Article Text

Abstract
Rationale Upregulation of glucocorticoid receptor β (GRβ) has been implicated in steroid resistance in severe asthma, although previous studies are conflicting. GRβ has been proposed as a dominant negative isoform of glucocorticoid receptor α (GRα) but it has also been suggested that GRβ can cause steroid resistance via reduced expression of histone deacetylase 2 (HDAC2), a key regulator of steroid responsiveness in the airway.
Objectives To examine GRβ, GRα, HDAC1 and HDAC2 expression at transcript and protein levels in bronchial biopsies from a large series of patients with severe asthma, and to compare the findings with those of patients with mild to moderate asthma and healthy volunteers.
Methods Bronchoscopic study in two UK centres with real-time PCR and immunohistochemistry performed on biopsies, western blotting of bronchial epithelial cells and immunoprecipitation with anti-GRβ antibody.
Measurements and main results Protein and mRNA expression for GRα and HDAC2 did not differ between groups. GRβ mRNA was detected in only 13 of 73 samples (seven patients with severe asthma), however immunohistochemistry showed widespread epithelial staining in all groups. Western blotting of bronchial epithelial cells with GRβ antibody detected an additional ‘cross-reacting’ protein, identified as clathrin. HDAC1 expression was increased in patients with severe asthma compared with healthy volunteers.
Conclusions GRβ mRNA is expressed at low levels in a minority of patients with severe asthma. HDAC1 and HDAC2 expression was not downregulated in severe asthma. These data do not support upregulated GRβ and resultant reduced HDAC expression as the principal mechanism of steroid resistance in severe asthma. Conflicting GRβ literature may be explained in part by clathrin cross-reactivity with commercial antibodies.
- Glucocorticoid receptor β
- clathrin
- histone deacetylase
- bronchial biopsy
- severe asthma
- airway epithelium
- asthma
- asthma mechanisms
- COPD mechanisms
- α1 antitrypsin deficiency
- cystic fibrosis
- cytokine biology
- emphysema
- innate immunity
- lung proteases
- macrophage biology
- neutrophil biology
- asthma genetics
- COPD pathology
- bronchoscopy
- lung cancer
- COPD exacerbations
- cough/mechanisms/pharmacology
- allergic lung disease
- asthma pharmacology
- eosinophil biology
- asthma guidelines
- COPD epidemiology
Statistics from Altmetric.com
- Glucocorticoid receptor β
- clathrin
- histone deacetylase
- bronchial biopsy
- severe asthma
- airway epithelium
- asthma
- asthma mechanisms
- COPD mechanisms
- α1 antitrypsin deficiency
- cystic fibrosis
- cytokine biology
- emphysema
- innate immunity
- lung proteases
- macrophage biology
- neutrophil biology
- asthma genetics
- COPD pathology
- bronchoscopy
- lung cancer
- COPD exacerbations
- cough/mechanisms/pharmacology
- allergic lung disease
- asthma pharmacology
- eosinophil biology
- asthma guidelines
- COPD epidemiology
Key messages
What is the key question?
Increased glucocorticoid receptor β (GRβ) with resultant reduction in histone deacetylase 2 (HDAC2) expression has been implicated in the pathogenesis of severe steroid-resistant asthma, but previous data are conflicting.
What is the bottom line?
GRβ mRNA was expressed at very low levels in the airways of a minority of patients with severe asthma. GRβ immunostaining was prominent in bronchial biopsies from all patients, but this was subsequently shown to be due to antibody cross-reactivity with heavy chain clathrin. No reduction in HDAC2 expression was identified in severe asthma.
Why read on?
These data do not support altered GRβ/HDAC expression as the principal underlying mechanism of steroid resistance in severe asthma. Some of the discrepancies in the GRβ literature may be explained by clathrin cross-reactivity with commercial antibodies.
Introduction
Patients with severe asthma respond poorly to available therapies, which results in high healthcare costs due to unscheduled healthcare visits, treatment of co-morbidities and work absence.1 The cornerstone of asthma treatment is glucocorticoid therapy; however patients with severe asthma are relatively resistant to inhaled glucocorticoids, often resulting in a requirement for systemic steroids to maintain disease control.2
Proposed molecular mechanisms for glucocorticoid resistance include abnormalities of glucocorticoid binding,2–4 reduced glucocorticoid receptor nuclear translocation in response to steroids,5 6 increased expression of pro-inflammatory transcription factors (eg, activator protein-1 and nuclear factor-κB)7 8 and altered expression of co-repressor proteins (eg, histone deacetylases).9 Two commonly proposed mechanisms for steroid resistance in severe asthma are increased expression of the dominant negative isoform of the glucocorticoid receptor, glucocorticoid receptor β (GRβ), and reduced expression and activity of histone deacetylase 2 (HDAC2).3 5 A recent study suggested the reduced HDAC2 in severe asthma may be regulated by GRβ overexpression.10
Existing data on GRβ expression in severe asthma have been variable. GRβ-immunoreactive peripheral blood mononuclear cells (PBMCs), CD3 T cells and bronchoalveolar lavage cells were increased in steroid-resistant asthma.3 11 12 Furthermore, Sousa et al reported increased GRβ-positive cells in steroid-resistant asthmatic tuberculin responses.13 In the lungs of patients who have died from asthma increased GRβ immunoreactivity has been reported,14 and in the only published bronchial biopsy study, GRβ expression detected by immunohistochemistry was increased in the epithelium and submucosa of patients with severe asthma.15 However, other studies in PBMCs in severe asthma have been negative.16 17 Thus, it remains unclear if GRβ is elevated in the airways of severe asthma (and other ‘steroid resistant’ conditions) and why there is such variability in the published literature.
Our aims were to examine GRβ and GRα expression at transcript and protein levels in bronchial biopsies from a large series of patients with severe asthma, and to compare the findings with those for patients with mild to moderate asthma and healthy volunteers. We also studied HDAC1 and HDAC2 expression in matched biopsies.
Methods
Subjects
This study was performed in two UK centres, Queens University Belfast and University of Leicester. Patients with severe asthma were recruited from the Belfast City Hospital and Glenfield Hospital, Leicester Difficult Asthma Services, where systematic evaluation protocols ensure patients have well characterised severe asthma as defined by current American Thoracic Society guidelines.18 All patients had persisting symptoms despite treatment at step 4 or 5 of the Global Initiative for Asthma (GINA) guidelines.19 Patients with mild to moderate asthma and healthy volunteers were recruited from hospital clinics or by advertisement.
In total, 27 participants were recruited from Belfast (10 healthy volunteers (HV), 7 patients with mild to moderate asthma (MA) and 10 patients with severe asthma (SA)) and 56 participants from Leicester (12 HV, 23 MA and 21 SA) (table 1).
Demographic characteristics of patients with asthma and healthy volunteers (Belfast and Leicester cohorts combined)
Bronchoscopy
Bronchoscopy was performed using standard techniques (see online supplement). Biopsies were either placed immediately in RNA preservative (RNAlater, Ambion, Austin, Texas, USA) and submitted for real-time PCR (qPCR) or placed into dry acetone containing protease inhibitors (iodoacetamide and phenylmethylsulfonyl fluoride) and fixed overnight at −20°C for immunohistochemistry. Brushings were placed in Promocell medium containing penicillin/streptomycin and Primocin for cell culture (Promocell, Heidelberg, Germany).
Gene expression analysis
qPCR analysis was performed using RNA from homogenised bronchial biopsies (74 biopsies; 22 HV, 28 MA and 24 SA) using TaqMan® Gene Expression Assays (Applied Biosystems, Foster City, California, USA). RNA purification and qPCR quality control are detailed in the online supplement. Relative expression levels were determined by the 2(-DeltaDelta CT) method, as described in Applied Biosystems User Bulletin No. 2 (P/N 4303859).20
Bronchial biopsy immunohistochemistry and confocal microscopy
For immunohistochemistry, biopsy samples were processed and stained using local protocols. Fifty-five biopsies (17 HV, 21 MA and 17 SA) were processed for immunohistochemistry. Infiltration and embedding with JB4 resin was performed.21 The immunohistochemical technique and confocal analysis are detailed in the online supplement.
