Article Text

Abstract
Objectives: To determine whether well trained lay people could deliver asthma self-management education with comparable outcomes to that achieved by primary care based practice nurses.
Design: Randomised equivalence trial.
Setting: 39 general practices in West London and North West England.
Participants: 567 patients with asthma who were on regular maintenance therapy. 15 lay educators were recruited and trained to deliver asthma self-management education.
Intervention: An initial consultation of up to 45 min offered either by a lay educator or a practice based primary care nurse, followed by a second shorter face to face consultation and telephone follow-up for 1 year.
Main outcome measures: Unscheduled need for healthcare.
Secondary outcome measures: Patient satisfaction and need for courses of oral steroids.
Results: 567 patients were randomised to care by a nurse (n = 287) or a lay educator (n = 280) and 146 and 171, respectively, attended the first face to face educational session. During the first two consultations, management changes were made in 35/146 patients seen by a practice nurse (24.0%) and in 56/171 patients (32.7%) seen by a lay educator. For 418/567 patients (73.7%), we have 1 year data on use of unscheduled healthcare. Under an intention to treat approach, 61/205 patients (29.8%) in the nurse led group required unscheduled care compared with 65/213 (30.5%) in the lay led group (90% CI for difference −8.1% to 6.6%; 95% CI for difference −9.5% to 8.0%). The 90% CI contained the predetermined equivalence region (−5% to +5%) giving an inconclusive result regarding the equivalence of the two approaches. Despite the fact that all patients had been prescribed regular maintenance therapy, 122/418 patients (29.2%) required courses of steroid tablets during the course of 1 year. Patient satisfaction following the initial face to face consultation was similar in both groups.
Conclusions: It is possible to recruit and train lay educators to deliver a discrete area of respiratory care, with comparable outcomes to those seen by nurses.
Trial registration number: NCT00129987
Statistics from Altmetric.com
Worldwide, 300 million people have asthma; 5.2 million have the condition in the UK.1 Most of these will have limited contact with healthcare professionals during any one year and will “self-manage” their own condition for most of the time. National2 and international guidelines3 stress the importance of health professionals providing self-management education to ensure that those with asthma recognise deteriorating symptoms, know how to monitor their own condition and know how to adjust therapy themselves and when to seek medical attention. Numerous studies and systematic reviews4 have shown the effectiveness of self-management education monitoring and follow-up in terms of reduction in the need for unscheduled healthcare and reduction in symptoms and time off work and school. One constituent of self-management education is the receipt by patients of a written personalised asthma action plan and other reviews have demonstrated the important actions to be included in such a plan.5
If receipt by the patient of a written personal asthma action plan is taken as a marker of the frequency with which self-management education is offered, the results of studies in the UK and elsewhere suggest that 17 years after guidelines first promoted this approach to management,6 it is poorly implemented. The reasons for poor implementation are not clear. Patients, including those in minority ethnic groups,7 have a desire for greater involvement in treatment decisions8 and welcome receipt of personal action plans.9 There are a number of reasons why health professionals may fail to implement guideline recommendations, both in general and specifically with regards to self-management,10 and their attitudes to self-management have been studied.11 Alternatives to health professional delivery of patient education programmes need to be explored. Such alternatives might include web based programmes,12 lay led self-help educator programmes13 or nurse delivered education. In the UK, routine follow-up and supervision of those with asthma is normally undertaken by primary care practice based nurses,14 but recent studies have shown that only between 3% and 20% of those with asthma in the UK9 15 have received personalised asthma action plans. We have therefore explored whether lay people who have been appropriately trained can be used to offer self-management education to adults with asthma and whether the outcomes are equivalent to those achieved by nurse led education.
METHODS
We carried out a randomised equivalence trial, the central hypothesis being that well trained lay people could offer self-management education to adults with asthma with results which would be equivalent to nurse led education.
