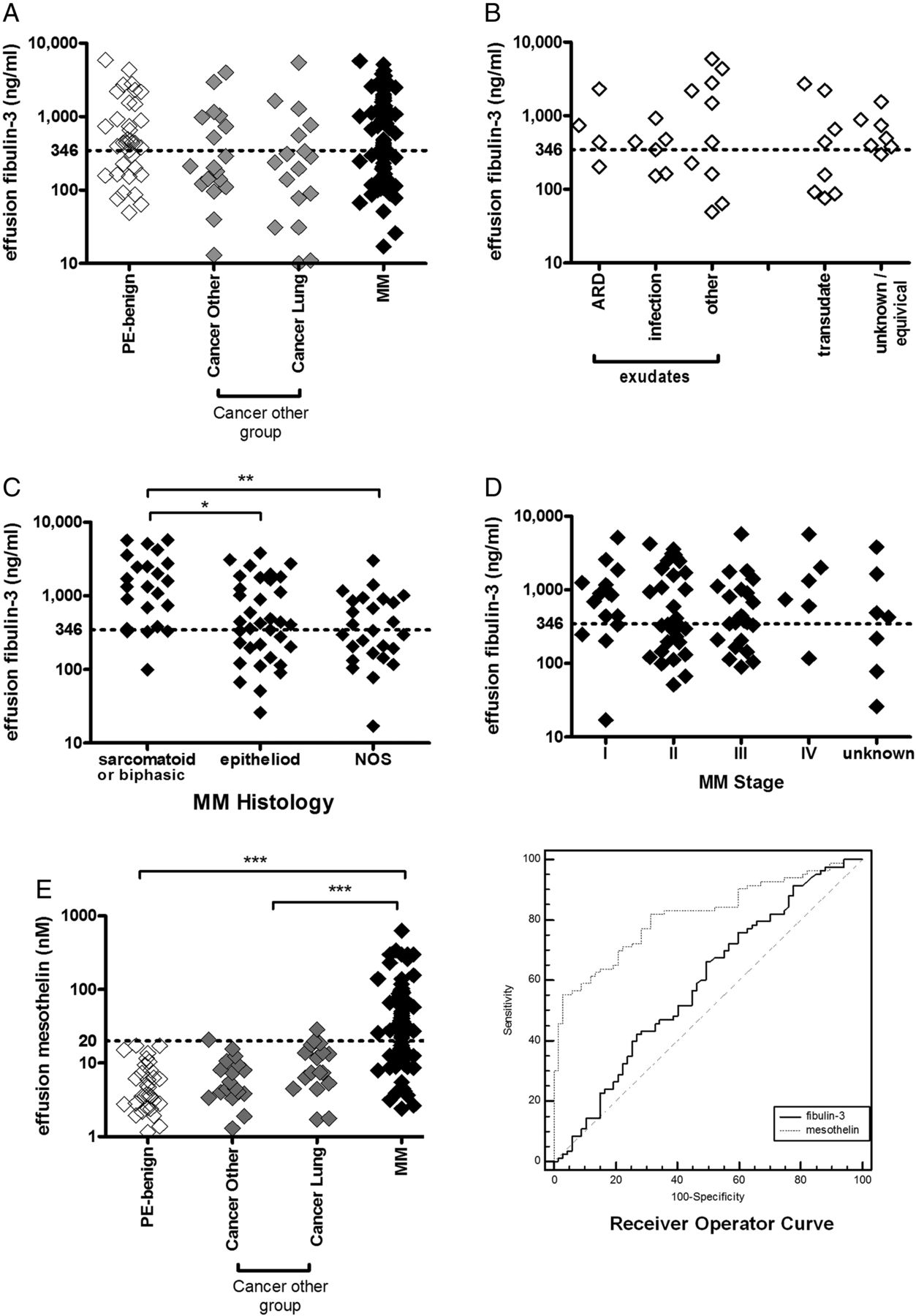
Effusion fibulin-3 levels of MM patients collected within 1 month of diagnosis and prior to any treatment ranged from 17 to 5748 ng/mL (figure 2A). There was no significant difference in fibulin-3 levels between the diagnostic groups; 63% of benign effusions were above the 346 ng/mL cut-off. In post hoc analysis, there was no statistical difference in fibulin-3 levels dependent upon a benign effusion being an exudate or transudate (figure 2B) or the presence of blood in the effusion (data not shown). In a subset of benign effusion samples (n=22), lactate dehydrogenase (LDH) levels were available and there was a correlation between LDH and fibulin-3 levels (rs=0.673; p<0.001). MM patients with biphasic or sarcomatoid histology had significantly higher effusion fibulin-3 concentrations (1331, IQR 538–2486 ng/mL) compared with patients with epithelioid histology (426, 171–1709 ng/mL, p=0.018) or patients diagnosed by cytology (298, 155–881 ng/mL, p=0.002) (figure 2C). There was no significant difference in fibulin-3 levels and MM tumour stage (figure 2D). At a threshold of 346 ng/mL effusion, fibulin-3 had a sensitivity of 59% and specificity of 52%. The AUC for effusion fibulin-3 to distinguish MM from all other patients in this study was 0.588 (0.505 to 0.668) (figure 2F).

