Article Text

Statistics from Altmetric.com
- Atypical mycobacterial infection
- pneumonia
- tuberculosis
- opportunist lung infections
- respiratory infection
A middle-aged individual of Ethiopian origin attended the emergency department with haemoptysis. The patient had no other significant medical problems and had not travelled for several years. The patient drank moderately and did not smoke but later admitted to chewing khat (a narcotic leaf) frequently over the past 6 months.
There were no significant findings on physical examination. Renal and liver function tests and C reactive protein were within normal limits, but a peripheral blood eosinophilia was noted (2.1×109/l). Serological tests for HIV, hepatitis B and C were negative. A poorly defined opacity was seen in the right lung on chest x-ray, and a subsequent CT scan showed an area of consolidation with cavitation (see figure 1). An incidental finding of low-attenuation subcapsular lesions in the part of the liver imaged on this scan was also noted.

Contrast-enhanced CT chest: consolidation seen in the right lower lobe, with the suggestion of early cavitation (arrow).
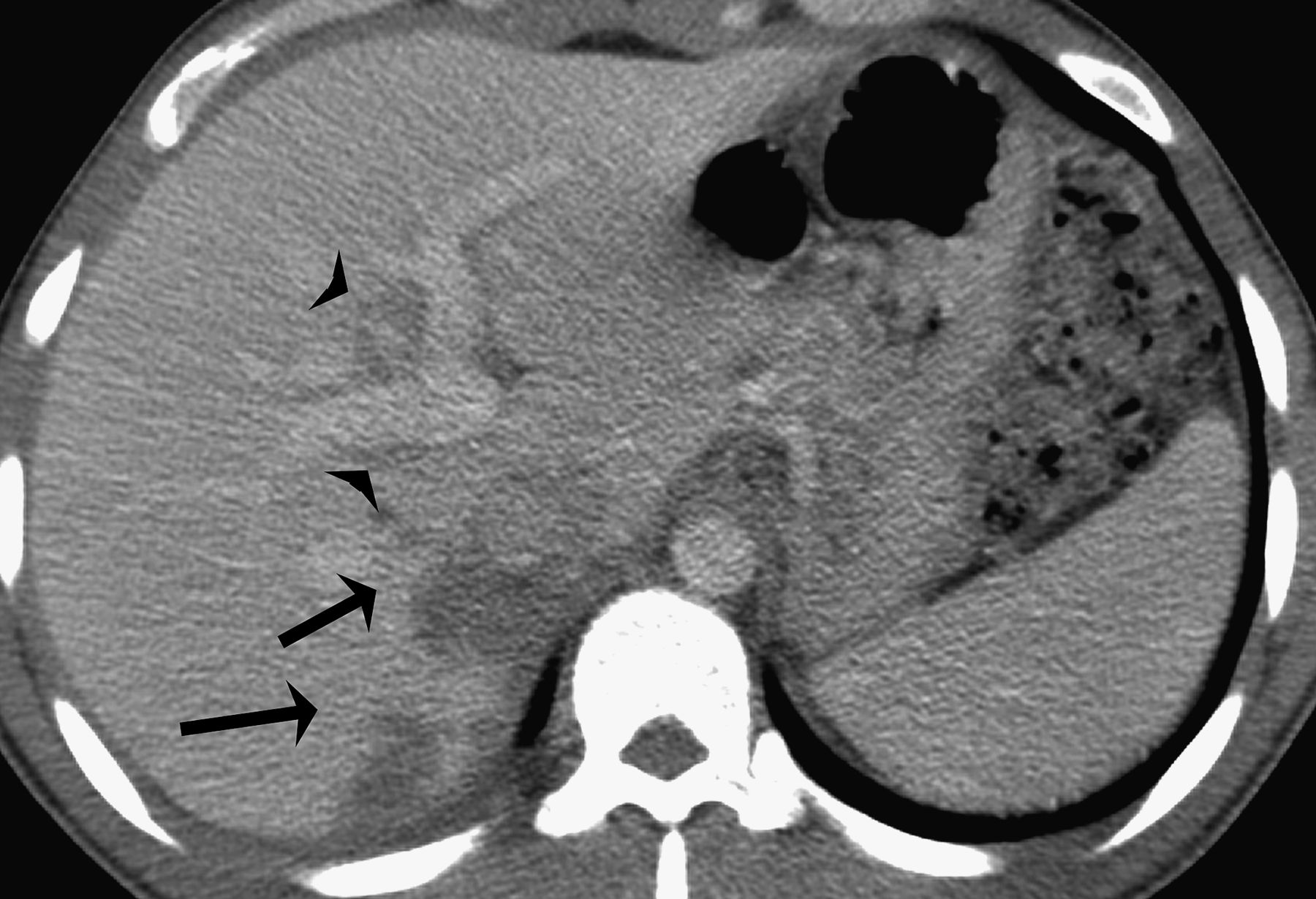
The patient was referred to the chest clinic for investigation of possible tuberculosis, but sputum cultures were negative for mycobacteria. On review two months later, the haemoptysis and the radiological findings had worsened. The eosinophil count remained raised. An abdominal CT scan revealed multiple low-density tracking liver lesions (figure 2). A serological test was performed.
{kind=link}
{kind=link}
Axial contrast-enhanced CT abdomen: There are multiple low-attenuation lesions seen in the subcapsular region (arrows) extending towards the porta hepatis. Mild intrahepatic bile duct dilatation is seen (arrowheads).
Question
See page 306
Answer
From question on page 305
Diagnosis: pulmonary fascioliasis
Fascioliasis occurs following ingestion of aquatic plants contaminated with encysted metacercariae of Fasciola spp. The parasites migrate to the liver after hatching in the bowel and grow into adult flukes. Egg production commences after several months, with excretion via the biliary tract into the faeces. A developmental cycle in the intermediate host (a freshwater snail) then results in contamination of further plants by metacercariae and a new cycle of infection.
Fasciola is found worldwide, and outbreaks associated, particularly, with the consumption of watercress have been well documented. An association with the chewing of khat has also been noticed.1 Khat is the leaf of the shrub Catha edulis. It has a mild narcotic effect when chewed and, although not illegal in most European states, its use is limited to certain ethnic communities.2 Khat may become contaminated when sprinkled with water to keep it fresh during transport.3
Fasciola usually affects only the liver but, as with all flukes, aberrant migration can lead to disease in a variety of organs. There are reports of Fasciola causing pleural effusions, pneumothorax and pulmonary lesions.4 ,5 Other flukes, such as Paragonimus and Schistosoma can also cause lung lesions. When there is an epidemiological risk, it is important to consider these unusual pathogens to avoid subjecting patients to unnecessary antituberculous therapy or surgery. In our case, the diagnosis was made on serological testing of serum (Fasciola IFAT 1:128) and review of the liver imaging, which showed tracking lesions suggestive of Fasciola migration. The patient was treated with 700 mg of triclabendazole twice. Two months later, the chest x-ray abnormalities had improved, the eosinophil count was within normal limits and the haemoptysis had completely resolved.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.