Immunostained sections were evaluated by two independent assessors with consensus scoring for any conflicting results (scoring system given in the online supplement). Two polyclonal anti-GRβ antibodies were compared, ab3581 (Abcam, Cambridge, UK) and PA3-514 (Affinity Bioreagents, Golden, CO, USA via Pierce Biotechnology, Rockford, IL, USA) along with anti-GRα (sc-1002), HDAC1 (sc-7872) and HDAC2 (sc-7899) (Insight Biotechnology, Wembley, UK).
Epithelial cell culture and western blotting
Bronchial epithelial brushings (Belfast cohort) were cultured (Promocell) and lysates (NE-PER lysis kit, Pierce Biotechnology, MSC, Dublin) used for western blot experiments (see online supplement). For clathrin identification blots, anti-clathrin antibody (ab2731, Abcam) was used. For immunoprecipitation, BEAS-2B cells (ATCC, Manassas, VA, USA) were also used following culture in supplemented Dulbecco's Modified Eagle's Medium (Gibco-Invitrogen Ltd, Paisley, UK).
Immunocytochemistry
Primary bronchial epithelial cells (PBECs) were grown onto collagen-coated Thermanox coverslips (catalogue no. 174950, Nalge Nunc International, Rochester, NY, USA), permeabilised and stained (see online supplement), and mounted on slides.
Immunoprecipitation
Immunoprecipitation was performed using IgA Magnetic Beads (Pierce Biotechnology, Rockford, IL, USA). PBECs and BEAS-2B cells were used. The method is detailed in the online supplement and the resultant blots were probed with anti-GRβ and anti-clathrin (ab2731, Abcam) antibodies. In addition, increasing amounts (250 ng, 500 ng, 1000 ng and 2500 mg) of recombinant clathrin was run on a gel and the blot probed with anti-GRβ and anti-clathrin antibodies.
Proteomics
Protein identification was performed by the Proteomics Facility, University of Dundee, UK. Following immunoprecipitation, gels were stained with Coomassie blue and the higher molecular weight band cut out of the gel, digested with trypsin prior to analysis by one-dimensional nano-scale liquid chromatography tandem mass spectrometry (nLC-MS-MS) and protein identification performed with Mascot (www.matrixscience.com/).
Statistical analysis
The statistical package Prism (GraphPad Prism version 4.00 for Windows, GraphPad Software, San Diego, California, USA) was used to generate graphs and perform appropriate statistical analysis. Data are presented as median (IQR) unless otherwise stated. Between-group data were analysed using one-way analysis of variance (Kruskal–Wallis) with Dunn's post hoc test or Wilcoxon Signed Rank test as appropriate. A p value <0.05 was considered significant.
Results
GRβ, GRα, HDAC1 and HDAC2 mRNA expression
In the samples available for qPCR (n=74), GRβ mRNA was detectable in only 13 of the 74 (18%) participants (seven SA—four of whom were on oral steroids, four with moderate persistent asthma on inhaled steroids, one with steroid-naive asthma and one HV) (figure 1A). There was a similar rate of detection in the SA group (p=0.10, Fisher's exact test). Despite the use of different specific primer-probe sets for GRβ, GRβ mRNA was not detected in any of the other samples. GRα mRNA was detectable in 70 of the biopsy samples (figure 1B, median (IQR) relative fold expression of GRα mRNA expression was 343.7 (137.4–928.2), 498.4 (200.4–1439) and 463.1 (186.3–1349) in HV, MA and SA groups respectively, p=0.62, Kruskal–Wallis). HDAC1 mRNA was significantly upregulated in the SA group compared with the HV group (figure 1C, HDAC1—median (IQR) relative fold expression was 0.08 (0.04, 0.21), 0.22 (0.09, 0.49) and 0.27 (0.10, 0.94) in the HV, MA and SA groups respectively (p=0.02, Kruskal–Wallis, post hoc analysis p<0.05 between HV and SA). HDAC2 expression did not differ between participant subgroups (figure 1D, HDAC2—median (IQR) relative fold expression was 0.52 (0.14–0.97), 0.63 (0.33–4.29) and 0.76 (0.36–1.97) in the HV, MA and SA groups respectively (p=0.23, Kruskal–Wallis). There was a significant correlation between HDAC2 mRNA and GRα mRNA (figure 3D, Spearman r=0.75, p<0.001).
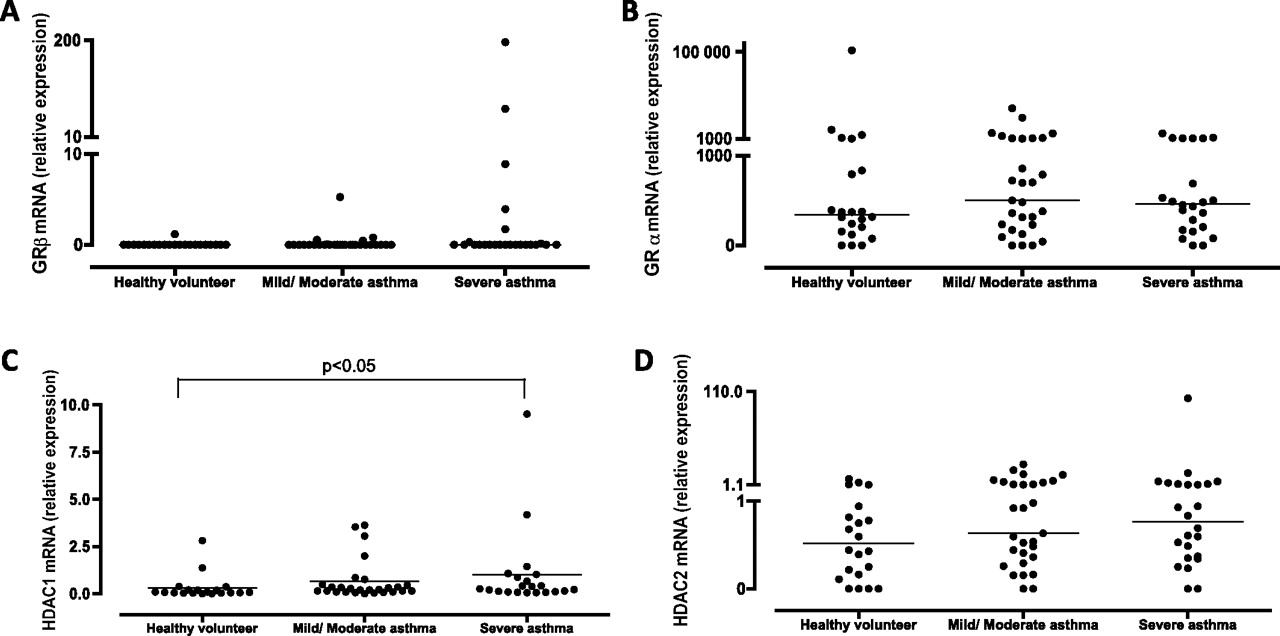
Gene expression in bronchial biopsies (n=74). Values represent fold change in target gene expression with GAPDH as housekeeping gene (2−∆∆Ct). (A) Glucocorticoid receptor β (GRβ) mRNA was detectable in only 13 of 74 samples (seven patients with oral-steroid-dependent asthma, four with moderate persistent asthma on inhaled steroids, one with steroid-naive asthma and one healthy volunteer). (B) GRα mRNA widely expressed in bronchial biopsies. There were no significant between-group differences (p=0.62, Kruskal–Wallis). (C) Histone deacetylase 1 (HDAC1) mRNA expression in bronchial biopsies. HDAC1 was increased in patients with severe asthma compared with healthy volunteers (HDAC1 p=0.02, Kruskal–Wallis, post hoc analysis p<0.05 between healthy volunteers and severe asthma). (D) HDAC2 mRNA expression in bronchial biopsies. There were no significant between-group differences (HDAC2 p=0.23, Kruskal–Wallis).
