Article Text

Abstract
Background Haemodynamic measurements may be superior to the 6-min walk distance (6MWD) as outcome measures in pulmonary hypertension (PH) as they are directly linked to the mechanisms of disease and are not subject to a ceiling effect. The aim of this study was to determine if treatment response in precapillary PH could be detected by pulmonary blood flow (PBF) and stroke volume (SV) measured non-invasively by the inert gas rebreathing (IGR) method at rest and during submaximal constant-load cycle exercise.
Methods Twenty-four patients with precapillary PH receiving de novo or modified disease-targeted therapy were studied. Isotime metabolic variables, PBF and SV were measured at rest and during constant-load cycle exercise at 40% maximal work rate alongside conventional outcome variables, at baseline and after 3 months of new therapy.
Results At follow-up there was a significant increase in PBF (supine rest: mean 0.7±SD 0.9 l/min, erect rest: 0.7±0.8 l/min, exercise: 0.8±1.0 l/min, p<0.005) and SV (supine rest: 7±10 ml, erect rest: 10±11 ml, exercise: median 6 (IQR 3–11) ml, p<0.005). There was a trend for 6MWD to increase by 17±42 or 29 (13–47) m (p=0.061), whereas WHO functional class, N-terminal pro-brain natriuretic peptide or Cambridge Pulmonary Hypertension Outcome Review score were unchanged. In patients with higher baseline 6MWD, IGR measurements were more sensitive than 6MWD in detecting treatment response.
Conclusions Non-invasive IGR haemodynamic measurements could be used to detect treatment response in patients with precapillary PH and may be more responsive to change than 6MWD in fitter patients.
- Exercise
- haemodynamics
- hypertension
- pulmonary
- primary pulmonary hypertension
Statistics from Altmetric.com
Key messages
What is the key question?
Haemodynamic measurements by the inert gas rebreathing method are potential alternative outcome measures in precapillary pulmonary hypertension.
What is the bottom line?
They could be used to measure treatment response.
Why read on?
In addition, they appear to be more sensitive to change than 6-min walk distance in fitter patients.
An impaired exercise stroke volume (SV) and consequently cardiac output (CO) response is the fundamental pathophysiological consequence of pulmonary arterial hypertension (PAH).1 Disease-targeted therapy is aimed at reducing pulmonary vascular resistance, thereby improving CO response to exercise. Measurement of CO at right heart catheterisation (RHC) would allow direct monitoring of disease progression and treatment response, but serial RHC is inconvenient in clinical practice owing to its invasive nature. As a result, 6-min walk distance (6MWD), a measure of functional exercise capacity, has been used as a simple surrogate marker of exercise CO and has been established as the primary end-point in most clinical trials of PAH therapy.2 However, several drawbacks exist which may compromise the reliability of this test as an outcome measure, such as subject volition, comorbid respiratory and musculoskeletal abnormalities, and a ceiling effect in its ability to detect clinical change in fitter patients.3 4 Additionally, it is subject to a learning effect.5
Measurement of CO by the inert gas rebreathing (IGR) method could be an alternative outcome measure to 6MWD. It is a direct measurement of haemodynamics and is hence disease-specific. CO is not subject to a ceiling effect due to its linear relationship with peak oxygen uptake and so, when combined with exercise, may be more sensitive than 6MWD in detecting early change in fitter patients.6 As stroke volume (SV) reaches its maximum at around 40–50% maximal work rate,7 maximal SV could be measured during submaximal constant-load exercise to give an objective measurement independent of patient effort. This form of exercise would also allow isotime comparison of metabolic variables which were shown to be more sensitive than variables measured at peak exercise in demonstrating improved exercise capacity from therapeutic interventions in chronic obstructive pulmonary disease.8–10 CO measured non-invasively by acetylene rebreathing using a mass spectrometer and by rebreathing of nitrous oxide and sulfur hexafluoride using a more recently developed metabolic system has been validated against the thermodilution and Fick methods in patients with pulmonary hypertension (PH) and interstitial lung disease.11–13
The aims of this study were to determine if the response to disease-targeted therapy in patients with precapillary PH could be detected by changes in IGR haemodynamic measurements and also by isotime comparison of metabolic indices of cardiac function (oxygen uptake and oxygen pulse) and ventilatory efficiency (ventilatory equivalent for carbon dioxide and end-tidal carbon dioxide partial pressure), at rest and during submaximal constant-load cycle exercise.
