Article Text

Abstract
Background: Although the use of antiretroviral therapy has led to dramatic declines in AIDS-associated mortality, Pneumocystis pneumonia (PCP) remains a leading cause of death in HIV-infected patients.
Objectives: To measure mortality, identify predictors of mortality at time of illness presentation and derive a PCP mortality prediction rule that stratifies patients by risk for mortality.
Methods: An observational cohort study with case note review of all HIV-infected persons with a laboratory diagnosis of PCP at San Francisco General Hospital from 1997 to 2006.
Results: 451 patients were diagnosed with PCP on 524 occasions. In-hospital mortality was 10.3%. Multivariate analysis identified five significant predictors of mortality: age (adjusted odds ratio (AOR) per 10-year increase, 1.69; 95% CI 1.08 to 2.65; p = 0.02); recent injection drug use (AOR 2.86; 95% CI 1.28 to 6.42; p = 0.01); total bilirubin >0.6 mg/dl (AOR 2.59; 95% CI 1.19 to 5.62; p = 0.02); serum albumin <3 g/dl (AOR 3.63; 95% CI 1.72–7.66; p = 0.001); and alveolar–arterial oxygen gradient ⩾50 mm Hg (AOR 3.02; 95% CI 1.41 to 6.47; p = 0.004). Using these five predictors, a six-point PCP mortality prediction rule was derived that stratifies patients according to increasing risk of mortality: score 0–1, 4%; score 2–3, 12%; score 4–5, 48%.
Conclusions: The PCP mortality prediction rule stratifies patients by mortality risk at the time of illness presentation and should be validated as a clinical tool.
Statistics from Altmetric.com
In 1996, the approval of HIV protease inhibitors and their use in combination with two nucleoside reverse transcriptase inhibitors heralded the current era of combination antiretroviral therapy (CART) that has witnessed dramatic declines in AIDS-associated mortality.1 Pneumocystis pneumonia (PCP), however, remains the most common AIDS-defining illness in the current era, and is a frequent cause of morbidity and mortality in HIV-infected patients.2 3 In the pre-CART era, mortality from PCP ranged from 10% to 30%,4 5 6 7 8 9 with even higher mortality rates of 35–85% in patients requiring admission to an intensive care unit (ICU).10 11 12 13 14 15 16 In comparison, few studies have examined PCP mortality in the CART era. One study based in North America reported a PCP mortality of 11.6% in the CART era,17 while a study based in the UK reported a decrease in PCP mortality during the pre-CART to CART eras from 14.8% to 9.7% (p = 0.142).18 None of the patients, however, was receiving CART.18 Whether mortality from PCP has changed since the introduction of CART is an important, unanswered question.
Previous studies have reported predictors of mortality in HIV-infected patients with PCP. In multivariate analysis, age,18 19 alveolar–arterial oxygen gradient (A–a O2 gradient),9 20 serum albumin,12 17 20 total lymphocyte count,9 haemoglobin,18 serum lactate dehydrogenase (LDH)5 and body mass index9 have been reported to be predictors of mortality. Results have been inconsistent, as not all studies were powered to identify each variable (eg, age, PaO2 or LDH) as predictors of mortality.19 21 In addition, most of these studies were performed before the introduction of CART and included patients who were presumptively diagnosed with PCP without laboratory confirmation.9 22 Finally, some predictors of mortality, such as HIV wasting, are subject to variability in provider interpretation, while others, such as bronchoalveolar lavage (BAL) neutrophilia or pulmonary Kaposi sarcoma, require specialty consultation and bronchoscopy and are therefore only performed in a subset of persons later in the hospital course.8 18 21 Because of these limitations, clinicians lack a simple tool for stratifying patients with PCP by risk for mortality at illness presentation.