Biomarker concentrations in pleural effusions. (A) Fibulin-3 concentrations in pleural effusions of patients with benign aetiologies (PE-benign), and malignancies (MM, lung cancer and other); (B) fibulin-3 concentrations in pleural effusions of patients with benign conditions segregated by fluid biochemistry and effusion aetiology; (C) effusion fibulin-3 in MM patients segregated by tumour histology (NOS, not otherwise specified); (D) effusion fibulin-3 in MM patients segregated by tumour stage; (E) soluble mesothelin concentrations in pleural effusions of patients with benign aetiologies and malignancies; and (F) receiver operating characteristic curve showing accuracy of pleural effusion biomarkers in differentiating patients with MM (n=103) from all other patients in the study (n=71). Horizontal dashed lines indicate threshold cut-offs at the indicated values; significant difference between indicated cohorts: * p<0.05, ** p<0.01, *** p<0.0001. MM, malignant mesothelioma. Open diamonds – non malignant asbestos related disease; grey diamonds – other cancer; black diamonds – MM.
Soluble mesothelin levels in pleural effusion
In matching samples, the effusion mesothelin level in patients with MM ranged from 0.6 to 630 nM (figure 2B). Effusion mesothelin levels were significantly higher in patients with MM than in patients with non-malignant exudative effusions (p<0.001) and other malignancies (p<0.001). At the 20 nM threshold, mesothelin had a sensitivity of 58% and specificity of 96%. The AUC for effusion mesothelin was 0.815 (0.743 to 0.874) for distinguishing patients with MM from other patients, significantly higher than for fibulin-3 (figure 2F).
Correlation between biomarkers in plasma and effusion
There was no correlation between plasma and pleural effusion fibulin-3 levels, analysed either per group or for all subjects. There was a significant correlation between plasma and pleural effusion mesothelin levels (rs=0.533, p<0.0001) for all subjects.
Survival analysis
Treatment data were available for 78 of the MM patients; four patients underwent tumour resection; 37 had combination pemetrexed- and platinium-based chemotherapy and 37 patients received best supportive care only. By the end of the observation period, 72 patients had died and 10 patients remained alive. The median survival of the deceased patients after diagnosis was 8.9 (95% CI 5 to 12) months. The patients surviving at the end of the study had been followed for a median duration of 20.5 (range 12–49) months.
A linear negative relation between survival and effusion fibulin-3 was observed (table 2). Increasing age, biphasic or sarcomatoid histology, poor performance status, high haemoglobin, high platelet count, CALGB prognostic group 5 or 6, and absence of active treatment were also negative univariable prognostic predictors. Neither plasma fibulin-3 nor plasma or effusion mesothelin was a significant prognostic predictor in univariable analyses. Effusion fibulin-3 remained significant in a multivariable analysis that excluded EORTC and CALGB prognostic groups and treatment; however, missing clinical data resulted in exclusion of nearly 16% of cases (table 2). Multivariable analysis including only variables with complete data sets demonstrated that effusion fibulin-3 (HR 2.05 (1.24 to 3.39) p=0.005), age (HR 1.05 (1.01 to 1.08) p=0.011) and histology (HR 1.52 (1.10 to 2.09) p=0.012) were significant prognostic predictors. MM patients with low effusion fibulin-3 (<467 ng/mL) survived significantly longer than those with high effusion fibulin-3 (14.1, 95% CI 10.5 to 17.7 vs 7.9, 95% CI 4.9 to 10.9 months, p=0.012) (figure 3).
Survival analysis

{kind=link}
{kind=link}
{kind=link}
Survival of malignant mesothelioma patients segregated on (A) pleural effusion fibulin-3 concentration, (B) European Organisation for Research and Treatment of Cancer (EORTC) prognostic group, (C) Cancer and Leukaemia Group B (CALGB) prognostic group and (D) neutrophil to lymphocyte ratio (NLR) at diagnosis.
Discussion
Recently, the secreted glycoprotein fibulin-3 has been reported to have impressive diagnostic accuracy for MM diagnosis.9 However, the present study shows that while fibulin-3 is elevated in MM, it is not superior to the more extensively studied mesothelin as a biomarker for MM in either plasma or pleural effusions.
