Article Text

Abstract
Background: Owing to its low incidence, the management of Mycobacterium xenopi pulmonary infections is not clearly defined. A multicentre retrospective study was performed to describe the features of the disease and to evaluate its prognosis.
Methods: All patients with M xenopi satisfying the 1997 ATS/IDSA criteria from 13 hospitals in north-east France (1983–2003) were included in the study. Clinical, radiological and bacteriological characteristics and data on the management and outcome were collected.
Results: 136 patients were included in the analysis, only 12 of whom presented with no co-morbidity. Three types of the disease were identified: (1) a classical cavitary form in patients with pre-existing pulmonary disease (n = 39, 31%); (2) a solitary nodular form in immunocompetent patients (n = 41, 33%) and (3) an acute infiltrate form in immunosuppressed patients (n = 45, 36%). 56 patients did not receive any treatment; the other 80 patients received first-line treatment containing rifamycin (87.5%), ethambutol (75%), isoniazid (66.2%), clarithromycin (30%) or fluoroquinolones (21%). After a follow-up of 36 months, 80 patients (69.1%) had died; the median survival was 16 months (range 10–22). Two independent prognostic factors were found: the acute infiltrate form was associated with a bad prognosis (hazard ratio 2.6, p = 0.001) and rifamycin-containing regimens provided protection (hazard ratio 0.325, p = 0.006). Clarithromycin-containing regimens did not improve the prognosis.
Conclusions: In contrast to recent guidelines, this study showed three different types of the disease (cavitary, nodular or diffuse infiltrate forms) with a different prognosis. In order to improve survival, all patients with M xenopi infection should be treated with a rifamycin-containing regimen. The usefulness of clarithromycin remains to be evaluated.
Statistics from Altmetric.com
Mycobacterium xenopi is a non-tuberculous mycobacterium responsible for lung disease,1 especially in north-east France, south-east UK and in Ontario, Canada.2 3 According to the recent ATS/IDSA statement, its usual feature is an apical cavitary process in patients with obstructive pulmonary disease.4 However, other features have been described.5 M xenopi infections are difficult to treat and there is no standard treatment.2 3 5 Rifampin, ethambutol and sometimes isoniazid or fluoroquinolones are usually recommended in combination with clarithromycin.4 Two randomised clinical trials have been conducted by Jenkins et al.6 7 In the first study, 42 patients were treated with rifampin and ethambutol with or without isoniazid, without any difference in the clinical response.6 The overall mortality rate at 5 years was 69%. In the second study, Jenkins et al compared clarithromycin with a ciprofloxacin-containing regimen in 371 patients infected with non-tuberculous mycobacteria and found no difference in the 34 patients infected with M xenopi.7
As M xenopi infection could present with different clinical and radiological patterns depending on the patient’s immunological status, we conducted a multicentre retrospective study to determine the clinical and radiological characteristics of patients with M xenopi infection and to evaluate the 36-month survival rate and prognostic factors.
METHODS
In 13 hospitals in north-east France (the “Xenopi Group”), the clinical files and bacteriology laboratory data were reviewed for all patients with at least one pulmonary bacteriological specimen positive for M xenopi between 1 January 1983 and 31 December 2003. To be included, patients had to be aged >18 years and to fulfil the 1997 ATS diagnostic criteria for non-tuberculous mycobacterial pulmonary infection.8
Definitions and recorded data
Clinical, radiographic and microbiological data were collected for patients with documented M xenopi infection (defined according to the 1997 ATS criteria). Radiographic abnormalities (nodular, infiltrative or cavitary) were analysed by chest radiography and/or CT scanning. Treatments were identified as first, second and third drug combinations, taken for at least 1 month. Outcomes were defined as cure, relapse or death. Patients were considered to be cured when there was no specimen culture positive for M xenopi during the last 3 months of treatment and 3 years after discontinuation of treatment. However, as such bacteriological follow-up was not systematically performed, patients were also considered to be cured when no relapse was observed during the 3 years after finishing treatment. For patients who died, the cause of death was noted. Survival at 36 months was chosen as the primary end point in the survival analysis. Prognostic factors among the recorded clinical, radiographic and microbiological characteristics and treatment were sought. We also evaluated the specific role of each molecule in the survival analysis. The data were checked for a possible period effect (before and after 1997) because highly active antiretroviral therapy (HAART), available since 1996, has improved the prognosis of HIV-infected patients.
Statistical analysis
Statistical analysis was performed with SPSS 12.0 software. Descriptive analysis of continuous quantitative variables is expressed as mean (SD) and qualitative variables as frequency (%). Univariate comparative analysis was performed with the Fisher exact text for qualitative variables and a Student t test or a Kruskal–Wallis non-parametric test for continuous variables. Univariate survival analysis was performed with a Kaplan–Meier non-parametric test and multivariate analysis with a Cox model. A p value <0.03 was considered to be statistically significant and was chosen according to the Bonferroni method in order to integrate the interim analysis.9 Percentages are expressed in relation to the total population unless otherwise specified.
RESULTS
During the period from 1983 to 2003, 180 patients with at least one positive specimen for M xenopi were eligible. Forty-four patients (24%) were considered to be colonised by M xenopi and were excluded. The remaining 136 patients (104 men, 32 women, mean age 53 (16) years, median 53 years (range 20–91)) met the criteria required by the 1997 ATS (and also the 2007 ATS/IDSA criteria) and were included in the study.4 8
Population
One hundred and twenty-four patients (91%) had co-morbidities—a history of systemic immunosuppression in 52.2% and/or local pulmonary immunosuppression in 56%. The characteristics of the patients are shown in table 1.
Imaging
A chest radiograph was available for 130 patients and was found to be abnormal in 125 cases (96%). A CT scan, performed in 71 patients, was always abnormal. Unilateral or bilateral apical shadows (nodule, cavitary and infiltrate) were observed in 55 patients (55/125, 44%) and were more frequently located in the right upper lobe (53/125, 42%; fig 1).
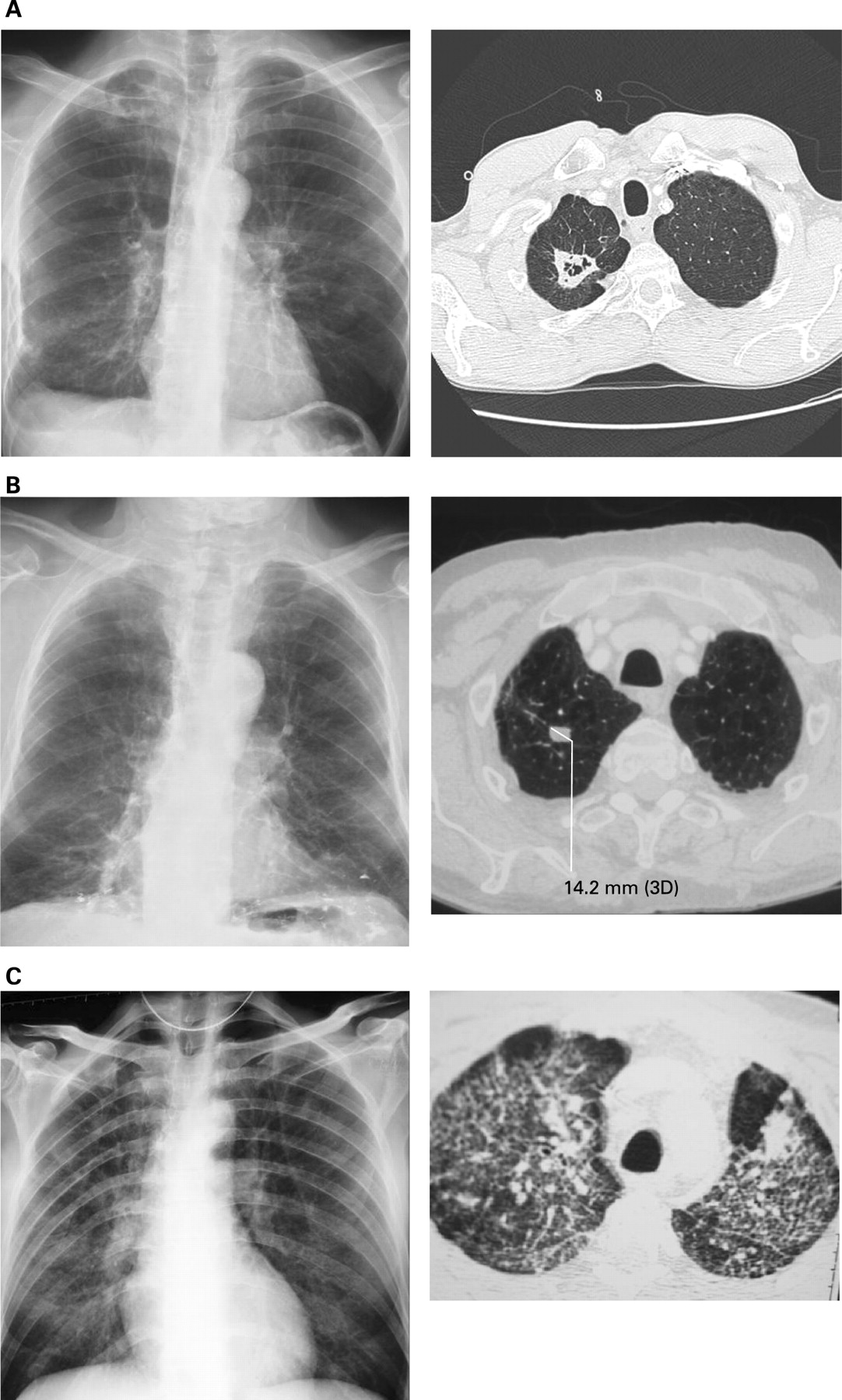
Chest radiograph and CT scan of (A) cavitary form, (B) nodular form and (C) infiltrate form.
Microbiology
A median of 3 (range 1–11) specimens were obtained with a median of 3 (range 1–11) positive specimens: sputum culture (n = 78, 57.4%), bronchoalveolar lavage fluid (n = 57, 41.9%), bronchial aspirate (n = 38, 27.9%), gastric fluid (n = 20, 14.7%), surgical biopsy (n = 8, 5.8%), bronchial biopsy (n = 4, 2.9%) and autopsy (n = 6, 4.4%). Eighty-three patients had one or more smear positive. The median time to diagnosis was 2 months (range 1–60). Antibiotic susceptibility testing was performed in 58 cases (44%). The strains were reported as resistant to isoniazid in 75%, to rifampin in 40%, to ethambutol in 24% and to clarithromycin in 2.5%. Co-infections were found in 23 patients (Aspergillus fumigatus in 14 and Pneumocystis jiroveci in 9).
Typology of M xenopi pulmonary infection
The typology of M xenopi pulmonary infection was established for the 125 patients with an abnormal shadow on the chest radiograph. Three radiological patterns were distinguished: the cavitary form (39/125, 31%), the nodular form (41/125, 33%) and the infiltrate form (45/125, 36%; fig 1 and table 1).
In 39 patients the radiographic appearance was a cavitary process. An underlying lung disease was significantly more frequent in these patients than in other patients (77% (30/39) vs 45% (39/86), p = 0.009). For these patients, all specimens were positive.
Forty-one patients presented with a nodular radiological form. Most of them had no co-morbidity compared with patients with other patterns (22% (9/41) vs 2% (2/84), p = 0.001). Five cases (12%) in this subgroup required surgical biopsy for diagnosis.
The remaining 45 patients showed an infiltrate radiological form. These patients were significantly younger than the other patients (48 years vs 54 years, p = 0.031) and associated co-morbidities were significantly more frequent (100% (45/45) vs 86% (69/80), p = 0.015), especially HIV-associated systemic immunosuppression (58% (26/45) vs 13% (10/80), p<0.001), with a lower incidence of underlying pulmonary disease (36% (16/45) vs 66% (53/80), p = 0.002) in this subgroup. Bronchoalveolar lavage was required more frequently in this subgroup for diagnosis (61% vs 32%, p = 0.002).
Treatment regimens
Fifty-six patients (41.2%) did not receive any drug and 21 patients died before the bacteriological diagnosis was made. Surgical resection was proposed in 6 patients (8%). Physicians decided to withhold treatment in 35 patients, especially in those with the nodular form (51.2% vs 30.9% in the other patterns, p = 0.03). Patients with a cavitary process were treated more frequently than the other patients (83.3% vs 54.7%, p = 0.004; see fig 3 in online supplement). Patients with a positive smear were treated more frequently (75.9% vs 32.1%, p<0.001). First-line drug combinations that contained an average of four antibiotics consisted of a combination of a rifamycin (70/80, 88%: rifampicin, n = 58; rifabutin, n = 12) and/or ethambutol (60/80, 75%) and/or isoniazid (53/80, 66%) and/or clarithromycin (24/80, 30%) and/or a fluoroquinolone (17/80, 21%: ofloxacin, n = 14; ciprofloxacin, n = 3). The median duration of the first-line drug combination was 5 months (range 1–72). Twenty-eight of these 80 patients received a second drug combination containing clarithromycin (23/28, 82.1%) and/or a fluoroquinolone (17/28, 60.7%) and/or a rifamycin (16/28, 57%) and/or ethambutol (13/28, 46.4%) and/or isoniazid (5/28, 18%), with a median duration of 5 months (range 1–12) (see fig 4 in online supplement). Only 13 patients (9.5%) received a third drug combination. The mean total duration of treatment was 9 months (range 2–25) with 34 adverse effects that required changes in treatment.
Outcome
Fourteen of the 136 patients were lost to follow-up. Survival analysis was therefore based on the remaining 122 patients. Twenty-six patients achieved a “clinical” cure and 7 fulfilled the criteria for a bacteriological cure. Twenty-one relapses were diagnosed after a median period of 5 months (range 1–40), 14 of whom were treated. The only significant predisposing factor to relapse was a treatment duration <6 months (85% vs 36%, p = 0.03).
The median survival of these 122 patients was 16 months (range 10–22). Twenty-one patients died before the bacteriological diagnosis and 26 before the planned end of treatment. When a follow-up of 36 months was applied, 80 patients (69.1%) had died at this end point with a median time to death of 9 months (range 1–120). Deaths were attributed to M xenopi infection in 49 cases (61.2%), to the underlying disease in 24 (30%) and to another cause in 7 cases (8.7%).
Prognostic factors (Kaplan–Meier univariate analysis)
Prognostic factors according to the Kaplan–Meier univariate analysis are shown in table 2 in the online supplement.
Clinical characteristics
Immunosuppression was found to be a poor prognostic factor (11 months vs 30 months, p = 0.002; hazard ratio (HR) 2.8 (95% confidence interval (CI) 1.3 to 6.2), p = 0.007). We found a period effect on survival (12 months before 1997 and 20 months after 1997 (HR 1.5 (95% CI 1.0 to 2.3), p = 0.05)) and, when patients were stratified according to HIV status, median survival improved after 1997 only in HIV-infected patients (p = 0.002).
Clinical and radiological patterns
When survival was analysed according to the three radiological patterns, a significantly longer survival was observed in patients with the nodular form (24 months vs 13 months, p = 0.039; HR 0.42 (95% CI 0.18 to 0.96)), whereas the worst prognosis was observed with the diffuse infiltrate pattern (9 months vs 25 months, p<0.001; HR 3.48 (95% CI 1.29 to 9.40)).
Microbiology data
For bacteriological results, no difference in survival was observed between positive or negative smears (p = 0.2) and between susceptible and resistant strains either to rifampicin, ethambutol or clarithromycin.
Treatment regimens
The absence of treatment was a factor for a poor prognosis, with a median survival of 10 months in untreated patients and 32 months in treated patients (HR 3.04 (95% CI 1.94 to 4.74), p<0.001; fig 2). Rifamycin-containing regimens were associated with a significant improvement in the median survival (p<0.001 in first-line drug combinations and p = 0.03 in later drug combinations; see fig 5 in online supplement). Similar findings were observed with rifamycin+ethambutol-containing regimens (p = 0.001 and p = 0.01, respectively; see fig 6 in online supplement). Clarithromycin, either as first-line (p = 0.18) or any drug combination, did not influence the prognosis (p = 0.57; see fig 7 in online supplement). For ethambutol, the significant improvement in survival observed in first-line drug regimens (p = 0.01) was not found for other regimens (p = 0.88). Similar findings were observed for isoniazid (p = 0.013 and p = 0.79 for first-line and later combinations). No significant difference in survival was observed with fluoroquinolones. First-line surgery was associated with an improvement in survival (p = 0.04). An interaction study with rifamycin-ethambutol, rifamycin-clarithromycin and rifamycin-isoniazid did not demonstrate any significant synergistic activity. A treatment duration of ⩽6 months was a poor prognostic factor (p = 0.008).

{kind=link}
{kind=link}
Cumulative survival according to whether or not the patient was treated. Treatment is defined as the use of a combination of antibiotics for at least 1 month, or surgical management, or the combination of medical and surgical treatment.
Prognostic factors (multivariate analysis according to the Cox model)
The following variables were entered into the model: systemic immunosuppression, infiltrate radiological pattern, rifamycin-containing regimen, ethambutol-containing regimen and clarithromycin-containing regimen. Two independent prognostic factors were found: the presence of the infiltrate radiological pattern was associated with a bad prognosis (HR 2.60 (95% CI 1.44 to 4.45), p = 0.001) while combination therapy with a rifamycin-containing regimen was found to be a protective factor (HR 0.33 (95% CI 0.15 to 0.72), p = 0.006). The presence of systemic immunosuppression tended to be associated with a poor prognosis (HR 1.87 (95% CI 1.09 to 3.27), p = 0.039).
DISCUSSION
Despite the fact that recent guidelines have considered M xenopi infection to be a single disease (cavitary form),4 our results support a new approach based on three clinical and radiological features: nodular, cavitary and infiltrate forms.
The cavitary form, which accounted for 31% of our cases, corresponds to the “classical” type with a clinical presentation similar to that of tuberculosis and a diagnosis easily made from sputum smears.4 10–12 It is mainly observed in patients with an underlying pulmonary disease (such as chronic obstructive pulmonary disease or bronchectasis). The nodular form, which is often observed in immunocompetent adults, is the least aggressive form and often has a delayed diagnosis. The main danger in this form is to consider a positive sample as a contaminated specimen and then not to repeat the samples. The diffuse infiltrate form, which is mainly observed in young immunosuppressed patients (mainly by HIV infection), is the most serious form of M xenopi infection. More aggressive methods are usually required to assess the diagnosis (repeated bronchoalveolar lavage and/or transbronchial biopsies).
In our patients, M xenopi infection appeared to be a disease with a 3-year mortality rate of 69.1% and a mean time to death of 9 months.
Like other authors,13–16 we have questioned the value of treatment. The only independent modifiable prognostic factor we found for the whole group, whatever the feature (nodular, cavitary or infiltrative form), was active treatment, particularly rifamycin-containing regimens. Owing to the lack of randomised trials and the lack of agreement in guidelines, the choice of drugs remains difficult. Treatment could be based on antibiotic susceptibility testing but many M xenopi strains appear to be resistant to rifampicin, isoniazid and ethambutol in vitro.17 18 As in our study, an absence of in vitro/in vivo correlation has been emphasised in the literature.6 9 19 20 In contrast with in vitro data and according to our results, treatment should contain a rifamycin, which is also recommended by the American Thoracic Society and the British Thoracic Society.2 4 8 21 Clarithromycin, which shows excellent in vitro activity,17 did not appear to improve survival in our study, whether administered as first-line treatment or later. With regard to the usefulness of clarithromycin, the only in vivo study was conducted in mice18 and other publications are isolated case reports.22 Juffermans et al reported the almost complete absence of in vitro resistance to clarithromycin but failed to find any improvement in outcome with this drug.23 Arguments in favour of the in vivo efficacy of clarithromycin on M xenopi are based on the in vivo efficacy of clarithromycin on Mycobacterium avium intracellulare complex.24 25 On the basis of a single unpublished abstract,26 clarithromycin has been recommended since 1997.4 8 Since this date, only one randomised study has been published which did not observe any difference in mortality between the clarithromicyn and ciprofloxacin treatment arms.7 This result is difficult to interpret due to the small number of patients (17 in each group). Ethambutol appears to be useful as it promotes the in vivo penetration of other antibiotics such as rifamycin into mycobacteria.17 27 Ethambutol was found to be a good prognostic factor, but not an independent one, probably because it is usually associated with a rifamycin. Surgery, which in our study was associated with a significantly prolonged survival, was performed for diagnostic purpose in patients whereas, in the literature, it has been reserved for cases of chemotherapy failure in patients with localised lesions.2 8 28 29
In conclusion, M xenopi infection remains difficult to diagnose and requires microbiological assessment whatever the radiological features. This infection should no longer be considered as a uniform disease as we were able to distinguish three radiological forms. The cavitary form usually occurred in patients with underlying pulmonary disease, the nodular form in immunocompetent patients and the diffuse infiltrate form usually affected young immunosuppressed patients. The prognosis of M xenopi infection remains extremely poor, and rifamycin-containing regimens must be prescribed in all patients except those in which it is contraindicated. As yet there is no evidence of any benefit of adding clarithromycin to the treatment regimen, but a controlled study is needed to confirm this.
Acknowledgments
The authors acknowledge the following members of the Xenopi Group: Arras (Dr Bervar, Noulard); Besançon (Professor Hoen and Professor Plesiat); Compiègne (Dr Merrien); Creil (Drs Lamarck, Lemaitre and Merour); Dijon (Professor Chavanet and Professor Kazmierczak); Lens (Dr Bure and Dr Canonne); Lille (Professor Wallaert and Dr Wallet); Nancy (Professors Martinet et May, Dr Dailloux); Reims (Drs Deslee, Strady et Vallerand, Professor De Champs de Saint Léger); Saint Quentin (Drs Albertini and Dayen); Strasbourg (Professors Martin, Monteil, Pauli and Weitzenblum); Tourcoing (PrYazdanpanah and Dr Dhennain). They also acknowledge the InterCISIH Nord-Est for this collaboration and Professor Jacques Grosset for his advice.
REFERENCES
Supplementary materials
web only appendices 64/4/291
Files in this Data Supplement:
Footnotes
↵* The list of participants appears at the end of the paper.
▸ Table 2 and figs 3–7 are published online only at http://thorax.bmj.com/content/vol64/issue4
Funding: None.
Competing interests: None.