Article Text

Statistics from Altmetric.com
A 70-year-old woman with a history of bronchiectasis diagnosed with bilateral pulmonary nodules was examined. She was a non-obese (body mass index: 18.3 kg/m2), non-diabetic never-smoker. The pulmonary nodules had been present for 4 years. Chest CT revealed multiple, well-defined and homogenous subcentimetre nodules of variable sizes scattered in the left and right lungs. The average nodule was –150 Hounsfield units (HU) with a density slightly less than muscle and similar to fat (HU: –50 to –200). The follow-up chest CTs with an interval of 4 years demonstrated slight growth of those pulmonary nodules (figure 1). Video-assisted thoracoscopic lung biopsies were performed on the left side. Two small pieces of lung tissue containing pulmonary nodules were wedge-resected from different lobes. Multiple yellowish and well-defined nodules up to 0.7×0.6×0.5 cm were found. Upon microscopic analysis, the resected lung tissues were found to contain multiple foci of lipomatous tumours, which are composed of lobules of mature adipose tissue (figure 2). The term ‘Intrapulmonary lipomatosis’ is therefore used to describe the clinical entity of the currently presented case.

Multiple, well-defined and homogenous, subcentimetre nodules of various sizes scattered in both lungs. The Hounsfield units (HU) of those nodules ranged between –329 and –56.

{kind=link}
{kind=link}
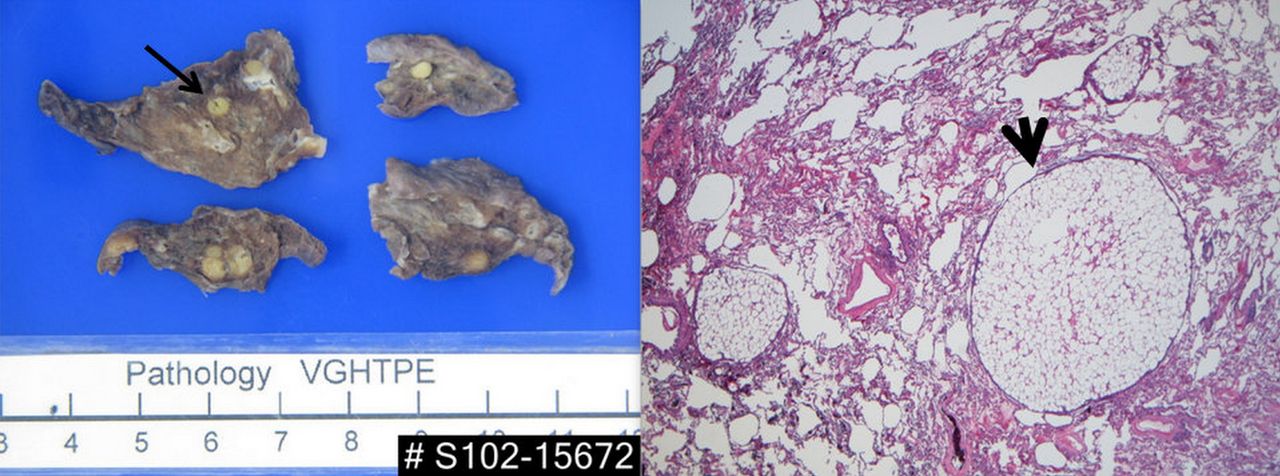
The tissue sample was resected from the left lower lobe of the lung. Multiple small, yellowish and well-defined nodules can be observed in the lung parenchyma (long arrow). Microscopically, lobules of mature adipose tissue with thin intervening fibrous septa were also observed (short arrow). No atypical adipocytes or lipoblasts are found.
Lipomas are one of the most frequently encountered benign neoplasms and are mostly seen in endobronchial trees. Intrathoracic lipomas are rare and lipomas in the lung parenchyma, also termed peripheral intrapulmonary lipoma, are extremely rare. From the first reported case in 1911, only 15 cases of peripheral intrapulmonary lipoma have been reported.1 All lipomas have been diagnosed as solitary pulmonary lesions. To the best of our knowledge, case of multiple intrapulmonary lipomas has not been reported in the literature. From a radiological perspective, a lipoma may be mistaken for an infectious disease, or a primary or secondary malignant lesion, but analysis using CT scan may provide valuable insight into the diagnosis when a well-defined, homogeneous, fat dense lesion is seen.2 In addition to lipomas, the differential diagnoses of fat-containing pulmonary nodules can be numerous, such as fibrolipomatous harmatoma, liposarcoma, thymolipoma, angiomyolipoma with adipocytic overgrowth and metastasising lipoleiomyomas.1 However, the nodules in the currently presented case contained no other element of soft tissue or calcium and the overall nature of the disease has not been aggressive. Taken together, malignancy was unlikely and early surgical intervention was not needed. This case report illustrates that intrapulmonary lipomatosis, although extremely rare, can be a diagnostic possibility when encountering multiple bilateral pulmonary nodules.
Learning points
-
Intrapulmonary lipomatosis should be considered in the differential diagnosis of multiple pulmonary nodules despite its rare incidence.
-
Radiological features and the clinical course of disease can support the diagnosis of intrapulmonary lipoma. However, surgical intervention for tissue diagnosis remains the treatment of choice when pulmonary nodules of an undetermined source are discovered.
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The second author's name has been amended to read Yu-Chao Yu.
-
Contributors T-YC and Y-HW provided the pathology image and information regarding the presented case.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves