Article Text

Abstract
Little is known about when symptoms of idiopathic pulmonary fibrosis first develop. We identified incident cases of idiopathic pulmonary fibrosis-clinical syndrome (IPF-CS) from a UK primary care database and assessed the frequency of consultations for common symptoms in the 5 years prior to diagnosis. 1671 cases were identified with 5 years of data prior to diagnosis. Breathlessness was the most common symptom, followed by cough. Cases were significantly more likely than controls to experience these symptoms (p<0.001), even 4–5 years before diagnosis (OR for breathlessness for this period 2.79, 95% CI 2.13 to 3.65). This suggests that some patients with IPF may be symptomatic for more than 5 years before diagnosis.
- idiopathic pulmonary fibrosis
- clinical epidemiology
Statistics from Altmetric.com
Introduction
Idiopathic pulmonary fibrosis (IPF) is a progressive disease with a median survival of 2–3 years following diagnosis.1 Diagnosis is often delayed,2 3 with evidence that a delay in referral to specialist care can impact on survival.4 Retrospective studies of symptom duration prior to diagnosis are limited by small populations and recall bias and do not reflect primary care consulting behaviour prior to diagnosis. With the introduction of antifibrotic therapies, there have been calls for earlier diagnosis5 to help define the natural history of the disease, allow more patients to enrol in clinical trials and potentially allow earlier treatment. We sought to investigate the presence of key symptoms in the years prior to a diagnosis of IPF, using primary care data from the UK.
Methods
We conducted a matched case–control study using The Health Improvement Network (THIN), an anonymised longitudinal primary care database that includes all consultations, prescriptions and diagnoses from a patient’s health record. THIN covers around 500 general practices, with over 12 million patients (3.6 million current patients),6 and is representative of the UK population. Incident cases were identified based on Read codes previously used to identify IPF,7 with a year of data prior to the first record to exclude prevalent cases. These cases were labelled IPF-clinical syndrome (IPF-CS), acknowledging some might not be ‘true’ IPF due to miscoding. Controls were identified as a 4:1 incidence density sample, matched on age, sex and primary care practice, meaning each case could have up to four possible controls.
Exclusions included cases with imprecise diagnosis dates, patients under 40, those with coexisting records suggesting alternative causes of pulmonary fibrosis (eg, rheumatoid arthritis; see online supplementary file 1) and those with prescriptions for amiodarone and methotrexate in the year prior to diagnosis.
Supplementary file 1
Consultations for breathlessness, cough, fatigue and weight loss were identified for cases and controls, as well as consultations for chronic obstructive pulmonary disease (COPD) or heart failure, as markers of potential misdiagnoses. Read codes identifying these are available on request.
The presence of a consultation for each symptom was identified in each 1-year time period up to 5 years before the date of diagnosis and compared between cases and controls by conditional logistic regression, with adjustment for smoking status. Consultations were plotted on a histogram for both cases and a single randomly selected control to enable graphical comparison of consulting behaviour. Sensitivity analyses were carried out focusing on those who had never smoked only and those without any record of COPD or heart failure.
Statistical analysis was performed using Stata V.14.0.
Results
We identified 2062 incident cases of IPF-CS, with 7187 controls. One thousand six hundred and seventy-one cases had 5 years of data prior to diagnosis. Sixty-three per cent were male, with a mean age at diagnosis of 74 years (SD 9.7 years). Cases were more likely to be ex-smokers than controls.
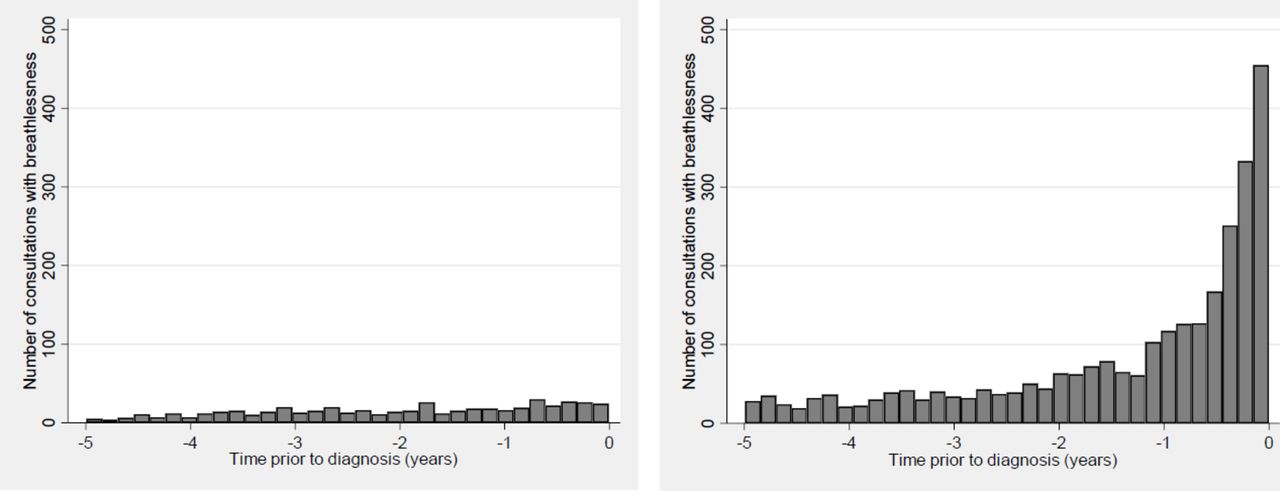
Forty-three per cent of cases had a consultation for breathlessness in the year prior to diagnosis, compared with 7% of controls (table 1). There was a rise in consulting behaviour for this symptom over the year (figure 1). Thirty-two per cent of cases had at least one consultation for cough in the preceding year (see table e2 in the online supplementary file 1); this symptom became more common at an earlier stage (see online figure e2 in the supplementary file 1). There was a significantly increased chance of cases having a consultation for these symptoms in each of the 5 years prior to diagnosis: even 4–5 years prior to diagnosis, cases were almost three times more likely to present with breathlessness than controls (OR 2.79; 95% CI 2.13 to 3.65, p<0.001), and cases were almost twice as likely to present with cough (OR 1.78; 95% CI 1.47 to 2.17, p<0.001). Fatigue and weight loss were also more common in cases compared with controls.

{kind=link}
Number of consultations for breathlessness for idiopathic pulmonary fibrosis cases (right panel) and single-matched controls (left panel) over 5 years prior to diagnosis date.
Number of idiopathic pulmonary fibrosis cases and controls with consultations for breathlessness (SOB) within five 1-year periods prior to diagnosis date
Cases were significantly more likely to have a diagnosis of heart failure in each of the 5 years prior to diagnosis, and a diagnosis of COPD in each of the 4 years prior to diagnosis (see tables e3 and e4 in the online supplementary file 1). The number of diagnoses of heart failure and COPD increased notably in the year prior to diagnosis (see figures e3 and e4 in the online supplementary file 1). In our sensitivity analysis including only those who had never smoked, breathlessness and cough were still significantly more common in cases than controls in all time periods; if all patients with a diagnosis of heart failure or COPD were excluded, breathlessness and cough again remained more common in cases (see online supplementary file 1).
Discussion
Cases with IPF-CS were significantly more likely than controls to present to their primary care practitioner with a symptom of breathlessness or cough in the 5 years preceding diagnosis, with a less dramatic association for fatigue and weight loss. Cases also had more diagnoses of heart failure or COPD prior to diagnosis of IPF-CS, particularly in the preceding year.
It is not clear whether these symptoms represent subclinical early interstitial lung disease or alternative respiratory complaints, but there may be the opportunity to diagnose IPF earlier. The increase in recorded diagnoses of heart failure and COPD could either reflect coexistent diagnoses given that smoking and heart disease are both more common in IPF8 9 or misdiagnoses of common conditions with similar symptoms.
Strengths of this work include the prospective data collection, preventing the recall or observer bias inherent in standard case–control studies. Limitations include the validity of primary care records for IPF-CS and the possibility of delayed presentation even to primary care.
Earlier diagnosis of IPF may lead to earlier treatment and potentially extended survival, although there is currently no consensus on whether earlier treatment will be beneficial (or cost-effective). Earlier diagnosis may also reduce unnecessary investigations into worsening dyspnoea. Increased use of chest radiography in primary care for patients with breathlessness and cough—as per National Institute for Health and Care Excellence guidelines10—may help identify IPF or other common conditions such as COPD and heart failure sooner.
Footnotes
Competing interests RBH and TMM have received grants from GSK for the PROFILE study, which aims to examine longitudinal disease behaviour and potential biomarkers in IPF. JPH has received funding from GSK for delivering a teaching session on asthma, and from Actelion to attend a two-day preceptorship on pulmonary hypertension. TH, JEG and VN have no competing interests.
Ethics approval THIN Scientific Review Committee (SRC 14–047).
Provenance and peer review Not commissioned; externally peer reviewed.