Therefore, we performed a retrospective observational cohort study with case note review of all HIV-infected patients with laboratory-diagnosed PCP at San Francisco General Hospital (SFGH) in the decade immediately after the introduction of CART. Our three goals were to measure in-hospital mortality in the CART era; to identify objective, independent predictors of mortality that are available at the time of illness presentation; and to derive a PCP mortality prediction rule that stratifies patients by risk for in-hospital mortality.
Materials and methods
Patients
Patients were consecutive HIV-infected persons diagnosed with PCP at SFGH between 1 January 1997 and 31 December 2006. PCP was diagnosed by identification of Pneumocystis cystic or trophic forms on microscopic examination of Giemsa-stained (Diff-Quik stain, Dade Behring, Newark, Delaware, USA) induced sputum or BAL specimens. We identified PCP cases by reviewing a registry of all diagnostic tests performed for PCP in the Division of Pulmonary and Critical Care Medicine. Because the Pulmonary Division performs all diagnostic procedures (sputum induction and bronchoscopy) for PCP and the standard of care is to confirm the diagnosis of PCP, it is unlikely that any cases were treated empirically or diagnosed without our involvement or knowledge.23 We confirmed all cases using the SFGH electronic medical record. The University of California, San Francisco Committee on Human Research approved the study protocol.
Data collection
Data were collected by case note review using standardised abstraction forms and predetermined definitions. Predictor variables consisted of demographic characteristics, medical history, initial vital signs, and laboratory data at presentation. CART was defined as use of at least three antiretroviral agents from two or more drug classes. Mortality was defined as death in the hospital or after transfer to hospice care.
Statistical analysis
Statistical analysis was performed using SAS version 9.1 (SAS Institute, Cary, North Carolina, USA). Bivariate and multivariate analyses were performed using logistic regression with mortality as the dependent variable. We used general estimating equations to adjust for clustered values among multiple PCP episodes of the same patient; multiple episodes per patient were ordered by visit date. Predictors with non-normal distribution were dichotomised using cut-off points based on either median or clinically relevant values. We considered all predictors with p values <0.05 in bivariate analysis for inclusion in the multivariate model. However, to avoid a multicolinear effect with CD4 cell count and A–a O2 gradient, respectively, total lymphocyte count and oxygen saturation were excluded from the multivariate model. There was a strong positive linear correlation between age and blood urea nitrogen (BUN) (Pearson correlation coefficient = 0.24, p<0.001). Therefore, BUN was excluded from the model because earlier studies have reported age rather than BUN as a predictor of PCP mortality.18 19 To develop the best-fit model, we used stepwise logistic regression and specified a level of significance (alpha) >0.10 for elimination. To assess for trend in PCP mortality over time, we performed Poisson regression with a variable for calendar year, setting 1997 equal to 0 and increasing the value by 1 for each subsequent year.24 All statistical tests were two-sided; a p value <0.05 was considered statistically significant.
Results
From 1 January 1997 to 31 December 2006, 524 consecutive episodes of PCP were diagnosed in 451 HIV-infected patients at SFGH. Overall, 503 episodes (96%) required hospitalisation and 21 episodes (4%) were treated as outpatients; no subject treated for PCP as an outpatient died in the month following diagnosis. The number of PCP cases per year decreased throughout the study period, from a high of 74 cases in 1998 to a low of 28 cases in 2006. There was no significant change in mortality by study year, which ranged from 5% to 15% (p = 0.40). A total of 56 patients had more than one episode of PCP diagnosed during the study period. There was no significant difference in mortality between a first episode of PCP and a repeat episode (11% (48 of 451 first episodes) vs 8% (6 of 73 repeat episodes), respectively, p = 0.54).
Demographic and clinical characteristics at admission
The mean age of the cohort was 41 years, and the majority were men (87%) and of non-white race (53%) (table 1). While the main risk factor for HIV infection was being a man who has sex with other men (59%), injection drug use was also common (37%). HIV was newly diagnosed during evaluation for PCP in 121 patients (23%). Patients were severely immunosuppressed at presentation, with a median CD4 cell count of 29 cells/μl (interquartile range (IQR) 13–64 cells/μl). While 52% of patients had a history of opportunistic infection, only 11% were taking CART and 15% were taking PCP prophylaxis. The median CD4 cell count in patients taking CART prior to admission was not significantly different compared with patients not taking CART (36 vs 28 cells/μl, p = 0.89). However, patients taking CART had a significantly lower HIV viral load (11.5 vs 12.2 log copies/ml, p = 0.001). Of the patients taking CART, 44% had initiated treatment in the 2 months prior to admission. There were no significant differences in admission laboratory indices or hospital outcomes between patients who had recently started CART and those who had not. Laboratory data were characterised by a marked abnormality in gas exchange, with a median A–a O2 gradient of 47 mm Hg (IQR 33–61 mm Hg).
Characteristics of 524 HIV-infected patients with Pneumocystis pneumonia at San Francisco General Hospital, 1997–2006
Hospital course and outcomes
In-hospital mortality was 10.3%. The median length of stay was 8 days (range 2–80 days). The diagnosis of PCP was made by sputum induction in 67% of cases and by BAL in the remaining 33%. The sensitivity of sputum induction for diagnosis of PCP was 73%. Trimethoprim–sulfamethoxazole was the initial antimicrobial therapy for 82% of episodes (402 of 493), and 79% of the patients received adjunctive corticosteroids (390 of 493). A minority of patients were initiated on CART in the hospital (38 of 440; 9%). Only 33 patients developed a pneumothorax, but in-hospital mortality in these patients was high (73%). Overall, 16% of patients required ICU care and 13% required mechanical ventilation. The mortality in these patients was 54% and 65%, respectively.
Predictors of mortality
There were 16 variables at presentation that were significantly associated with mortality in bivariate analysis: age, recent injection drug use during the 6 months before admission, temperature, systolic blood pressure, room air O2 saturation, CD4 cell count, total lymphocyte count, sodium, BUN, total bilirubin, serum albumin, A–a O2 gradient, serum LDH, medical co-morbidity, hepatic insufficiency and pneumothorax at admission (table 2). Among events occurring during hospitalisation, requiring intensive care (p<0.001) and mechanical ventilation (p<0.001) were associated with increased mortality, as was development of a pneumothorax (p<0.001). Factors that were not associated with mortality included gender, race, tobacco use, haematocrit, new diagnosis of HIV, first versus repeat episode of PCP, and use of PCP prophylaxis or CART before admission.
Characteristics associated with mortality in bivariate analysis in 524 HIV-infected patients with PCP
In multivariate analysis using stepwise regression, the best fitting model retained six predictors that were associated with mortality (table 3). Significant predictors included two sociodemographic variables and three laboratory variables: age (adjusted odds ratio (AOR) per 10-year increase, 1.69; 95% CI 1.08 to 2.65; p = 0.02); recent injection drug use (AOR 2.86; 95% CI 1.28 to 6.42; p = 0.01); total bilirubin >0.6 mg/dl (AOR 2.59; 95% CI 1.19 to 5.62; p = 0.02); serum albumin <3 g/dl (AOR 3.63; 95% CI 1.72 to 7.66; p = 0.001); and A–a O2 gradient ⩾50 mm Hg (AOR 3.02; 95% CI 1.41 to 6.47; p = 0.004). CD4 count <50 cells/μl was retained in the best-fitting model but was not a significant predictor of mortality (AOR 2.34; 95% CI 0.95 to 5.80; p = 0.07).
Characteristics associated with mortality in multivariate analysis in 524 HIV-infected patients with PCP
A prediction rule for PCP mortality
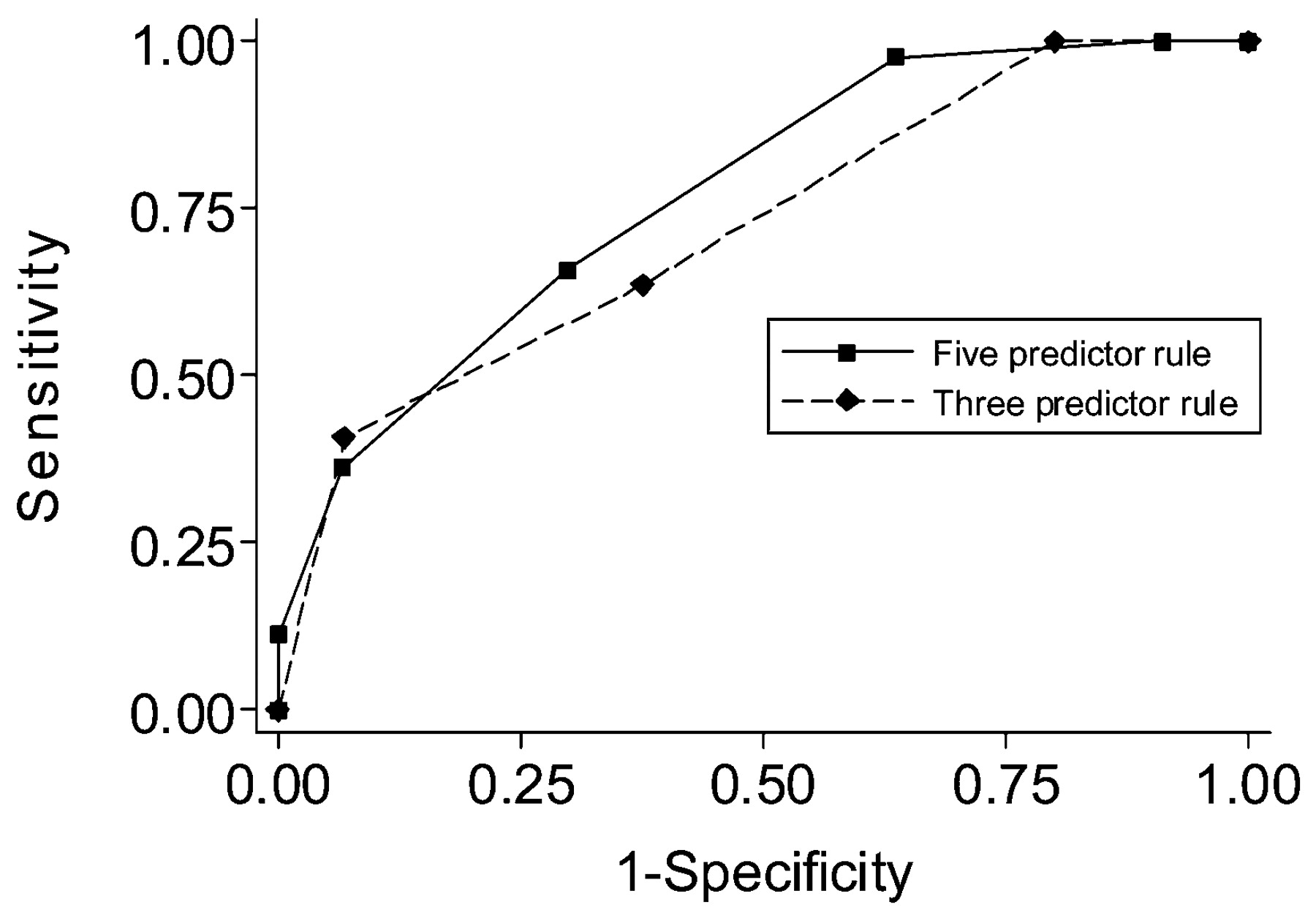
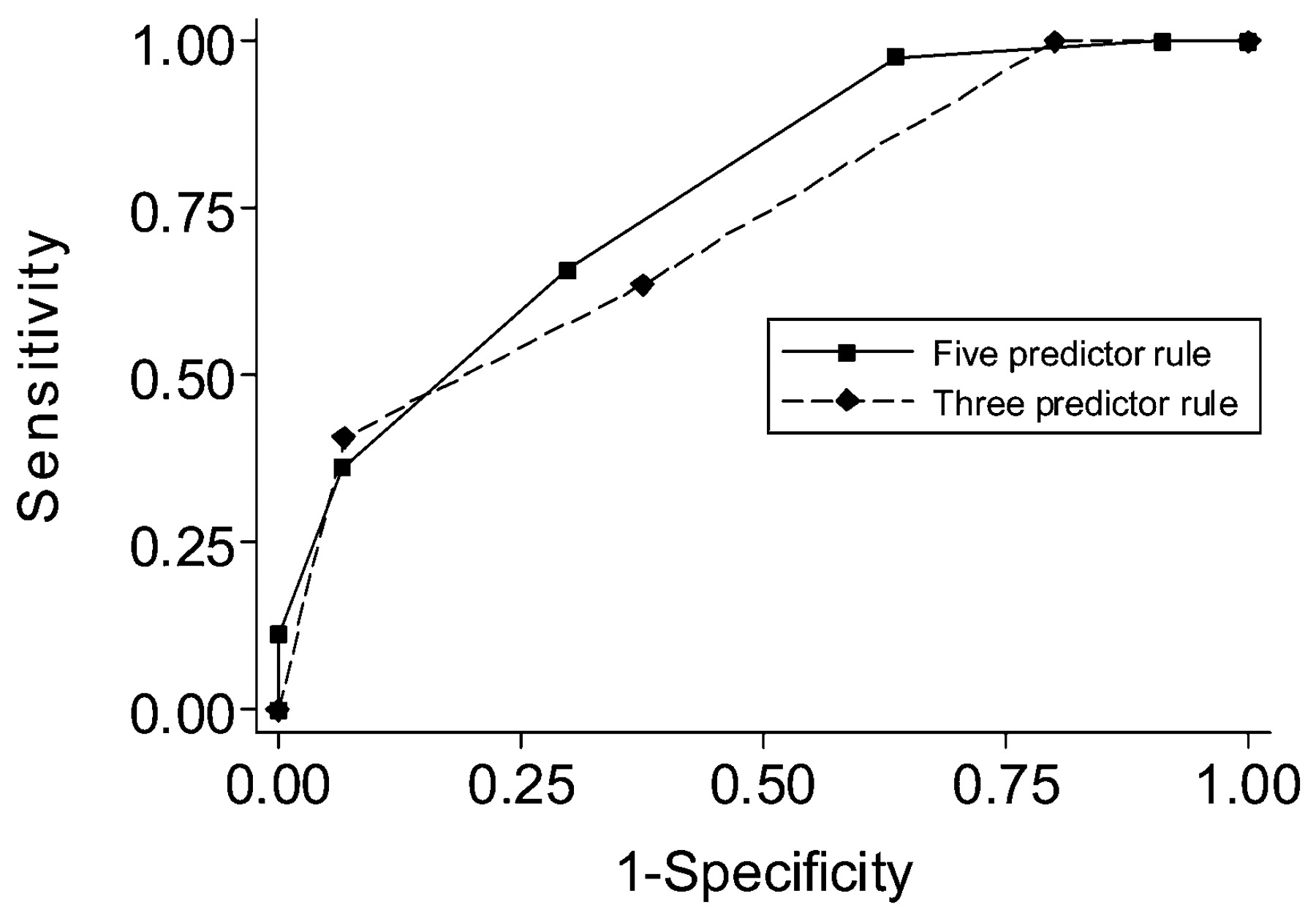
Based on the multivariate analysis results, we stratified patients by increasing risk for mortality using two prediction rules, both of which assigned one point for each predictor present. In the first rule, all five independent predictors from multivariate analysis were used to stratify patients by increasing mortality, resulting in a 6-point score (range 0–5). Mortality ranged from 4% (score 0 or 1) to 48% (score 4 or 5, fig 1). A simpler model based on three variables—age, A–a O2 gradient and serum albumin, resulted in a 4-point score (range 0–3) and stratified patients into groups with 0% mortality (score 0) to 41% (score 3, fig 2). The sensitivities, specificities, and positive and negative predictive values are given in table 4 and fig 3. While the 4-point score is simpler to use and requires less clinical information, model testing by the quasi-log-likelihood information criterion (QIC) indicated that the 6-point score was a better fit (6-point and 4-point QIC scores 232.3 and 241.9, respectively). The 4-point score also classified fewer patients than the full 6-point score into combined high and low mortality groups (109 vs 167 patients, 28% vs 46% of total patients, respectively).
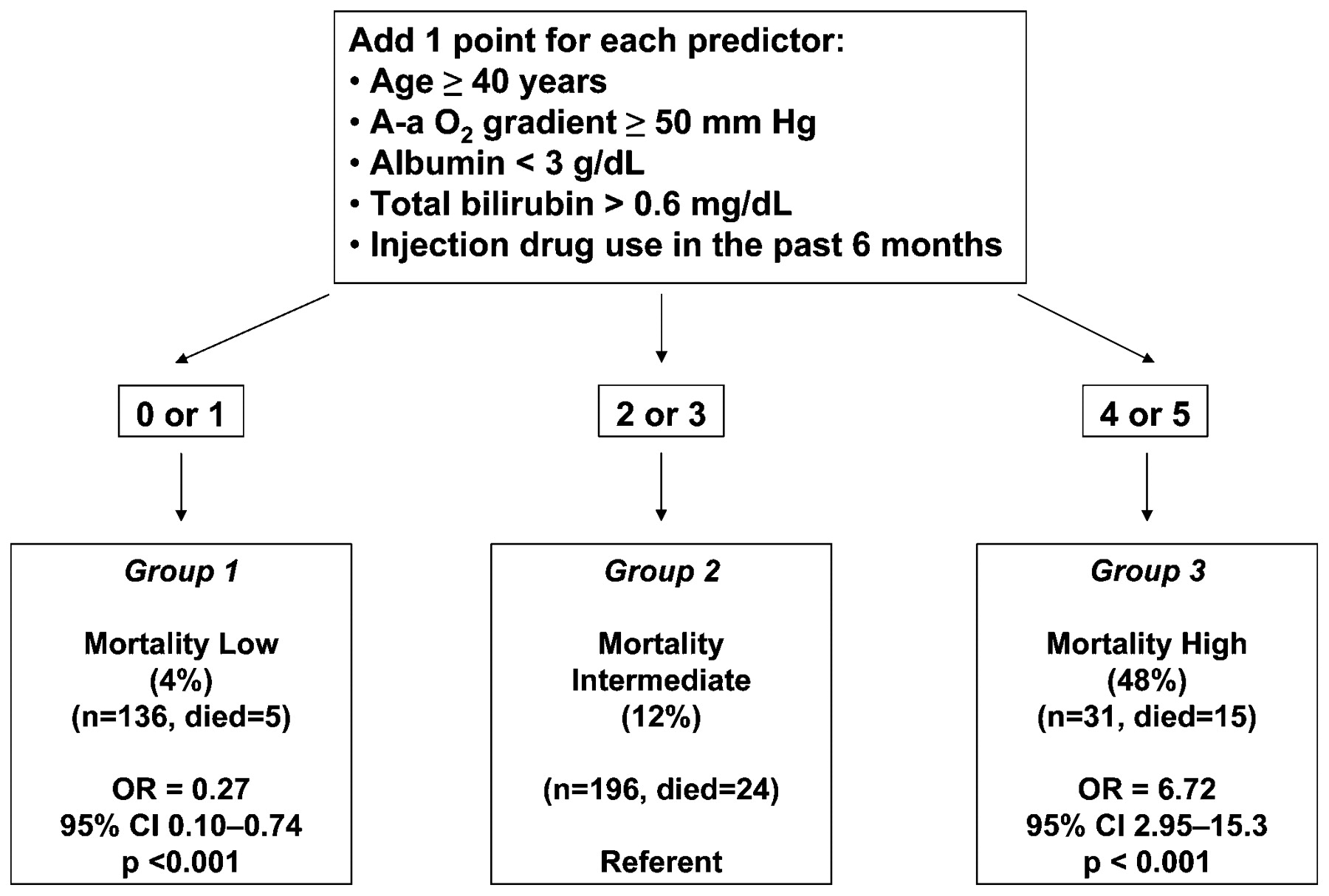
Stratifying patients with HIV-associated Pneumocystis pneumonia by mortality at illness presentation using all five predictors identified in multivariate analysis.

Stratifying patients with HIV-associated Pneumocystis pneumonia by mortality at illness presentation using three predictors—age, serum albumin and alveolar–arterial oxygen gradient (A–a O2 gradient)—identified in multivariate analysis.
{kind=link}
{kind=link}
{kind=link}
Receiver operating curves for the five-predictor and three-predictor PCP mortality prediction rules.
Test characteristics of mortality prediction rules for HIV-associated PCP
Discussion
In this single-centre study of 524 HIV-infected patients with laboratory-diagnosed PCP during the CART era, we found an overall mortality of 10.3% and identified five independent and objective predictors of mortality that are readily available at illness presentation. Using these predictors, we then developed two prediction rules that stratify patients by mortality risk upon presentation to medical care.
The overall mortality of 10.3% in our study cohort is within the range of mortality rates, 7–13%, reported in large cohorts (>500 subjects) of HIV-infected patients with PCP from the pre-CART and early CART eras,9 11 20 25 suggesting that mortality from PCP has not changed in the current era. Other studies, however, have documented a trend toward decreased PCP mortality in the CART era even in patients who were not receiving CART,18 a finding that has been attributed to improvements in ICU care.26 27 28 While the number of PCP cases per year has declined at our institution, those persons still presenting with PCP are rarely receiving antiretroviral therapy or PCP prophylaxis and still have an appreciable, and possibly unchanged, mortality.
We identified five significant and objective predictors of mortality that are readily available at illness presentation. Except for the A–a O2 gradient, none of the significant predictors of mortality identified in multivariate analysis was strictly associated with the severity of underlying HIV disease or respiratory compromise from PCP. Instead, our results suggest that non-HIV-associated factors that reflect the presence of underlying medical co-morbidities and general severity of illness, namely age, injection drug use, serum total bilirubin and serum albumin, may be more accurate predictors of mortality from PCP than HIV-associated factors, such as CD4 cell count or history of opportunistic infection. Age is a predictor that is widely used in risk stratification rules for community-acquired pneumonia, and correlates with the number of medical co-morbidities in HIV-infected patients.29 30 In addition, many studies have reported age and serum albumin as predictors of mortality not only for patients with PCP but also for HIV-infected patients requiring intensive care.12 18 19 20 31 To our knowledge, the associations between recent injection drug use and serum total bilirubin with increased PCP mortality have not been reported. Recent injection drug use increases the presence of concurrent medical co-morbidities and reflects the absence of appropriate, preventive medical care. Previous studies have either had a low prevalence of injection drug users or evaluated the association between any history of injection drug use and PCP mortality, which would include persons who had quit years previously.18 20 The serum bilirubin has been used in validated scoring systems (eg, Simplified Acute Physiology Score II, Pneumonia Severity Index) to assess severity of illness and predict mortality in patients with critical illness and pneumonia.30 32 As a reflection of end-organ dysfunction, bilirubin may also be a marker of sepsis or septic shock, and has recently been reported to predict development of acute respiratory distress syndrome and mortality in patients with sepsis.33
Both mortality prediction rules we present have distinct advantages. The three-predictor rule is easier to use and requires fewer clinical data, but classified fewer patients into groups with extremely high or low mortality compared with the five-predictor rule. Although the sensitivities and specificities of the two prediction rules were comparable, model testing using QIC scores showed that the five-predictor rule had a better fit. Two previous studies from the pre-CART and early CART eras have described strategies to predict mortality from PCP. One prediction model incorporated the A–a O2 gradient, total lymphocyte count and body mass index,9 while the other used HIV wasting, the A– a O2 gradient and serum albumin.20 However, both studies included patients who had presumptive PCP without microbiological confirmation. In addition, HIV wasting is subject to variability in provider categorisation and varying clinical manifestations, as noted by the study’s authors.20 34 In contrast, our mortality prediction rules are based on objective clinical and laboratory characteristics which are widely available and easily assessed in most HIV-infected patients presenting with PCP in high-income countries. Because our goal was to provide a simple, clinically useful prediction rule to identify patients at presentation with the highest and lowest risk for mortality, the algorithm has limited ability to stratify further patients with an intermediate mortality risk (Group 2, figs 1 and 2). At institutions where the risk of loss to follow-up is low, it is possible that persons who are predicted to have a low risk for mortality may not require admission for diagnosis and treatment. Similarly, persons who are predicted to have a high risk for mortality may warrant closer observation, such as on a “step-down” unit or in the ICU. Further research is needed to validate the predictive accuracy of our algorithm in patient cohorts from other institutions.
In addition to the limitations discussed above, our study’s main drawback is that it reflects the experience and patient population at a single public hospital in the USA and may not be more broadly applicable to all HIV-infected patients with PCP. Earlier studies have documented variations in patient demographics and processes of care among HIV-infected patients with PCP based on hospital type (ie, Veterans Affairs, public or private),35 and the high prevalence of injection drug use and sensitivity of sputum induction for PCP diagnosis in our study may make our findings less generalisable to other institutions. Our centre’s reliance on sputum induction rather than bronchoscopy for PCP diagnosis may explain why we did not identify pulmonary KS as a predictor of mortality, in contrast to findings reported by Walzer and colleagues at a centre that predominantly performs bronchoscopy for PCP diagnosis.18 We hope that our prediction rules will be validated using large cohorts of HIV-infected patients with PCP at other institutions, as has been recently described.17 18 Nevertheless, while sociodemographic characteristics, severity of illness and clinical practices may differ across patient cohorts and institutions, we believe that there is a biological basis and clinical rationale for the variables we identified to stratify patients by mortality. These are predictors which reflect presence of medical co-morbidity, severity of pulmonary disease and overall health status, and should be broadly applicable to most HIV-infected patients with PCP.
In conclusion, we found that mortality from HIV-associated PCP in the CART era remains unchanged from studies performed earlier in the HIV/AIDS epidemic. Using clinical and laboratory data routinely obtained at the time of presentation, we developed two mortality prediction rules that stratify patients by risk for in-hospital mortality. While our prediction rules require further validation in cohorts from different institutions, they are potentially a practical method of identifying patients who are at high and low risk for death early in the hospital course, and therefore may assist clinicians in assessing severity of illness and more accurately deciding on management strategies.
Acknowledgments
The authors would like to thank the staff of the San Francisco General Hospital medical records for help in locating all patient charts for this study.
REFERENCES
Footnotes
Funding This study was supported by National Institutes of Health Grants K24HL087713 and R01HL090335 (L.H), National Institutes of Health Grant F32HL088990 (J.L.D) and National Institutes of Health Grant T32HL007185 (M.W.F and E.J.K).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Ethics approval Ethics committee approval was obtained from University of California, San Francisco Committee on Human Research.