Methods
Study population
The study was performed in the Scottish Pulmonary Vascular Unit between July 2008 and June 2010. The inclusion criteria were incident patients diagnosed with precapillary PH including WHO group I PAH (except congenital heart disease) and chronic thromboembolic pulmonary hypertension (CTEPH) started on de novo disease-targeted therapy, and prevalent patients in whom disease-targeted therapy was modified. The diagnosis of PH was based on RHC in accordance with contemporary guidelines.14 15 Patients who were unable to perform a 6-min walk test (6MWT) or cardiopulmonary exercise test (CPET) were excluded. Reproducibility of IGR measurements was tested in a subgroup of patients. The study was approved by the West Glasgow research ethics committee and written informed consent was obtained from all participants.
Study design
Study patients underwent a symptom-limited incremental cycle ergometer CPET and a 6MWT at baseline. On a separate day within 2 weeks they performed a second 6MWT and submaximal constant-load CPET with IGR measurements on the same day 30 min apart and in this order. These two tests were repeated after 3 months of new disease-targeted therapy. In addition, conventional outcome measures including WHO functional class (FC), N-terminal pro-brain natriuretic peptide (NTproBNP) and Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR) score were recorded at baseline and follow-up.
Incremental cardiopulmonary exercise test
This was performed on an electromagnetically-braked cycle ergometer with 2 min of rest, followed by 3 min of unloaded cycling and then cycling at a ramp rate of 5–20 Watts/min to achieve peak work rate in 8–12 min (Ergoline Select 200, Ergoline, Bitz, Germany; Ergocard, Medisoft, Dinant, Belgium). Oxygen saturation and heart rate (HR) were monitored continuously using pulse oximetry and 12-lead ECG. Breath-by-breath oxygen uptake (Vo2), carbon dioxide output (Vco2), minute ventilation (Ve), ventilatory equivalent for oxygen, ventilatory equivalent for carbon dioxide (Ve/Vco2), oxygen pulse (Vo2/HR), end-tidal oxygen partial pressure, end-tidal carbon dioxide partial pressure (Petco2), respiratory rate and respiratory exchange ratio were measured via a face mask and averaged over 20 s. Peak Vo2 was defined as the highest averaged value within 30 s of peak exercise. Anaerobic threshold (AT) was determined by the V-slope method. Standardised reference equations were used to calculate predicted values.16 The development of right-to-left shunt through a patent foramen ovale during exercise was assessed using a set of published pulmonary gas exchange criteria.17
6-min walk test (6MWT)
The 6MWT was performed on a 20-metre corridor, but otherwise according to the American Thoracic Society guideline.18
Inert gas rebreathing (IGR) and isotime metabolic measurements during submaximal constant-load exercise
The IGR method measures pulmonary blood flow (PBF) which is equivalent to CO in the absence of significant intracardiac or intrapulmonary shunt (Innocor, Innovision, Odense, Denmark), as previously described.19–21 Patients were coached on how to perform the rebreathing manoeuvre and had 2–3 practices prior to testing. Duplicate measurements were made after 10 min of rest in the supine position and again after 10 min of rest on the upright cycle ergometer. There was an interval of 5 min between duplicate measurements to ensure complete washout of inert gases from the lungs. The patient then underwent a constant-load CPET consisting of 2 min of rest followed by 3 min of cycling at 40% maximal work rate predetermined in the incremental CPET. At the end of 3 min PBF was measured while the patient continued to cycle. Oxygen saturation and HR were measured continuously by pulse oximetry and 12-lead ECG. Breath-by-breath respired air was collected via a mouthpiece with the nose clipped and moving averages of metabolic data over eight breaths were obtained. End-exercise values were defined as the highest of the last eight averaged values and were used for isotime analysis at baseline and follow-up. Isotime analysis refers to comparison of measurements made at standardised time with an identical workload history. Stroke volume was derived from PBF and HR (PBF divided by HR). Arteriovenous oxygen content difference (Ca–vo2) was calculated from Vo2 and PBF (Vo2 divided by PBF). The exercise protocol was repeated after 15–20 min of rest. Duplicate measurements in each step were averaged to give the final results. The work rate remained the same for submaximal constant-load exercise at follow-up. A subgroup of seven patients and two separately recruited patients with stable PH underwent submaximal constant-load exercise on two separate occasions 1 day to 1 month apart to determine the intersession reproducibility of IGR measurements.
Statistical analysis
Statistical analysis was performed using Statview Version 5.0.1 (SAS Institute) and Graphpad Prism Version 5.00 (Graphpad Software, California, USA). Assuming a treatment-induced change in 6MWD of 40 m and a SD of 54 m based on data from a group of patients with idiopathic PAH receiving disease-targeted therapy,22 the sample size required to detect a treatment effect with 80% power and 5% two-tailed level of significance by paired t test would be 17. The post-hoc power calculation was repeated using data observed in this study. Continuous variables were tested for normality using D'Agostino and Pearson omnibus normality test. Normally distributed variables are shown as mean±SD and non-normally distributed variables are shown as median (IQR). Categorical variables are presented as number (%). Comparison between baseline and follow-up 6MWD, NTproBNP, CAMPHOR, IGR and isotime metabolic measurements were made by paired t test or Wilcoxon signed rank test depending on data distribution. Comparison between baseline and follow-up WHO FC was made by χ2 test. Correlation between two variables which were both normally distributed was determined by Pearson correlation coefficient (r), and otherwise by Spearman correlation coefficient (ρ). Post-hoc analysis was carried out by stratifying patients into high and low 6MWD groups using the median baseline 6MWD. Comparison of baseline characteristics between 6MWD subgroups was made by unpaired t test or Mann–Whitney U test depending on data distribution. Reproducibility of IGR measurements was determined by Bland–Altman analysis.23 Coefficient of variation (CoV) was defined as the SD of each pair of duplicate measurements expressed as a percentage of the mean of the respective pair. The overall CoV was defined as the median CoV of the whole group. A p value of <0.05 was considered significant.
Results
Patient characteristics
Twenty-four patients were recruited and their characteristics are shown in table 1. Incremental CPET abnormalities were consistent with moderately severe exercise impairment due to pulmonary vascular disease (table 2). Other factors such as the use of digoxin, diuretics and beta-blockers were unchanged during the study period. None of the study patients were involved in exercise programmes or had evidence of exercise-induced right-to-left shunt. The mean time interval between baseline testing and follow-up assessment was 3.3 months (range 2.4–4.5).
Patient characteristics
Incremental cardiopulmonary exercise test characteristics
Conventional outcome measures
After 3 months of new therapy, 6MWD increased from 384±115 m to 401±111 m (mean change 17±42 m; median change 29 (3–47) m, p=0.061). There were no significant changes in WHO FC (baseline: 50% in FC II and 50% in FC III; follow-up: 8% in FC I, 54% in FC II and 38% in FC III, p=0.215), NTproBNP (baseline: 1145±1319 pg/ml; follow-up: 1014±1066 pg/ml, p=0.436) or CAMPHOR score (baseline: 33±21; follow-up: 30±21, p=0.435).
IGR and isotime metabolic measurements
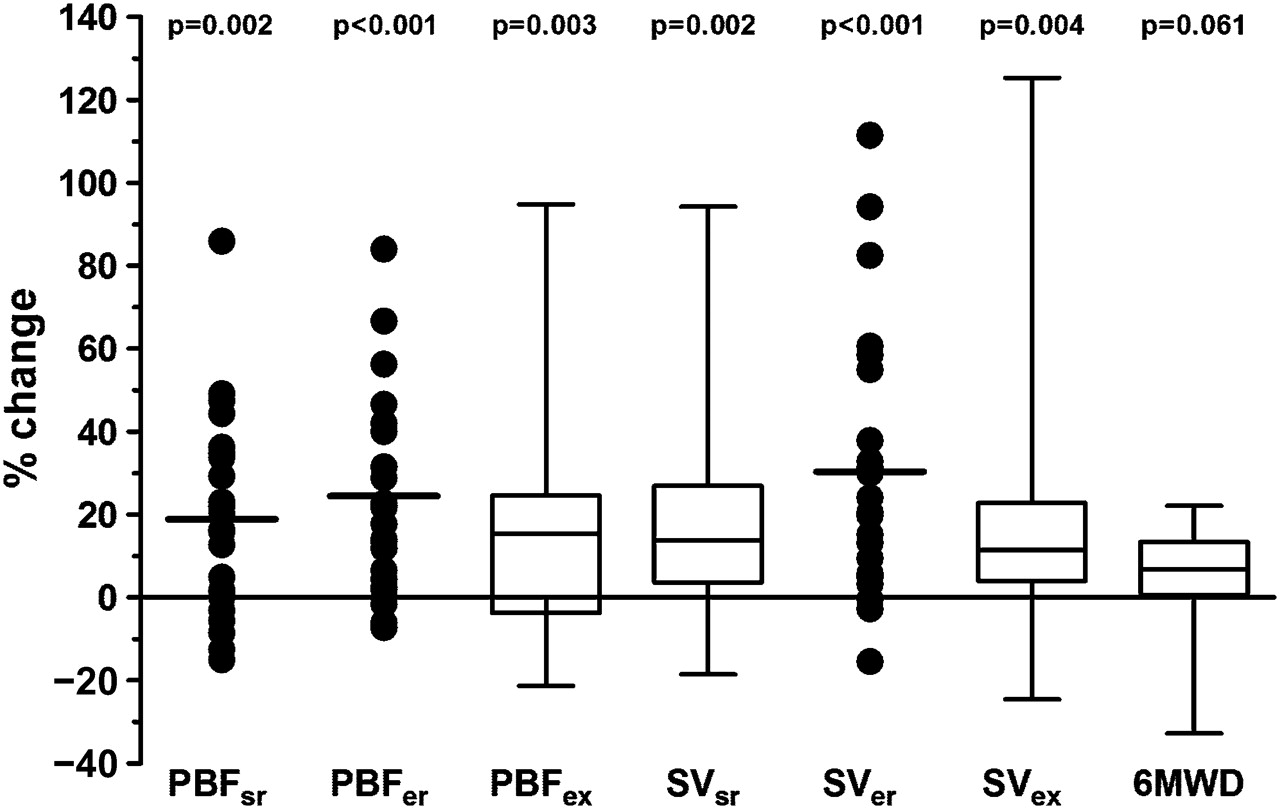
After 3 months of new therapy, IGR measurements at supine rest, erect rest and submaximal exercise increased significantly at follow-up (table 3). The change in PBF with therapy was 0.7±0.9 l/min at supine rest, 0.7±0.8 l/min at erect rest and 0.8±1.0 l/min at submaximal exercise. The change in SV with therapy was 7±10 ml at supine rest, 10±11 ml at erect rest and 6 (3–11) ml at submaximal exercise. Isotime Vo2 increased by 0.025±0.042 l/min (p=0.010) and Vo2/kg by 0.3±0.6 ml/min/kg (p=0.012). Arteriovenous oxygen content difference decreased by 1.6±3.0 ml/dl (p=0.021) and respiratory exchange ratio by 0.02±0.05 (p=0.025). There were no significant changes in Vo2/HR, Ve/Vco2 or Petco2 (see table 1 in online supplement). There were modest correlations between therapy-induced changes in IGR and isotime metabolic measurements during constant-load exercise (see figure 1A,B in online supplement). The mean/median percentage change in IGR measurements from baseline was greater than that for 6MWD (figure 1).
Inert gas rebreathing measurements during submaximal constant-load exercise
{kind=link}
Percentage changes in inert gas rebreathing measurements and six-minute walk distance from baseline. Non-normally distributed variables are represented by box and whisker plots. The whiskers represent the minimum and maximum values and the box represents the 25th and 75th percentiles. The line in the box represents the median. Normally distributed variables are represented by dot plots. The line represents the mean. PBF, pulmonary blood flow; SV, stroke volume; sr, supine rest; er, erect rest; ex, exercise; 6MWD, 6-min walk distance. p Values refer to comparison of variables between baseline and follow-up by paired t test or Wilcoxon signed rank test.
In the post-hoc analysis the high 6MWD group (477±80 m) was significantly younger and had less severe exercise impairment on incremental CPET than the low 6MWD group (291±47 m) (see table 2 in online supplement). 6MWD improved by 34±25 m (p<0.001) and isotime Vo2 by 0.033±0.031 l/min (p=0.009) with new therapy in the low 6MWD group whereas neither variable changed significantly in the high 6MWD group. In comparison, there remained a significant improvement in IGR measurements in both groups (table 4). Stratified isotime metabolic data are shown in table 3 in the online supplement.
Inert gas rebreathing measurements during submaximal constant-load exercise in 6MWD subgroups
Correlation between 6MWD and IGR measurements
At baseline, 6MWD correlated with submaximal exercise PBF (r=0.52, p=0.008) and SV (r=0.47, p=0.021). At follow-up, 6MWD correlated with supine rest PBF (r=0.46, p=0.025) and SV (ρ=0.42, p=0.041), submaximal exercise PBF (ρ=0.53, p=0.010) and SV (r=0.54, p=0.008). There was no significant correlation between 6MWD and erect rest IGR measurements or between therapy-induced changes in 6MWD and IGR measurements.
Post-hoc power calculation
This was performed using data on treatment effect and SD observed in this study for conventional outcome measures, IGR and isotime metabolic measurements (see table 4 in online supplement). Much larger sample sizes would be required for conventional outcome measures (50–268) and isotime metabolic variables (24–100) to detect a treatment effect compared with IGR measurements (13–22).
Intersession reproducibility of IGR measurements
Based on 27 duplicate measurements, the mean difference of duplicate PBF measurements was 0.12 l/min with 95% limits of agreement −0.53 to 0.75 l/min. The mean difference of duplicate SV measurements was 1.4 ml with 95% limits of agreement −7.2 to 9.9 ml. The median CoV was 2.9% for PBF and 4.2% for SV.
Discussion
This study is the first to show that PBF and SV measured non-invasively at rest and during submaximal constant-load exercise by the IGR method could be used to detect the effect of proven disease-targeted therapy in a group of patients with precapillary PH. The sample size required for IGR measurements to detect a treatment effect was considerably smaller than that required for conventional outcome variables, suggesting that IGR measurements may be more sensitive outcome measures. In the post-hoc analysis, IGR measurements were able to demonstrate a treatment effect in both high and low 6MWD groups whereas 6MWD did not change with therapy in the high 6MWD group. This finding would suggest that IGR measurements may be more sensitive than 6MWD in detecting therapy-induced changes in fitter patients. In addition, IGR measurements were shown to have good intersession reproducibility.