The published finding that fibulin-3 is elevated in MM patient plasma is confirmed in our study, although at a lower sensitivity. Interestingly, a discrepancy in the diagnostic accuracy between the two cohorts in the original study was noted: sensitivity for MM 97% at a 95% specificity in the US cohort versus an estimated sensitivity of 40% at a 95% specificity in the Canadian cohort.9 The discrepancy was possibly not clear because of the use of the different threshold values in the two cohorts. The Canadian result is more similar to that reported in this study, that is, 22% sensitivity. The lower sensitivity seen in the current study could also relate to the fact that the Australian samples were all from within 1 month of diagnosis and prior to any treatment. This finding of lower sensitivity early in the course of disease was noted in the first mesothelin studies and presumably relates to less tumour bulk.8
Fibulin-3 was suggested to be a superior marker for discriminating between MM patients and asbestos-exposed persons and patients with effusions not due to MM compared with that of other published markers9 based upon the results of AUC analysis and published data. In the current study, the two markers were directly compared in the same plasma samples. While the manufacturers of the MESOMARK assay recommend sera, we have previously found that plasma and serum mesothelin have virtually identical sensitivity for MM.21 In the current study, fibulin-3 had a sensitivity of 21% and mesothelin 56% for MM, at a specificity of 95%. The observation that nearly half of MM patients have elevated blood levels of mesothelin within 1 month of diagnosis has previously been reported in independent samples from the same centre.8 No improvement in diagnostic accuracy over mesothelin alone was obtained when the two markers were combined.
Despite differences in sensitivities between the previous9 and current study, both found that plasma fibulin-3 levels were elevated in MM patients relative to other cancers. This finding may be associated with the tissue distribution of fibulin-3, which was previously found to be expressed at relatively high levels in normal lung tissue,25 or the regulation of expression, as fibulin-3 is downregulated in epithelial-derived tumours compared with matching tissue.26 However, previous studies have not specifically compared expression between mesothelial cells and other tissues, malignant or benign. Pass et al9 found all 26 MM tumours examined expressed fibulin-3, but expression varied between the cytoplasm and nucleus in different samples.
As observed previously,9 there was no correlation between plasma and effusion fibulin-3 concentrations. However, effusion fibulin-3 was not specific for MM in the current study, as opposed to the high sensitivity of 84% at a 92% specificity observed in the above study. Our study found elevated fibulin-3 in over half of the effusions of benign aetiology. Preliminary analysis did not determine a common clinical pattern of these fibulin-3 positive benign effusion samples although there was an indication of a correlation with effusion LDH. Further studies would be required to elucidate the basis of the discrepancy between the previous and current studies.
The prognostic potential of fibulin-3 was also examined and compared with mesothelin. Neither effusion or plasma mesothelin concentration nor plasma fibulin-3 was a significant predictor of survival in the MM patients in this study. The individual prognostic significance of age, sarcomatoid histology and poor performance status was, however, observed. EORTC and CALGB prognostic groups, while trending appropriately, were not significant, possibly due to small numbers and missing data. As previously reported, neutrophil to lymphocyte ratio at the time of MM diagnosis had no prognostic value.16 However, higher effusion fibulin-3 concentration was a significant negative predictor of survival. This may be because of higher concentrations of fibulin-3 in biphasic and sarcomatoid tumours, which generally have a worse prognosis than predominantly epithelioid MM tumours, compared with mesothelin, which is largely restricted to the latter histological type. Effusion fibulin-3 may therefore be useful as a biomarker for these subtypes of MM once a diagnosis of MM had been made by other means.
In conclusion, this study confirmed that fibulin-3 is increased in the plasma of MM patients but at a lower diagnostic sensitivity than previously reported9 and inferior to that of mesothelin in both plasma and effusions. Therefore, mesothelin remains the most useful biomarker for the diagnosis of MM and the biomarker to which future biomarker candidates should be compared. Effusion levels of fibulin-3 were prognostic for MM survival and further investigation of fibulin-3 is warranted as an understanding of its biological role in this tumour may result in new insights into the treatment of MM.
Acknowledgments
We would like to thank the staff of PathWest Laboratory Medicine, Sir Charles Gairdner Hospital, Hollywood Hospital and St John of God Pathology for their assistance with this study. The Australian Mesothelioma Tissue Bank is a member bank of the Australian Biospecimen Network which is supported in part by the Australian National Health and Medical Research Council.
References
Footnotes
-
Contributors JC: (principal contributor and guarantor) study coordinator, study conception, data acquisition, data analysis, data interpretation, drafting of the manuscript review and approval of the manuscript. IMD and TMM: data analysis, data interpretation, drafting of the manuscript review and approval of the manuscript. SLL, JL and YD: data acquisition, review and approval of the manuscript. AS and AWM: data acquisition and interpretation, review and approval of the manuscript. YCGL and BWSR: study conception, data acquisition, data interpretation, drafting of the manuscript review and approval of the manuscript. SJS: data analysis interpretation, review and approval of the manuscript. AKN: data acquisition, data interpretation, drafting of the manuscript review and approval of the manuscript.
-
Funding National Health and Medical Research Council (1063067).
-
Competing interests None.
-
Ethics approval The human ethics committees of Sir Charles Gairdner Hospital and Hollywood Hospital, Perth, Western Australia.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All data from the study are published.
Linked Articles
- Airwaves
- PostScript
- PostScript