Immunohistochemistry for GRβ, GRα, HDAC1 and HDAC2 and relation to asthma severity in bronchial biopsies
Similar location and intensity of immunostaining for GRβ was seen using both immunohistochemistry protocols (figure 2A). Identical staining was noted with both GRβ antibodies (data not shown). The most striking observation was the intensity of immunostaining in contrast to low mRNA expression. GRβ immunostaining was mainly localised to the epithelium with scant submucosal expression in glands, smooth muscle cells and inflammatory cells (figure 2A,B). Confocal microscopy revealed that epithelial immunostaining with GRβ antibodies was predominantly cytoplasmic, though some cells did demonstrate nuclear staining (figure 2D).

Glucocorticoid receptor β (GRβ) expression in bronchial biopsies; representative immunohistochemistry shown at ×400 magnification. (A) Biopsy from patients with severe asthma, demonstrating the pattern and anatomical localisation of GRβ expression to be identical in both clinical centres. (B) GRβ expression in individual patient groups. (C) Quantitative immunohistochemical epithelial expression for GRβ in bronchial biopsies. There was no significant difference between groups (p=0.18, Kruskal–Wallis). (D) Immunostaining with GRβ antibody (ab3581) using confocal microscopy in bronchial biopsy from a patient with severe asthma, demonstrating diffuse epithelial staining with scattered submucosal reactivity (×400 magnification).
There was no significant between-group difference in epithelial GRβ immunostaining (figure 2C, p=0.18, Kruskal–Wallis). Figure 2B shows representative sections from each of the participant groups. Among the 10 patients with mRNA above the limit of detection and matched immunohistochemistry samples, there was no correlation between mRNA levels and epithelial expression of GRβ (data not shown).
Glucocorticoid receptor α (GRα) immunostaining was diffusely present in the epithelium and submucosa with no difference between participant subgroups (data not shown), but GRα immunostaining was more abundant than GRβ immunostaining in all groups.
HDAC1 and HDAC2 immunostaining was also more prominent in the epithelium, with occasional submucosal cells. There was no difference between subgroups (figure 3A–C; HDAC1, p=0.55, Kruskal–Wallis and HDAC2, p=0.89, Kruskal–Wallis). In the SA group, there was no significant difference in mRNA or protein expression for HDAC1 and HDAC2 between those taking theophyllines and those who were not (data not shown).
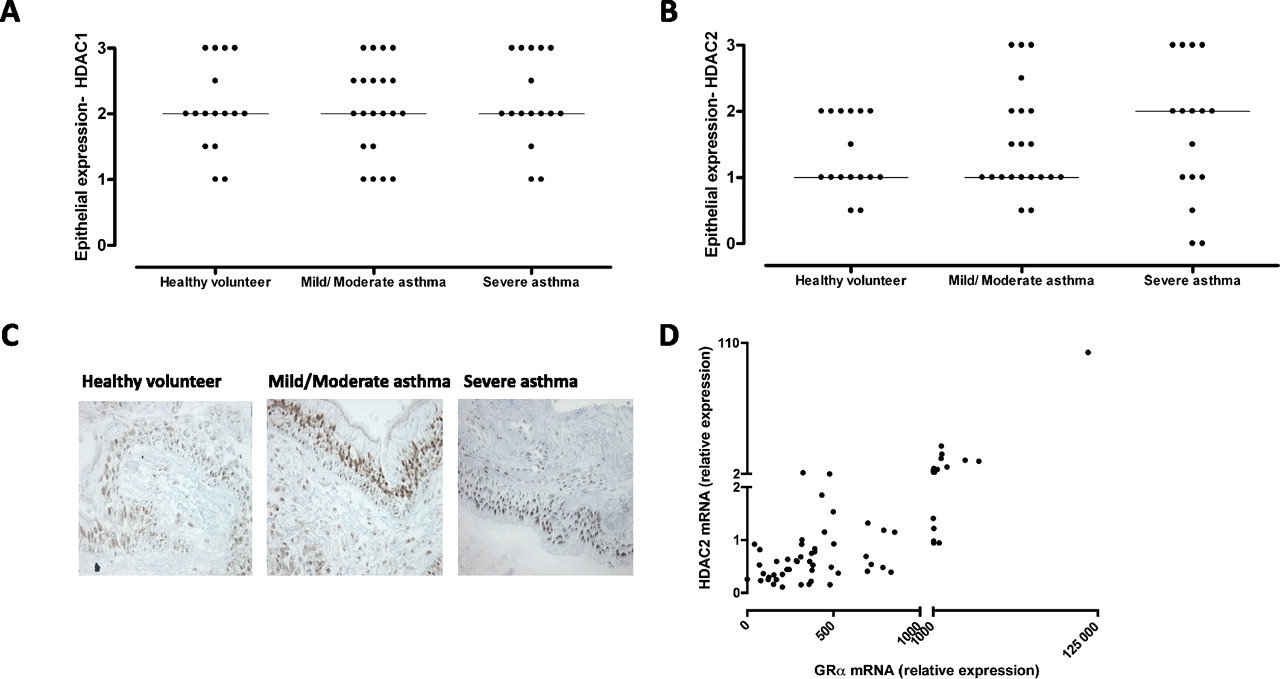
Immunohistochemical epithelial expression for histone deacetylase 1 (HDAC1) and HDAC2 in bronchial biopsies. (A) HDAC1: there was no significant difference between groups (p=0.55, Kruskal–Wallis); (B) HDAC2: there was no significant difference between groups (p=0.89, Kruskal–Wallis). (C) HDAC2 expression in individual patient groups—representative immunohistochemistry shown at ×400 magnification. (D) Highly significant correlation between glucocorticoid receptor α (GRα) and HDAC2 mRNA.
Western blot analysis and immunocytochemical analysis of PBEC lysates
Immunocytochemical analysis of cultured PBECs revealed predominantly cytoplasmic location of GRβ with some cells demonstrating concomitant nuclear expression (figure 4A). In view of the ‘dissociation’ between mRNA levels of GRβ and immunohistochemical staining, further analysis of GRβ-antibody specificity was performed using western blots of cultured PBECS. This consistently demonstrated two bands (figure 4B); one band was identified at the anticipated molecular weight of GRβ at 90 kDa but a second higher molecular weight band (∼180 kDa, band 2) was consistently present on the PBEC blots and always stronger than the GRβ band in both nuclear and cytoplasmic compartments (figure 5, online supplement).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Immunocytochemical analysis of primary bronchial epithelial cells from a healthy volunteer showing predominantly cytoplasmic glucocorticoid receptor β (GRβ) expression with occasional cells demonstrating nuclear expression (arrowed). (B) Typical western blot showing GRβ band (at around 90 kDa) and higher molecular weight band (band 2) at 180 kDa in primary bronchial epithelial cells. (C) Recombinant clathrin (250–2500 ng) was immunoblotted with (i) anti-clathrin antibody (1:1000 in 5% milk) and (ii) anti-GRβ antibody (1:500 in 3% bovine serum albumin (BSA)). Similar bands were noted in the anti-GRβ and anti-clathrin probed gels at 180 kDa. (D) Gene expression for clathrin in bronchial biopsies. There was no significant difference between patient groups noted.
To evaluate the 180 kDa band, immunoprecipitation using both GRβ antibodies was performed using BEAS-2B cells (where the 180 kDa band was also identified) and PBEC lysates. The higher molecular weight bands were cut out of the gel and sequenced. In both BEAS-2B cells and PBECs, this identified heavy chain clathrin as the 180 kDa protein.
To further confirm that clathrin was responsible for band 2, recombinant clathrin was run on a gel and probed separately with anti-GRβ and anti-clathrin antibodies (figure 4C). Both antibodies identified the clathrin protein, confirming this band was clathrin and importantly both anti-GRβ antibodies displayed similar bands on western blotting. There was no significant difference in clathrin mRNA expression in bronchial biopsies between groups (figure 4D).
Discussion
This study examined GRβ, HDAC1 and HDAC2 gene expression and protein in the largest cohort of patients with severe asthma to date. We demonstrated low levels of GRβ mRNA expression in bronchial biopsies from a minority of patients with severe asthma despite prominent immunostaining in matched tissue sections. GRβ is upregulated at the transcriptional level by steroid exposure in an airway epithelial cell line22 and of the 13 participants in the present study in whom GRβ mRNA was detectable, 11 were on inhaled steroids; however, in the majority of patients with asthma on steroid therapy, GRβ was not detectable. No previous study has reported the existence of a 180 kDa band on western blot with commercially available GRβ antibodies, which we have subsequently identified as heavy chain clathrin. Therefore it is impossible to comment with confidence on the distribution of GRβ using these antibodies.
Previous data suggested predominantly nuclear expression of GRβ, though cytoplasmic expression has been reported.23 Clathrin is a ubiquitous protein complex involved in transport vesicle formation to mediate endocytosis of transmembrane receptors,24 and given the low GRβ mRNA expression in a few patients, we believe that cross-reactivity with clathrin resulted in prominent biopsy staining. The only other bronchial biopsy study in severe asthma reported significant upregulation of GRβ in bronchial biopsies from patients with severe asthma.15 Their pattern of staining was similar to that reported here but tissue expression of GRβ at the mRNA level was not examined. Other studies examining GRβ expression in severe asthma using these antibodies have reported variable associations. GRβ immunoreactivity was increased in PBMCs and bronchoalveolar lavage (BAL) cells from patients with severe asthma.3 12 25 However, another PBMC study was unable to identify any GRβ immunoreactivity in healthy volunteers and patients with asthma that is steroid sensitive or resistant.16 Of note, that study was unable to identify GRβ mRNA in the first round of PCR, though it did on the second cycle of nested PCR.16 A further PBMC study by Torrego et al reported 600-fold lower GRβ mRNA expression than GRα, but that group was also unable to detect any GRβ expression on western blot.17 Goleva et al demonstrated readily appreciable GRβ expression using immunohistochemistry in BAL macrophages but demonstrated only femtograms of GRβ mRNA.12
In other inflammatory disease states, such as glaucoma, ulcerative colitis and rheumatoid arthritis, GRβ expression has been reported to be upregulated in glucocorticoid-unresponsive disease, although again there is controversy.26–30 Some of these studies have looked at mRNA expression from PBMCs rather than immunohistochemistry. For example, GRβ mRNA was detectable in PBMCs from patients with glucocorticoid-resistant ulcerative colitis compared with low detection in glucocorticoid-responsive disease and healthy volunteers.27 This same group also demonstrated elevated PBMC GRβ mRNA in patients with active ulcerative colitis compared with inactive disease or Crohn's disease, though this was disputed by Hausmann et al, who did not find elevated PBMC GRβ mRNA in relation to steroid resistance.26 29 PBMC GRβ mRNA and GRβ-positive PBMCs were increased in steroid-resistant rheumatoid arthritis.28 Zhang et al were able to confirm that glaucomatous trabecular meshwork cells expressed lower levels of GRβ protein by western blotting and these cells were more sensitive to the effects of steroids compared with normal trabecular meshwork cells.30 A recent immunohistochemistry study by Ishida et al reported increased GRβ expression in patients with severe allergic rhinitis compared with healthy controls, and of note, GRβ mRNA was not assessed in this study.31
Our data suggest that tissue immunohistochemistry with these GRβ antibodies is unreliable due to concomitant clathrin staining. This illustrates the problems associated with using antibodies for immunohistochemistry in the absence of validation with other methods, for example, mRNA expression and target protein specificity using western blots. If multiple bands are seen on western blot from the target tissue, we would suggest that this antibody may be inappropriate for use in immunofluorescence, immunocytochemistry or immunohistochemistry. These techniques have been widely used in the GRβ literature and this study questions the validity of previous immunohistochemical and immunocytochemical data utilising these antibodies and supports the need for western blotting techniques. In view of the low mRNA signal compared with that for GRα, we would further conclude that GRβ is not highly expressed in the airways of patients with severe asthma. Given the substantially higher expression of GRα, GRβ is unlikely to function as a dominant-negative isoform of GRα and this mechanism has little to do with the relative steroid resistance seen in this group.
Another proposed mechanism for the induction of steroid resistance by GRβ is reduced tissue expression of HDAC2 mRNA and recent data suggested reduced HDAC2 in severe asthma may be regulated by GRβ overexpression. If this mechanism of HDAC2 regulation is correct, then our data provide no support that it is relevant in severe asthma because, consistent with the low levels of GRβ expression in severe asthma biopsies, we identified no reduction in HDAC2 expression in matched biopsies from the same patients when compared with normal controls and patients with mild to moderate asthma. Reduced HDAC2 tissue expression has been described in patients with chronic obstructive pulmonary disease (COPD) and those who smoke and is associated with reduced HDAC function,32 33 but the data in asthmatic airway samples are conflicting. One study suggested decreased expression of HDAC1 and HDAC2 in mild asthma which increased with steroid treatment.34 In more severe asthma, Bergeron et al reported similar HDAC2 expression between patients with asthma that is steroid resistant and steroid responsive,15 whereas another study reported reduced HDAC2 mRNA expression in BAL cells.10 Importantly, in previous studies in which HDAC mRNA data have been presented along with functional HDAC activity, when there has been a reduction in HDAC activity, there has been a concomitant reduction in HDAC mRNA.34 Thus, there has been no suggestion that reduced HDAC function in asthma or COPD disease is due to any specific alteration in HDAC function, but rather reduced activity is due to reduced tissue expression. Therefore, we believe it is reasonable to conclude that an absence of reduction of HDAC1 and HDAC2 in this large cohort of patient with refractory asthma argues against this being the mechanism of steroid resistance in this patient group.
At a transcriptional level, we found HDAC1 was increased in patients with severe asthma on higher dose steroid treatment compared with healthy volunteers but not those with mild to moderate asthma, which is consistent with the previously described steroid effect of upregulating HDAC1.35 However, this difference appeared small compared with milder disease and no difference was identified in HDAC1 protein expression. Thus, even if HDAC1 is upregulated by steroid treatment, the fact that many patients with severe asthma remain dependent on oral steroids suggests that this upregulation does not enhance steroid efficacy in this group. There was no association between HDAC2 and theophylline treatment, suggesting that the normal HDAC2 levels in severe asthma are not due to theophylline treatment, as has previously been suggested.36 37 The close correlation of HDAC2 with GRα expression at the transcriptional level suggests that these molecules are co-regulated, with increased expression of both molecules tending to increase steroid responsiveness. We did not specifically examine bronchoalveolar macrophages in the present study and thus a reduction in HDAC2 activity in macrophages contributing to steroid resistance cannot be completely excluded. However, other important and relevant immunological mechanisms in asthma pathogenesis have been identified in proximal airway samples obtained at bronchoscopy.
In conclusion, we have demonstrated that commercially available GRβ antibodies cross-react with clathrin and are unreliable for the analysis of GRβ expression in situ. GRβ mRNA was expressed at low levels in the airways with no difference between steroid-sensitive and severe disease. Our findings may explain the discrepant reports for the role of GRβ in steroid-resistant states in a variety of diseases, and do not support the view that GRβ plays a role in severe asthma. In addition, our data suggest that downregulation of HDAC1 or HDAC2 does not occur in severe asthma, and so the mechanism of relative steroid resistance in severe asthma remains unclear.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding CB was supported by a grant from the Northern Ireland Chest, Heart and Stroke Association (reference no. 200645). Research in Leicester was conducted in laboratories and was part funded by ERDF #05567 and supported by a grant-in-aid from Genentech Inc., South San Francisco, California, USA.
Correction notice This article has been corrected since it was published Online First. The corresponding author is affiliated to Centre for Infection and Immunity, Health Sciences Building, Queens University Belfast, Belfast, UK only.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves