Article Text

Statistics from Altmetric.com
Introduction
A 19-year-old male patient with a history of asthma was in good health until he developed a sudden-onset, right side pleuritic chest discomfort and shortness of breath. At that time, he was on a cruise to Puerto Rico. He returned home 1 week later and was evaluated in the emergency room at that time. On further history, he denied cough, fever, chills, night sweats, weight loss, sputum production, haemoptysis or other symptoms. He did not recall recent sick contacts or exposure to tuberculosis. He was born in the USA and this cruise was his only recent travel. He worked in a law firm and denied significant occupational exposures, any tobacco or drug use, allergies or significant family history of lung or cardiovascular disease. Tachycardia was the only abnormality on his physical examination, and initial laboratory testing were completely normal. His pulse oximetry measurement was 97% O2 saturation on room air at rest. His ECG was consistent with sinus tachycardia, with a rate of 108/min and no ST–T wave changes. He was admitted to the hospital for further investigation of his chest pain.
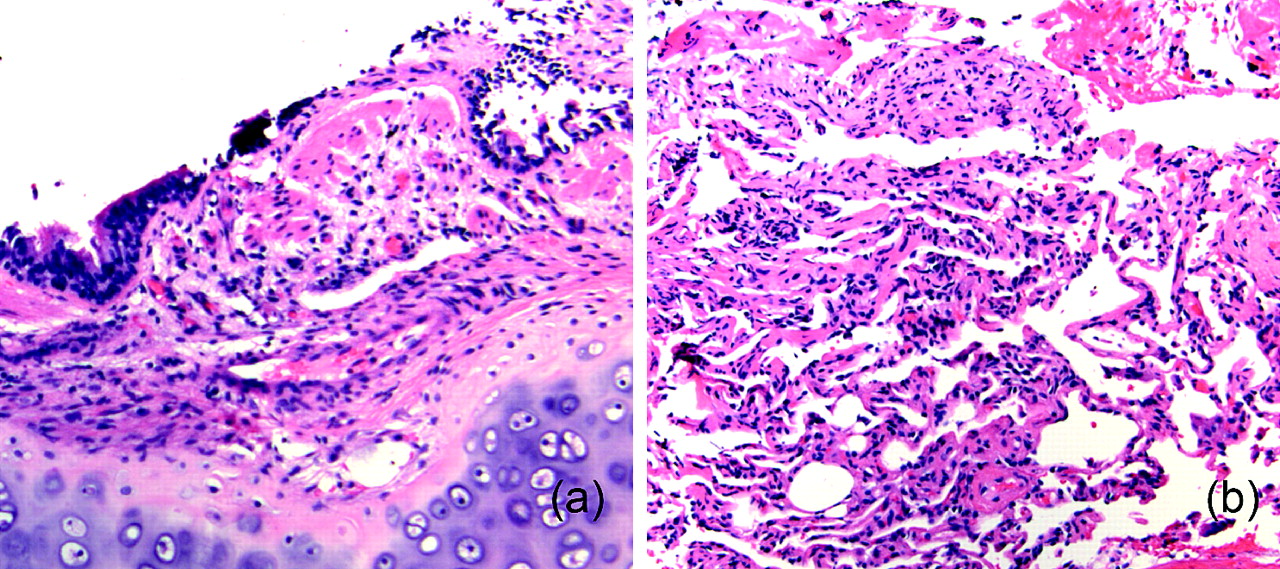
His chest radiograph (figure 1A) and chest CT scan (angiogram protocol) (figure 1B) were abnormal but showed no evidence of pneumothorax or pulmonary embolism. A small unilateral pleural effusion was present but was too small to sample using bedside ultrasonography. All subsequent blood tests in the hospital including cardiac enzymes, immunoglobulins levels and vasculitis screen were all unremarkable. The chest x-ray and CT scan were remarkable for the predominance of right-sided findings with relative sparing of the left side. This suggested the possibility of unilateral interstitial lung disease.Therefore, the patient underwent bronchoscopy to further narrow the differential diagnosis. Airway examination revealed prominent submucosal blood vessels with mucosal oedema and hyperaemia involving the surface of the right side airways with complete sparing of the left side airways. The biopsies revealed interstitial oedema and early fibrotic changes (figure 2A,B). On further review of the CT scan, an extraneous septum within the left atrium was noted and the diagnosis was made (figure 3).

(A) Chest radiograph showing significant mediastinal shift and volume loss on the right side, with prominent vascular markings only seen on the right side, (B) Chest CT scan showing right-sided volume loss with hypolucency, prominent right interstitial markings, subsegmental atelectasis, very small right pleural effusion and small right hilar and mediastinal adenopathy.

(A) Mucosal endobronchial biopsy: bronchial tissue with prominent submucosal capillaries and mild fibrosis. (B) Transbronchial biopsy: lung parenchyma with mild interstitial chronic inflammation and alveolar macrophages.

Chest CT scan that shows the septum in the left atrium.
Question
What is the diagnosis?
See page 313 for the answer
Answer
From the question on page 285
This is an unusual case of cor triatriatum sinistrum with secondary unilateral pulmonary venous hypertension and right lung hypoplasia. The interstitial changes in the parenchyma were secondary to a state of chronic congestion as a result of reduced interstitial fluid drainage due to elevated pressures in the right pulmonary vein. Our biopsy specimens highlight how chronic persistent interstitial oedema can result in chronic inflammation and the development of interstitial fibrosis.1 2 The enlarged mediastinal lymph nodes were probably hyperplastic and the gross findings on bronchoscopy reflected compensatory hypertrophy of the bronchial circulation draining into the right pulmonary vein.
Transoesophageal echocardiogram revealed a membrane in the left atrium (LA), preferentially obstructing the right pulmonary venous inflow. The obstruction was incomplete, and high velocity flow across the membrane suggested elevated right pulmonary venous pressure of 25–30 mm Hg (figure 4A,B). This was confirmed by cardiac MRI which showed asymmetric pulmonary blood flow, with ∼15–20 times more flow to the left lung than the right, with delay enhancement within the LA (figure 5). In our patient, despite the paucity of literature, surgical options were carefully considered. The patient underwent median sternotomy with surgical excision of the fibromuscular intra-atrial septum due to concerns about further progression of the pulmonary venous hypertension and the subsequent effects on the interstitium of his right lung. His postoperative course was unremarkable, and a 3-month follow-up cardiac MRI showed that the LA membrane can no longer be seen and there is no longer evidence of delayed enhancement within the LA (figure 6). Also, of note, there was a marked improvement in the flow differential between the right and left pulmonary veins on MRI.

(A) Echocardiogram: apical four-chamber view showing the septum (arrow) and extra atrial chamber (asterisk) (B) Echocardiogram: colour Doppler enhanced showing different flow velocities within the left atrium (arrow).

Preoperative cardiac MRI showing the left atrium (LA) membrane and the flow differential between the right and left pulmonary veins. Serial axial MRIs obtained during infusion of contrast demonstrate prompt enhancement and washout of the left inferior pulmonary vein (arrow), distal left atrium (dLA) and left ventricle (LV). The right inferior pulmonary vein (arrowhead) and proximal left atrium (pLA) show delayed enhancement. The LA membrane can be seen in image (b).