Thirty-nine general practices in West London and North West England were recruited to the study. Their asthma registers were systematically sampled by a research assistant, followed by casenote review. Eligible patients were adults over the age of 18 years with clinician diagnosed asthma with persistent disease requiring regular preventative therapy, who had evidence of variability of their disease necessitating unscheduled healthcare or a course of steroid tablets in the 12 months prior to recruitment. Patients already in receipt of a written personal asthma action plan were excluded from the study. Every effort was made to recruit according to the ethnic diversity of the study population and to recruit patients with disabilities (eg, visual impairment or functional illiteracy). The initial intention was to recruit 30 patients from each general practice from 16 sites in London and 16 sites in Manchester. This would give a total of 960, and allowing for a one-third dropout rate, we anticipated 20 patients completing follow-up at each site, giving an anticipated sample size of 640 patients completing the study (320 in each arm). Using unscheduled use of healthcare as the primary outcome, we extrapolated from national data which suggested a likely hospital admission rate of 7.4 per 10 000 practice patients aged more than 16 years, and 557 adults seeking treatment in primary care at least once in a year per 10 000 practice patients, which gave an overall anticipated 6% occurrence of unscheduled health services use in the study patients. Allowing for a 5% difference in such consultations between the nurse and lay led group, a sample size calculation using n-Query Advisor indicated that a minimum of 279 patients was required in each arm in order to reject the null hypothesis that lay led and nurse led education were not equivalent (0.05 significance level, 80% power). Random allocation of patients to the group was performed using the Clinstat program (http://www-users.york.ac.uk/∼mb55/soft/soft.htm). A random allocation sequence was generated for each of the 32 sites using blocks of size 4 to maintain balance within potentially small sites. Blinding was not possible, but the random allocation was concealed from the educators until the interventions were assigned, and the individual generating the random sequences was not involved in the interventions.
The intervention was a disease specific asthma self-management education programme delivered either by a practice nurse or by a lay person. A total of 15 lay trainers were recruited by advertisement and the criteria for selection were that the trainer or a close relative had to have asthma. No minimum educational qualifications were stipulated. After recruitment, the lay persons underwent a specially constructed 2 day residential training course at the National Respiratory Training Centre (NRTC) (now part of Education for Health) followed by a distance learning programme, and three reinforcing 1 day training sessions with an NRTC trainer, followed by regular monthly opportunities for training, support and answering of queries from clinicians and researchers involved in the study on both sites. Lay educators were paid £8.00 per hour (€11.98/$15.28). All 46 nurses undertook a 1 day NRTC update programme and received specific training on writing personal asthma action plans and on the study protocol. It was emphasised to the general practitioners that the lay educators would be teaching the patients entirely in line with the recommendations in the British Asthma Guidelines2: for quality assurance, the lay educators’ early consultations were observed to ensure that they were practising as taught.
The major part of the intervention was an initial consultation of up to 45 min in which either the nurse or lay person delivered an individualised training session for each patient, and to follow this up with a second face to face reinforcing session of up to 30 min duration, 3 weeks after the first session. Topics addressed during consultations were those recommended in national and international asthma guidelines and identified in relevant reviews as effective elements of self-management education, and included aetiology of asthma and the long term nature of the disease; asthma medications and their uses; asthma triggers and allergen avoidance; and recognition of the signs of worsening asthma and appropriate action to take. To further promote provision of guidelines based care, both nurses and lay educators completed a guidelines based patient history sheet and proforma for each consultation. A standard written asthma action plan template was provided for all educators in the study and this was individualised for each patient, advising them when to increase their routine preventative therapy, when to start a course of steroid tablets and when to seek urgent medical attention (see appendix available online). Reinforcing written materials about asthma and its treatment were provided to all educators from the charity, Asthma UK. The initial face to face consultations were planned to be followed by a telephone follow-up call every 3 months for 1 year to reinforce messages and to give ongoing advice. The nurses and lay educators were available as a source of advice at other times; the practice nurses in the normal manner and the lay educators were provided with a mobile telephone which the patients were able to contact to leave a message to clarify any issues which had been discussed and which had not been fully understood. In order to minimise contamination, patients who were randomised to care from a lay educator signed an agreement to seek advice from a practice nurse only in an emergency.
While unscheduled use of health services (one or other of a hospital admission, emergency department attendance, unscheduled consultation with a GP) was the primary outcome, patient satisfaction with their consultations was also assessed using the MISS-21 Medical Interview Satisfaction Scale16 adapted for this purpose with the collaboration and permission of the originators.
After each consultation or patient contact, the nurses or lay educators completed data forms which were collected from each practice by a research assistant. At the end of the study all patients who had been randomised were contacted to collect self-reported information regarding need for unscheduled healthcare and courses of oral steroids used. This was validated wherever possible against GP records. Those not responding to the initial mailing were contacted up to three further times.
The data were entered into and analysed descriptively using SPSS. The main outcome measure, percentage with unscheduled use of healthcare services, was compared between groups using a two sided 90% confidence interval (CI) for the difference; if the confidence interval lies within the prespecified equivalence region (−5% to 5%), then the experimental treatment (lay led education) is considered to be equivalent to the control treatment (nurse led education) at a significance level of 5% according to the sample size calculation.17 It was also compared between the groups using the more usual 95% CI for the difference.18 CIs were estimated using Newcombe’s method19 via an Excel spreadsheet written by Newcombe (http://www.cardiff.ac.uk/medicine/epidemiology_statistics/research/statistics/newcombe/proportions). Mean scores for MISS-21 in the two groups were compared using the t test with a significance level of 5%.
RESULTS
Thirty-nine practices initially agreed to take part in the study but eight dropped out. Patients were recruited and followed-up between January 2004 and August 2006. The responses to invitation letters are shown in table 1; 567 eligible patients were randomised (287 to nurse educators and 280 to lay educators), and details of retention are shown in fig 1. There were no noticeable differences between the two arms of the study in the characteristics of the patients at baseline or after 12 months of follow-up (table 2). Patients randomised to see a lay educator were more likely to attend their first consultation (61.1%) than were those allocated to see a nurse (50.9%) (χ2 = 5.98, df = 1, p = 0.015) and similarly more likely to provide 12 month follow-up data.

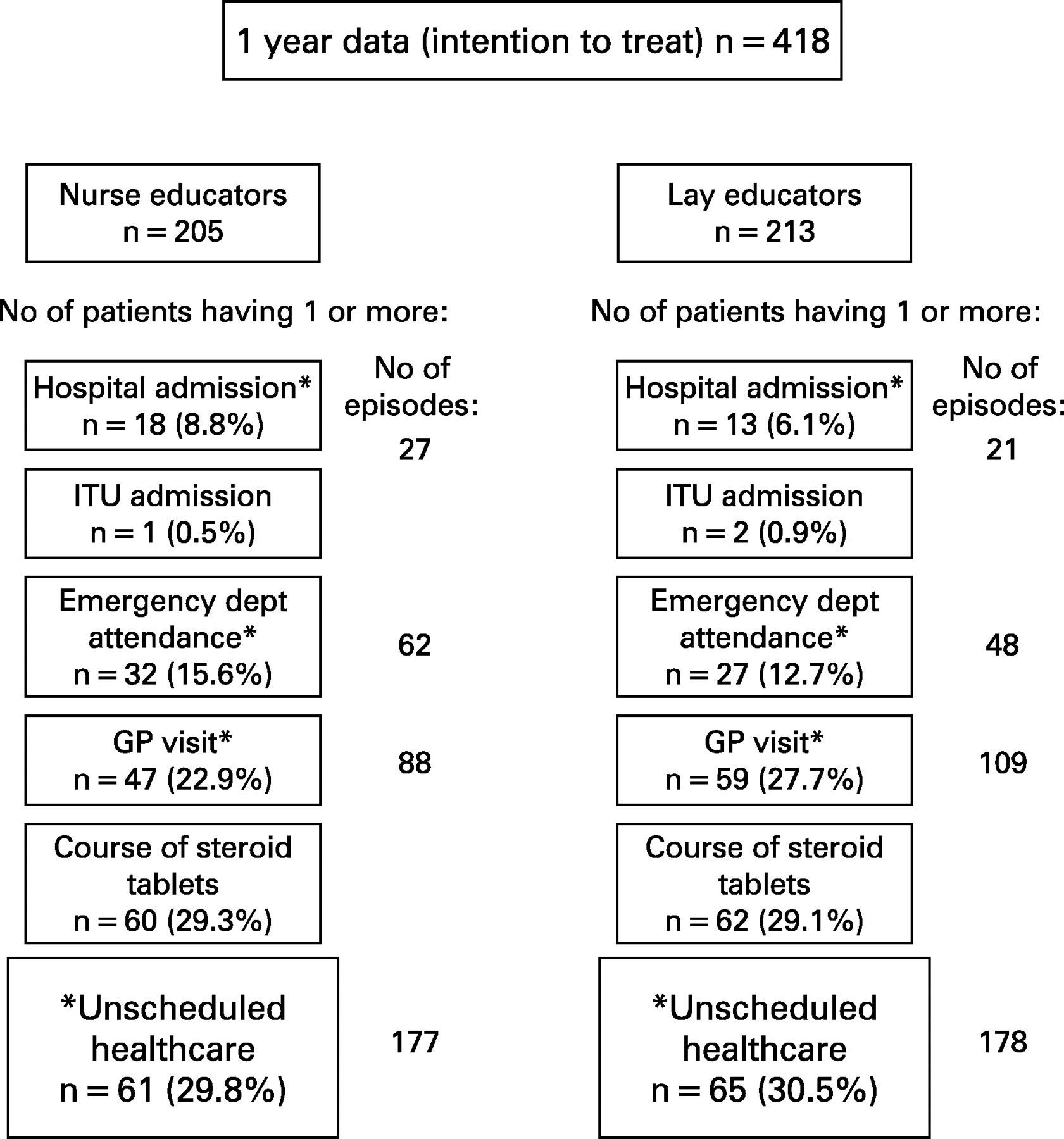
During the first two consultations, changes were made to the patients’ medication, inhaler device or dosage (including reductions) in 35 of the 146 patients seen by a practice nurse (24.0%) and in 56 of the 171 patients (32.7%) seen by a lay educator. For 418 of the 567 patients (73.7%) we had 1 year data on use of unscheduled healthcare. These results are presented in fig 2, from which it can be seen that the numbers of patients requiring hospital admission, emergency department attendances or unscheduled general practitioner consultations were almost identical in the nurse and lay led groups. (If a patient attended the emergency department, and on the same occasion was admitted to hospital, this is counted as one episode of unscheduled healthcare.) Under an intention to treat approach, 61/205 patients (29.8%) in the nurse led group required one or other of these three services, compared with 65/213 (30.5%) in the lay led group (90% CI for difference −8.1% to 6.6%; 95% CI for difference −9.5% to 8.0%). The 90% CI for the difference between percentages contained the predetermined equivalence region (−5% to 5%), so that statistically there was an inconclusive result regarding equivalence. Despite the fact that all of the patients in the trial had been prescribed regular maintenance therapy, 122/418 patients (29.2%) required courses of steroid tablets during the course of 1 year of follow-up. Thirty-one patients were admitted to hospital on 48 occasions, 59 had emergency department attendances on 110 occasions and 106 had a need for an unscheduled general practitioner consultation on 197 occasions.

{kind=link}
{kind=link}
Complete records of patient satisfaction were obtained after the first face to face consultation for 259 patients (124 nurse educated patients and 135 lay educated patients). The practice nurses’ mean total score was 119.9 (SD 15.3) and that for the lay educators was 120.6 (SD 14.8) (unpaired t = 0.37, df = 257, two sided p = 0.432, 95% CI for difference −4.4 to 3.0).
There were only seven protocol violations. Three patients randomised to a lay educator were seen by a nurse. In three cases the opposite occurred. One patient saw the general practitioner instead at an appointment arranged by the nurse.
Fifteen lay educators were recruited for this study. Five had left school at the age of 16 years and 10 left school at the age of 18 years. Among the latter, seven undertook non-graduate further education and two had completed a university degree course. Of the 15, nine (60.0%) dropped out over the subsequent 22 months: four left the study for health reasons and three for personal reasons (one was counselled out of the study because of difficulties meeting study responsibilities due to home commitments, two due to family circumstances) and one had to leave the trial because of changes in work circumstances. Contact was lost with one lay educator for reasons which are not known. Forty-six practice nurses were initially recruited and trained for this study, of whom 21 (45.6%) dropped out over the subsequent 22 months: 10 left the practice, others took maternity leave, were promoted, took indefinite sick leave, handed over work to another nurse or no longer wished to be involved in the project, and three left because their practice no longer wished to be involved in the study.
DISCUSSION
This is a report of an ambitious study. The numbers we intended to recruit would have represented one of the largest self-management education studies ever undertaken in asthma. We were able to recruit an excellent cross section of patients and we achieved our goal of satisfactory ethnic diversity. Analysis was performed on an intention to treat basis, and the results demonstrate that clinical outcomes for those seen by lay educators were highly comparable with those achieved by patients seen by a primary care practice based nurse. During the consultations, lay educators were as likely as nurses to recommend meaningful changes to management and patients were as satisfied with care by a lay educator as with care by a nurse.
We had intended to offer education to 640 patients but eventually recruited only 567 patients. Patients with asthma frequently do not maintain contact with healthcare professionals9 and in this study 44.1% of those who consented to take part in the study could not in the event be persuaded to attend to undergo their education. In a previous systematic review of self-management education in asthma,4 6090 participants were randomised into 36 trials. The reported dropout rates ranged from 0% to 54%. The size of this problem needs to be taken into consideration when planning future trials. A total of 317 of our patients attended for their first consultation but only 251 for the second. The fact that more patients randomised to the lay educators attended than did those in the nurse group probably reflects a greater persistence by the lay educators to contact the patients and invite them to attend. The proportion having subsequent reinforcing telephone consultations was lower, and discussion with nurses and lay educators suggested that this part of the protocol was probably over complicated, but it was equally difficult for nurses as for lay educators. While the dropout rates had been taken into consideration in our power calculations, we had not anticipated 30% of patients needing unscheduled healthcare during the 12 month follow-up period. It is important in asthma self-management trials to avoid only recruiting those with well controlled asthma, hence giving no opportunity for the patient to self-manage and alter outcomes. For this reason we specifically aimed to recruit patients with a history of poorly controlled asthma, and in so doing almost certainly increased the rate of subsequent need for unscheduled healthcare to above that anticipated. Since the trial commenced, others have reported similar difficulty in predicting unscheduled healthcare among those with asthma.20
The study was powered to demonstrate equivalence within ±5% assuming 6% needing unscheduled healthcare. This figure was chosen based on national statistics on unscheduled use of health services current at the time the study was designed. With 30% requiring unscheduled healthcare, the observed 95% CI for the difference between the arms18 (−9.5% to 8.0%) would not have demonstrated equivalence within ±7.5% but it would have demonstrated equivalence within ±10%, had those limits been chosen to be clinically acceptable from the outset. While statistical equivalence was not demonstrated, the clinical outcomes following education delivered by lay people and nurses are almost identical suggesting that lay educators can produce similar outcomes to those achieved by primary care practice based nurses. Furthermore, patients found this to be an acceptable approach. These are encouraging findings, suggesting that this approach merits further attention.
Using lay educators to deliver healthcare involves consideration of a number of logistical issues. In this study, we recruited lay educators from prior knowledge or open advertisement who were fully appraised of the task ahead, but nevertheless several dropped out of the study shortly after training. This in part reflected a delay between training and use of that training, which resulted from difficulties in obtaining approval and honorary contracts from some Primary Care Trusts. In discussion, it also appears likely that some of the lay educators responded to the advertisement to learn more about asthma for themselves or their family and were less committed to the idea of delivering education to others. Our lay educators’ reflections on this process have been reported elsewhere.21 The fact that we did not contractually employ the educators meant that we had no “control” over them. Their training course was a “one-off” course designed especially for this research meaning that it was impossible to recruit additional educators and send them for training during the course of the research, as might have been possible in a real life situation. However, equal problems were encountered with nurse delivered education. We had anticipated that many primary care based nurses in West London and the North West of England would have already been in possession of an Asthma Training Diploma or Certificate, but in the event this was the case for only one nurse, hence our previously planned 1 day training update had to be made more basic and further training sessions arranged for interested nurses. The high turnover of nurses in primary care was also unexpected and it was difficult for nurses to maintain ongoing commitment to the provision of asthma education because of competing priorities, such as seasonal vaccinations. The logistical lessons learnt from this trial will be of value to others seeking to undertake comparable work.
In conclusion, Cochrane Systematic Reviews and National Guideline recommendations promote self-management education for those with asthma. The evidence suggests that this aspect of the guidelines is poorly implemented. We have demonstrated that such education can be given by well trained lay persons, with outcomes comparable with those achieved by practice nurses.
Acknowledgments
We acknowledge with thanks the provision of patient information materials by Asthma UK.
MRP and A-LC jointly wrote the proposal for the study, recruited the practices and supervised its undertaking. CB and JH recruited the patients and acted as the link with the lay educators, nurses and practices. MRP, A-LC, CB, JH and MC analysed the results. MRP wrote the first draft of the paper, but all authors contributed and agreed to the final version.
REFERENCES
Footnotes
▸ The appendix is published online only at http://thorax.bmj.com/content/vol63/issue9
MR Partridge and A-L Caress contributed equally to the project.
Funding: This study was funded by the BUPA Foundation.
Competing interests: None.
Ethics approval: Ethics approval was obtained.
Linked Articles
- Airwaves