Improvement in IGR measurements with therapy was observed across supine rest, erect rest and submaximal exercise. In addition, the exercise response in PBF or SV was unchanged with therapy. Therefore, resting IGR measurements appear to be as sensitive as submaximal exercise measurements in detecting a treatment effect in this study population. The prognostic significance of SV has been demonstrated in a previous study using cardiac MRI.22 In a group of patients with idiopathic PAH, a low SV at baseline predicted survival independently. More importantly, change in SV with disease-targeted therapy was more predictive of survival than change in 6MWD in multivariate analysis, confirming a correlation between SV and clinical outcome. The inability of 6MWD to demonstrate a treatment effect in patients with higher 6MWD in this study concurs with the finding from a previous study which showed that haemodynamic indices measured at RHC were more sensitive than 6MWD as outcome measures in patients with PAH walking >450 m.24 The precise mechanism behind this observation is unclear, but is thought to be related to the ceiling effect of 6MWD.
Metabolic variables during incremental CPET have been shown to have prognostic significance, but previous studies using these variables as outcome measures in PAH showed mixed results.25 The use of metabolic variables to assess treatment response in PH is revisited in this study using isotime comparison at submaximal constant-load exercise. At follow-up there was a small significant increase in Vo2 and a decrease in Ca–vo2 consistent with an improved exercise CO secondary to treatment, but no change in the metabolic indices of ventilatory efficiency. There is therefore no conclusive evidence from this study to support the use of isotime metabolic variables to assess treatment response, but it does add to the current body of literature on the use of CPET in PAH, an area where more research is required.
Although the findings of this study are preliminary, the use of IGR measurements in PH warrants further studies, especially in specific patient groups. IGR measurements would allow more reliable assessment of therapy-induced changes in patients with comorbid conditions affecting 6MWD, such as patients with connective tissue disease. They may also be superior to 6MWD as outcome measures in clinical trials focused on patients with less advanced disease. Resting measurements could be used to assess patients who are too disabled to perform a 6MWT. In addition, simultaneous measurement of SV and Vo2 would allow determination of Ca–vo2, thereby identifying patients with peripheral muscle dysfunction confounding exercise limitation, which is a recognised phenomenon in PAH.26 In this setting, exercise training may have an adjunctive role to medical therapy in improving exercise capacity.27
This study has a number of limitations. It was underpowered to detect changes in WHO FC, NTproBNP and CAMPHOR score with new therapy. The aetiology of PH in the study population was heterogeneous, including patients with CTEPH and one patient with sarcoidosis, but this reflects the real-life nature of the study population. Although disease-targeted therapy is currently not approved in CTEPH, there is some evidence from several uncontrolled studies and one randomised controlled trial to support its efficacy. Its off-label use in patients with inoperable disease, persistent PH after surgery or as a bridge to surgical intervention is recommended by current guidelines.15 28 29 In sarcoidosis, the mechanisms limiting exercise may differ from PAH or CTEPH, but excluding this patient did not affect the results of the analyses. Patients in WHO FC IV were not included as they were unable to perform exercise tests. Prevalent patients were included whose response to new therapy might be less marked than that seen in treatment-naive patients, but the number was small and this would not have affected the comparison between 6MWD and IGR measurements. Repeat RHC data were not available at follow-up to assess treatment efficacy, but this was not the aim of the study. The present study was designed to determine if the effect of proven disease-targeted therapy could be detected by IGR measurements alongside conventional outcome measures in patients with precapillary PH representative of those seen in routine clinical practice.
Conclusions
This study is the first to show that non-invasive resting and submaximal exercise haemodynamic measurements by the IGR method could be used to detect treatment response in precapillary PH. The data analysis also suggests that these measurements may be more sensitive than 6MWD in detecting the effects of therapy in fitter patients. In comparison, other conventional outcome measures and isotime metabolic variables were less responsive to change.
Acknowledgments
The authors thank all patients for their participation in this study and the Pulmonary Hypertension Association UK for their financial support.
References
Supplementary materials
Web Only Data thx.2011.159228
Files in this Data Supplement:
Footnotes
Funding Pulmonary Hypertension Association UK and Enzysive/Pfizer UK Inc.
Competing interests None.
Ethics approval This study was conducted with the approval of the West Glasgow research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.