Serial axial MRIs obtained during infusion of contrast demonstrate gradual uniform enhancement of the left atrium (LA) and left ventricle (LV). The interatrial membrane has been resected. Note: the right pulmonary veins, while present were not seen in this slice location.
Discussion
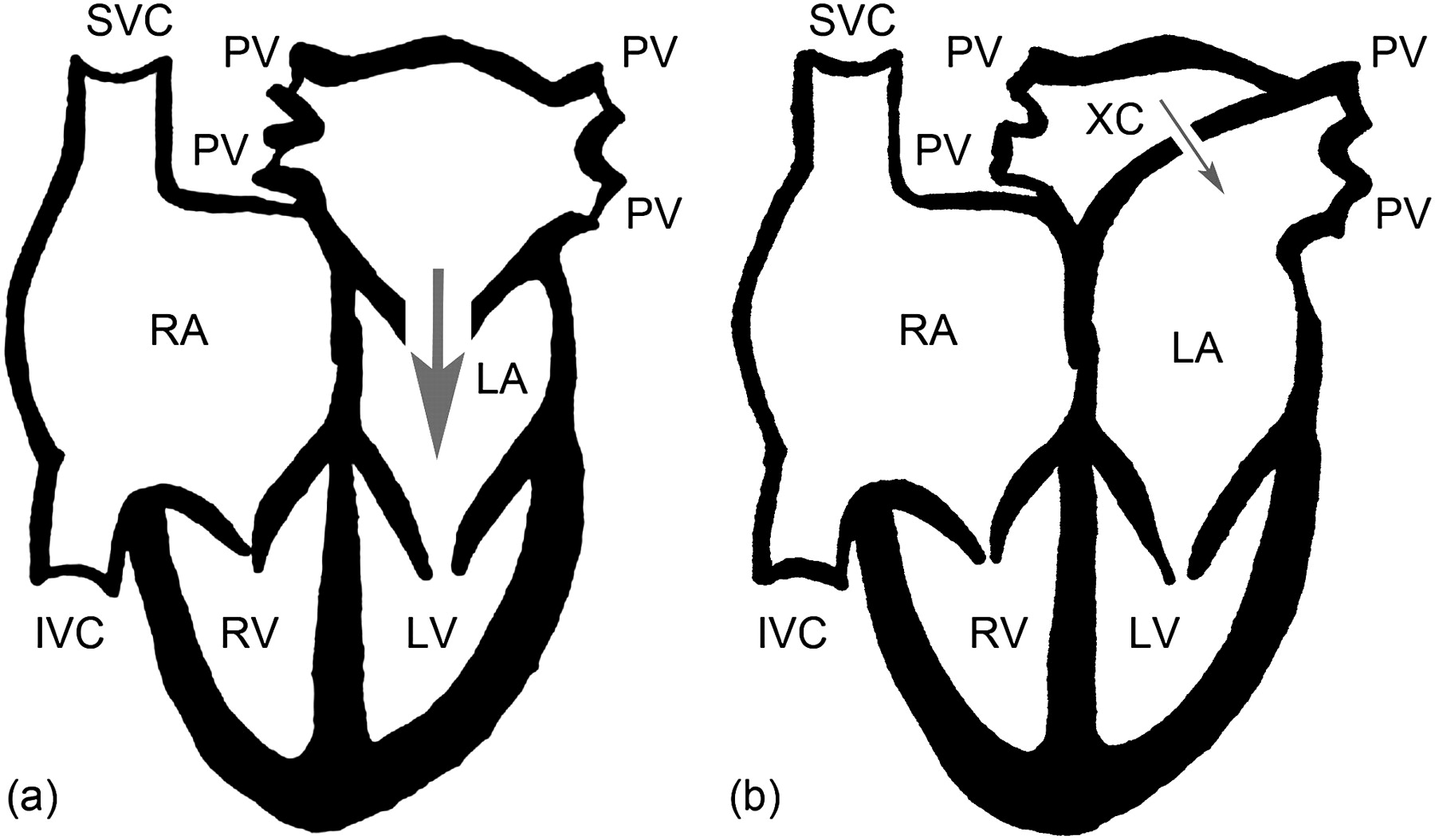
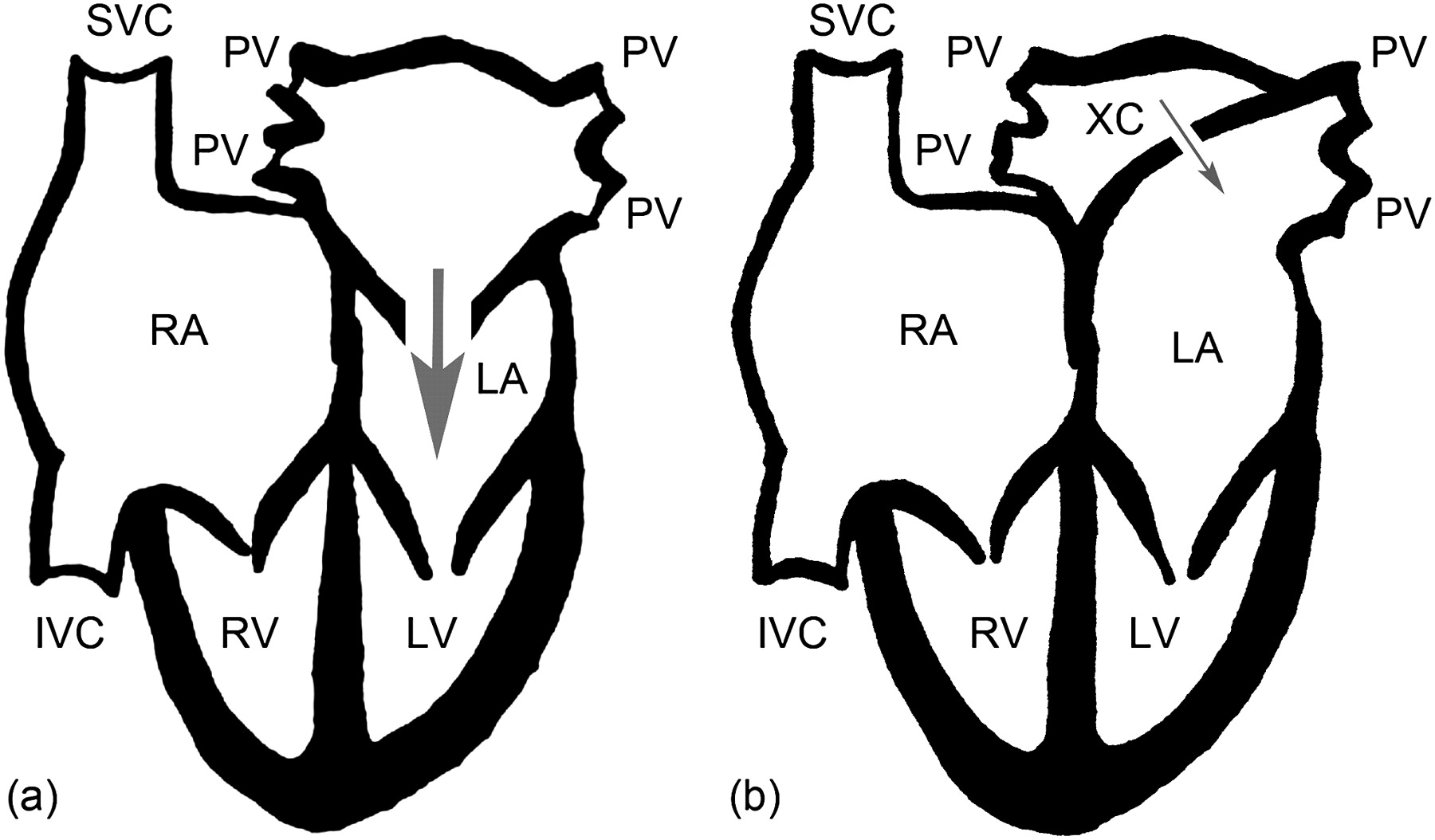
To our knowledge, this is the first report in the literature of a patient with unilateral pulmonary venous hypertension and unilateral hypoplastic lung related to an atypical cor triatriatum sinistrum. Therefore, it is very important to distinguish this unusual case from other reported cases of classic cor triatriatum sinistrum. Typically, all of the pulmonary venous drainage enters the proximal chamber and then crosses the septum through small fenestration(s) into the distal chamber (figure 7A). As a consequence, pulmonary venous hypertension (bilateral) develops and results in recurrent pulmonary oedema. This clinical syndrome resembles (and is frequently misdiagnosed as) congenital mitral stenosis.3 Surgical resection in these circumstances is the optimal therapeutic option.4
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Classic cor triatriatum sinistrum: illustration of the pulmonary veins entering the proximal chamber with the incoming blood escaping through a small fenestration(s) that communicates with the distal left atrium. (B) Unusual cor triatriatum sinistrum (our patient): the extra chamber created by the intra-atrial septum separated the right from the left pulmonary veins by a membrane with a pin-hole fenestration, creating significant pulmonary venous congestion and hypertension in the right lung.
In our patient, the intra-atrial septum separated the right from the left pulmonary veins, creating a small chamber in the left atrium that had the right pulmonary venous return (figure 7B). A pin-hole fenestration connected this chamber with the supramitral left atrium that received left pulmonary venous return. This created significant isolated pulmonary venous congestion and pulmonary venous hypertension in the right lung with significant difference in pulmonary blood flow between the right and left lungs as demonstrated at cardiac MRI.
This case highlights the need to consider a cardiac aetiology in patients with prominent unilateral interstitial lung markings on chest x-ray or CT scan, and how echocardiography and cardiac MRI are valuable tools in the diagnosis and follow-up of such conditions. Surgical resection of the membrane appears to be the optimal treatment option for all age groups.
Footnotes
Institution at which work was performed Rhode Island Hospital, Providence, RI 02903.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves