Article Text

Statistics from Altmetric.com
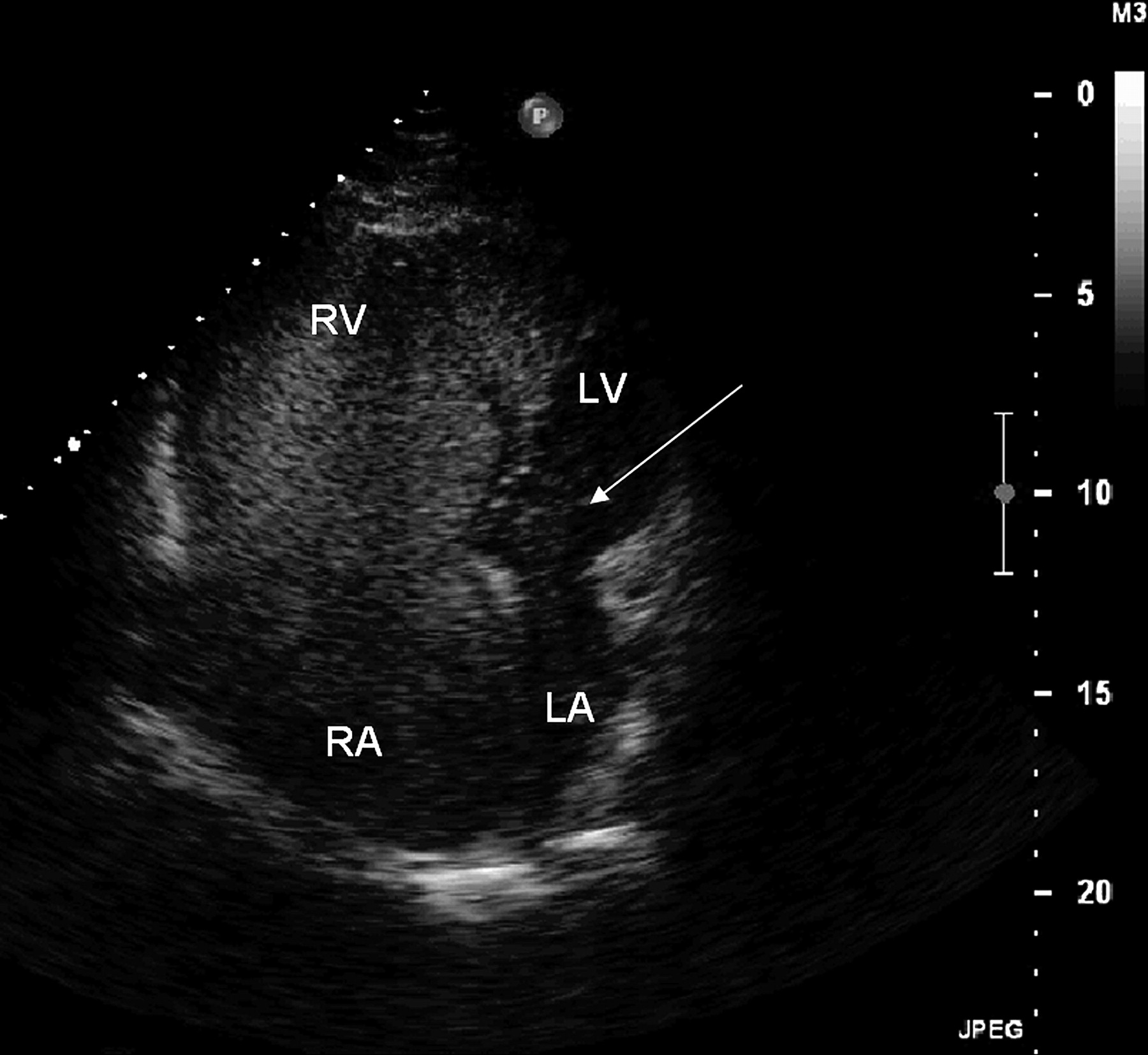
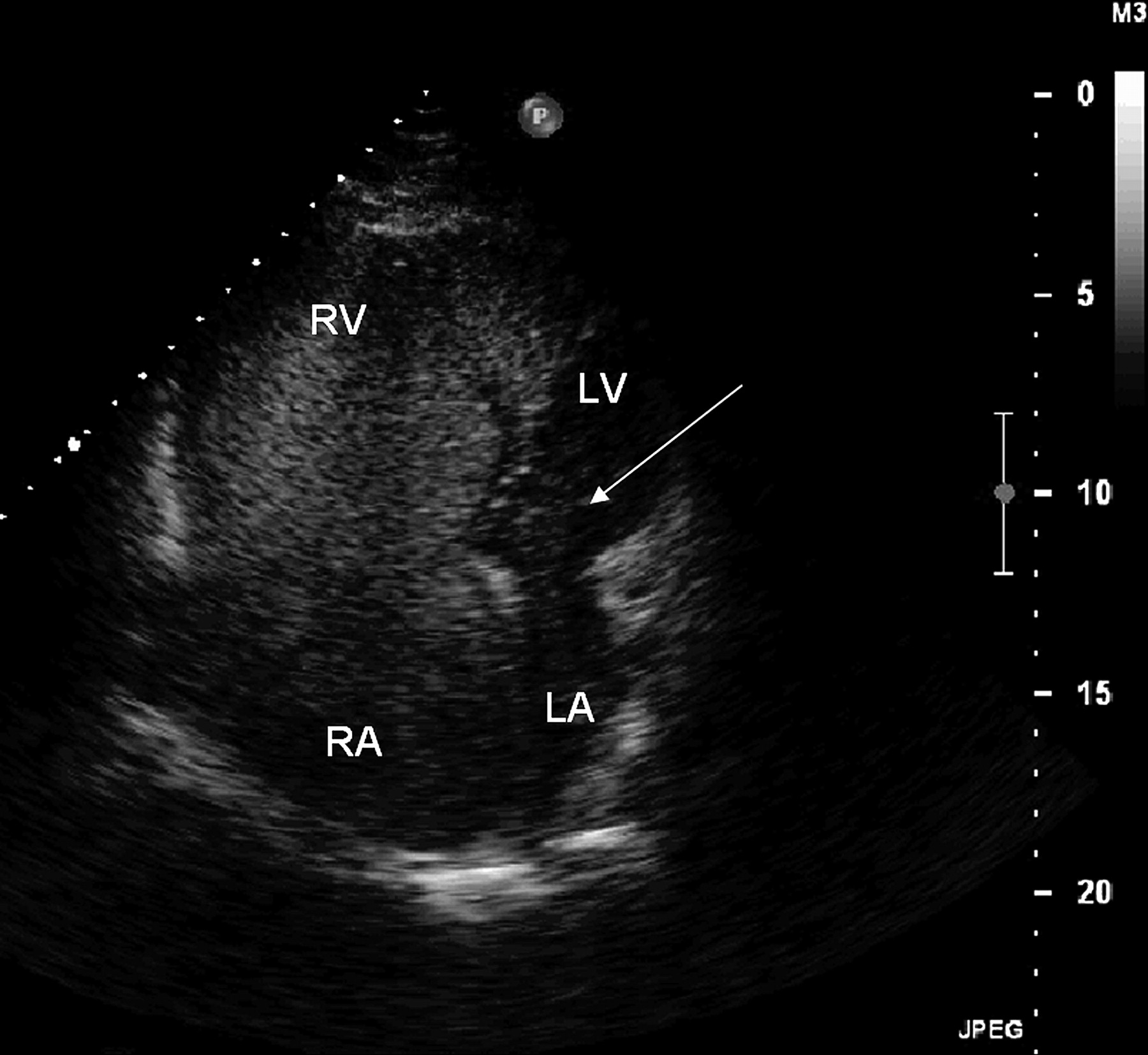
We reported a case of a 30-year-old Hispanic patient with a history of idiopathic pulmonary arterial hypertension (PAH). A baseline catheterisation showed a mean pulmonary artery pressure (PAP) of 58 mm Hg, capillary wedge pressure of 14 mm Hg, cardiac index of 2.7 l/min/m2 and pulmonary vascular resistance of 7.5 WU, with no response to adenosine. A pulmonary CT scan ruled out thromboembolism or significant abnormalities (such as glass opacities, septal lines or mediastinal node enlargement commonly seen in venocclusive disease1); albumin macroaggregate lung perfusion scan showed normal perfusion without significant intrapulmonary shunt (IPS). He was started on diuretics, oxygen and sildenafil 25 mg three times a day. Despite treatment, dyspnoea worsened and 2 months later the patient was referred to our centre. At admission, the patient was in WHO functional class (FC) IV; his resting PaO2 had dropped to 56 mm Hg. No decompensating factor was identifiable. A saline-contrast transthoracic echocardiography (SC-TTE) showed a dilated right ventricle (70 mm) with mild ventricular dysfunction and an estimated systolic PAP of 100 mm Hg. Peripheral injection of 10 ml agitated saline evidenced delayed appearance of bubbles in the left atrium, suggestive of IPS (figure 1). After discontinuing sildenafil for 48 h, his PaO2 improved to 64 mm Hg and the SC-TTE showed no evidence for IPS. Thirty minutes after a challenge dose of 50 mg sildenafil orally, the SC-TTE evidenced IPS recurrence with a PaO2 drop to 55 mm Hg despite oxygen administration. After permanent discontinuation of sildenafil, the patient had a significant clinical improvement and was discharged with nebulised iloprost 5 μg four times a day. At 6 months follow-up, he remains in FC II without further hospitalisations.
{kind=link}
Saline-contrast transthoracic echocardiogram showing right-to-left shunt. LA, left auricle; LV, left ventricle; RA, right auricle; RV, right ventricle.
Hypoxaemia in PAH patients might be due to ventilation–perfusion mismatch, depression of cardiac output or right-to-left shunting. SC-TTE offers a fast, non-invasive approach to diagnose right-to-left shunting. Under normal circumstances, saline microbubbles only appear in the right heart chambers. Presence of microbubbles in the left chambers suggests an arteriovenous connection, either due to an atrial septal defect, ventricular septal defect with Eisenmenger's syndrome or IPS. The time frame for contrast appearance in the left chambers allow to differentiate between intracardiac shunting (one or two cardiac cycles after its appearance in right chambers) and IPS (four to eight cycles).2 Sildenafil administration in PAH patients is associated with a significant reduction of pulmonary-to-systemic vascular resistance ratio, with improvement in arterial oxygenation and 6 min walk distance.3 However, any vasodilator may theoretically exacerbate hypoxaemia by increasing perfusion to poorly ventilated areas in patients with lung disease, resulting in further ventilation–perfusion mismatch. Kleinsasser et al4 demonstrated, in a porcine model, that a high dose of sildenafil results in a dose-dependent fall in vascular pulmonary resistance associated with a marked increase in ventilation–perfusion heterogeneity, as seen in patients treated with a high dose of intravenous epoprostenol in whom IPS and severe hypoxaemia occurred.5 In these cases, an accurate diagnosis and drug down-titration or discontinuation allowed a rapid recovery of the symptoms. In conclusion, sildenafil may be associated with development of IPS and hypoxaemia in PAH patients. In these cases, an SC-TTE should be performed in order to disclose previously undiagnosed IPS.
Footnotes
Institution at which the work was performed: Pontificia Universidad Católica de Chile, Santiago de Chile, Chile.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Pontificia Universidad Católica de Chile.
Provenance and peer review Not commissioned; externally peer reviewed.