Article Text

Abstract
Familial pulmonary fibrosis is associated with loss-of-function mutations in telomerase reverse transcriptase (TERT) and short telomeres. Interstitial lung diseases have become the leading indication for lung transplantation in the USA, and recent data indicate that pathogenic mutations in telomerase may cause unfavourable outcomes following lung transplantation. Although a rare occurrence, solid organ transplant recipients who develop acute graft-versus-host disease (GVHD) have very poor survival. This case report describes the detection of a novel mutation in TERT in a patient who had lung transplantation for familial pulmonary fibrosis and died from complications of acute GVHD.
- idiopathic pulmonary fibrosis
- airway epithelium
Statistics from Altmetric.com
Case-based discussion
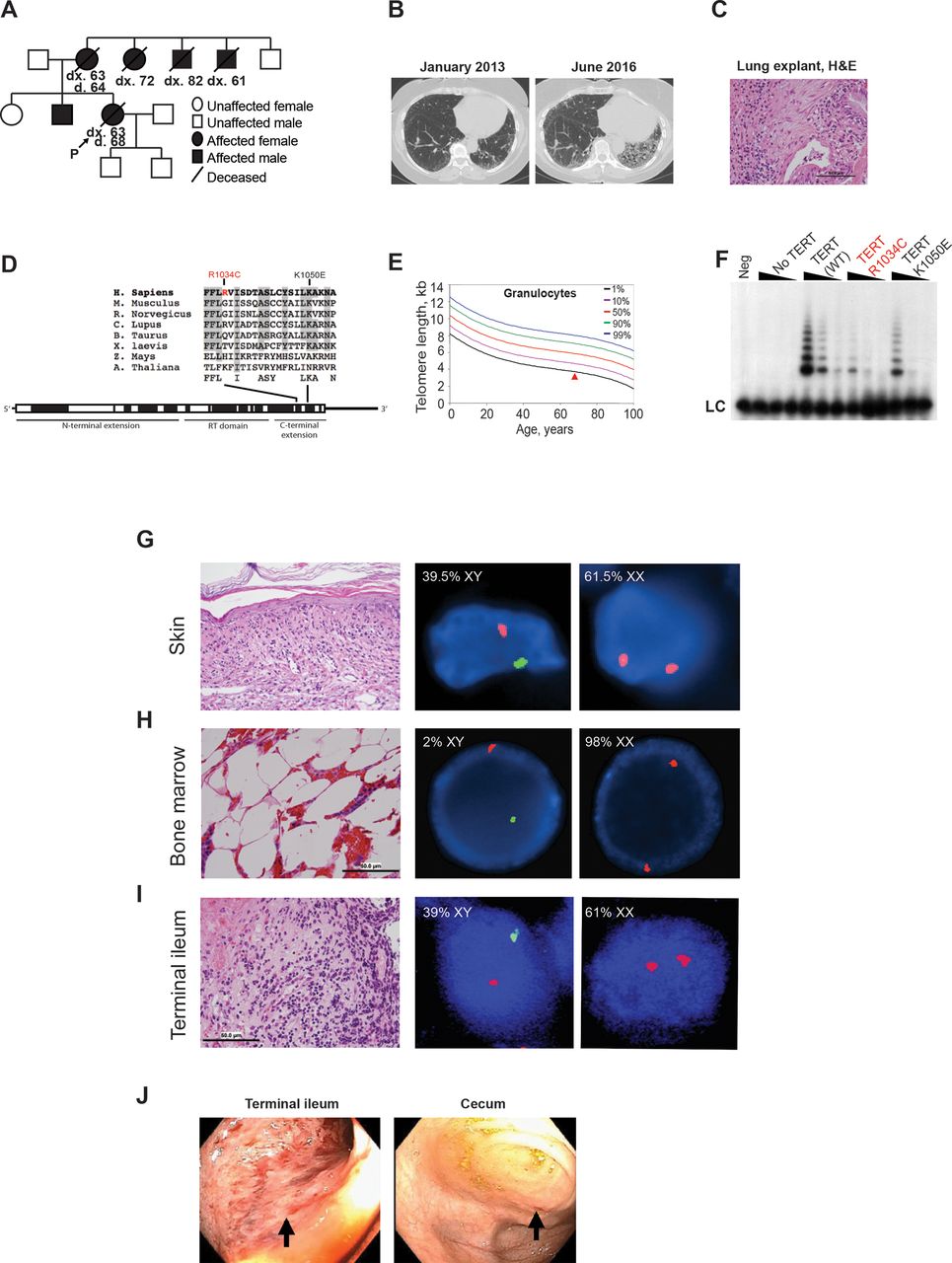
A woman who had familial pulmonary fibrosis (figure 1A) presented to our transplant programme for evaluation. Her symptoms began 5 years prior with a chronic non-productive cough and dyspnoea. Spirometry showed a mild restrictive ventilatory abnormality, and chest CT showed typical characteristics of pulmonary fibrosis (figure 1B). Despite experimental treatment with a lysophosphatidic acid receptor blocker and pirfenidone, her symptoms, physiological abnormalities and radiological findings progressively worsened with a nadir FVC of 1.46 L (50% of predicted), total lung capacity of 2.09 L (41%) and diffusing capacity of the lungs for carbon monoxide of 3.7 mL/min/mm Hg (22%). Histopathological analysis of the explanted native lungs showed end-stage lung disease and extensive interstitial fibrosis and honeycombing (figure 1C).
{kind=link}
Acute graft-versus-host disease following lung transplantation in a patient with familial pulmonary fibrosis harbouring a novel TERT mutation. (A) Pedigree of the proband (P) and the TERT R1034C mutation shows extensive family history of pulmonary fibrosis. (B) Serial CT of the chest (axial view) of the lower lobes of the lung shows progression of interstitial lung disease, especially at the left base (reader’s right side). (C) Histopathology by H&E stain of formalin-fixed paraffin-embedded lung explant tissue obtained from the proband at the time of lung transplantation. 500X magnification (50 µm scale bar). (D) Location and conservation analysis of TERT amino acid residues altered in the proband (R1034C) and control mutation (K1050E). Amino acid sequences were aligned using ClustalW. Conserved residues identified as the consensus region are shaded. (E) Telomere length in granulocytes measured by flow cytometry coupled to in situ hybridisation with a telomere-specific probe, plotted by age. Established age-adjusted reference percentiles are indicated by lines. Red triangle identifies the proband. (F) Telomerase activity by telomere repeat amplification protocol (TRAP) in cells that express wild-type TERT and mutant forms of TERT R1034C and K1050E. Neg control: NP40 buffer. (G–I) Histopathology by H&E stain and fluorescence in situ hybridisation (FISH) of the X and Y chromosomes of the (G) skin at 200X magnification showing vacuolar alteration of the dermoepidermal junction associated with scattered necrotic keratinocytes and a sparse lymphocytic infiltrate, (H) bone marrow at 500X magnification showing hypocellular marrow with maturing multilineage haematopoiesis with erythroid predominance, and (I) terminal ileum at 500X magnification showing ulcerated granulation tissue with intraepithelial apoptosis. Representative images of FISH to centromeres of the X (CEPX, red) and Y (CEPY, green) chromosomes, identifying donor (XY) and recipient (XX) cells are shown (50 µm scale bar). (J) Colonoscopy images of the terminal ileum and caecum. Black arrows point to ulcerations and granulation tissue in the terminal ileum and erosion in the caecum. d, age at death; dx, age at diagnosis with pulmonary fibrosis; LC, loading control; Neg, negative; RT, reverse transcriptase; TERT, telomerase reverse transcriptase; WT, wild type.
Given this patient’s family history of interstitial lung disease, we recommended sequencing studies to assess mutations in 14 different telomere biology-related genes. Using next-generation sequencing (NGS) we identified a novel, non-synonymous mutation in telomerase reverse transcriptase (TERT), c.3100C>T, p.R1034C, that resulted in an amino acid substitution at a weakly conserved site (figure 1D). The allelic frequency of this mutation in the ExAC database was 0.000008384 (1 in 120 000). The in silico pathogenicity prediction tools SIFT, PolyPhen2, Align GVGD and REVEL provided contradictory results suggesting the mutation may or may not have deleterious effects on TERT, and prior studies have not described this variant. Therefore, we classified the mutation as a variant of unknown significance. However, her granulocyte telomere length measured by flow-fluorescent in situ hybridisation (FISH) was below the first percentile for her age (figure 1E). Given this discrepancy between NGS and flow-FISH, we undertook further experimental studies to evaluate the functional impact of this mutation. We employed U2OS cells that lack endogenous telomerase and ectopically expressed the telomerase components telomerase RNA component (TERC) and either wild-type or mutant TERT. Importantly, expression levels of both TERC and different forms of TERT were similar in all cell lines analysed (data not shown). Using telomere repeat amplification protocol assays to assess telomerase activity, we found that TERT 3100C>T (R1034C) caused a marked reduction in telomerase activity by more than 75% compared with wild-type TERT (figure 1F). Additionally, this variant had a more deleterious effect on telomerase activity than TERT 3148A>G (K1050E), another variant in the c-terminal domain previously linked to pulmonary fibrosis (figure 1D,F).1 These results demonstrated that the TERT 3100C>T variant severely compromised telomerase activity by approximately 75% in human cells, supporting the pathogenicity of this mutation.
In October 2016, the patient had a bilateral lung transplant from a male donor. The donor-recipient pair had bidirectional mismatches at human leucocyte antigens (HLA)-A, B, C, DRB1 and DQB1. Serological crossmatch was negative. Both the recipient and the donor were cytomegalovirus (CMV) seropositive. The lung transplant recipient received induction therapy with basiliximab on the day of transplantation and 4 days later. Her maintenance immunosuppressive regimen consisted of tacrolimus, mycophenolate and prednisone. Her infection prophylaxis regimen included acyclovir (later changed to valganciclovir), trimethoprim-sulfamethoxazole and nystatin. She had a relatively uncomplicated immediate postoperative course and was discharged 9 days after surgery. However, 3 weeks later she developed a diffuse non-pruritic mottled rash on her chest and face that progressed to involve her back, extremities, palmar surfaces and oral mucosa. Initially, the rash was attributed to a drug reaction, and because of leukopenia valganciclovir was discontinued and mycophenolate was reduced and then eventually discontinued. She did not improve with these changes and her clinical condition continued to worsen with the development of watery diarrhoea, nausea, cough, gingival bleeding, chills and fever. When hospitalised for further evaluation, she was also found to have pancytopenia with 0.9x109/L white blood cells/μL, 9.5 g/dL haemoglobin and 52x109/L platelets. She received empirical antimicrobial therapy including cefepime, vancomycin, metronidazole, micafungin and acyclovir.
Despite these changes in her medications, the patient continued to have progressive multiorgan dysfunction. Therefore, the transplant team considered acute graft-versus-host disease (GVHD) as a possible diagnosis and evaluated her dysfunctional organs. Skin biopsy showed interface dermatitis, with short tandem repeat (STR) identity testing revealing mixed chimerism with 12% of the DNA derived from the donor. FISH of the X and Y chromosomes (XY-FISH) showed 39.5% donor-derived cells in the skin (figure 1G). Bone marrow core biopsy revealed a markedly hypocellular marrow, and bone marrow aspirate XY-FISH showed 2% donor-derived cells (figure 1H). Peripheral blood STR identity testing of CD3-enriched T cells demonstrated 42% donor origin, whereas CD15-enriched granulocytes were 100% recipient derived. Endoscopic biopsy of the terminal ileum showed extensive lymphocytic inflammation with ulcerations and granulation tissue, and XY-FISH showed 39% of cells derived from the donor (figure 1I). Gross findings on colonoscopy showed complete loss of villi, erythema and granular appearance of the terminal ileum and an erosion in the caecum (figure 1J). Thus, the patient developed acute GVHD that became symptomatic about 1 month after lung transplant.
The patient also had low-grade CMV viraemia upon readmission with blood CMV DNA levels of 1350–1450 IU/mL and CMV-positive cells detected in terminal ileum and stomach biopsies, though biopsies from the duodenum, ascending colon and descending colon were CMV negative. She received ganciclovir and then foscarnet for the CMV infection, with low blood CMV DNA levels ranging from <870 to 9920 IU/mL. She did not show evidence of hepatitis.
In the setting of early post-transplant GVHD, she continued tacrolimus, had mycophenolate reinitiated and had her steroid dose markedly increased. She also received thymoglobulin and intravenous immunoglobulin and initiated extracorporeal photopheresis. For her pancytopenia she received filgrastim, eltrombopag, and red blood cell and platelet transfusions. Bone marrow transplant evaluation was also initiated. However, she developed a bowel perforation and septic shock, and based on patient and family wishes, she received comfort care only and died a few days later.
Discussion
This case report describes the discovery of a novel loss-of-function mutation in the telomerase gene TERT 3100C>T in a patient with familial pulmonary fibrosis who developed acute GVHD involving the bone marrow, skin and gastrointestinal tract about 1 month after lung transplantation. Telomeres support genomic integrity, especially in rapidly dividing cells such as the respiratory epithelium and immune cells.2 Recent evidence suggests that patients who have familial pulmonary fibrosis and a pathogenic telomerase mutation have unfavourable outcomes following lung transplantation that include thrombocytopenia, leucopenia and poor tolerance of immunosuppressive agents.3
Normally, a transplant recipient’s immune system recognises foreign cells in the solid organ allograft, mounts an immune response and eliminates donor-derived immune cells. Rarely, this immunosurveillance programme fails in solid-organ transplant recipients, leading to donor immune cell engraftment and the development of acute GVHD.4 This rare complication results in death within 1–2 months of onset in most cases.5 The factors that contribute to acute GVHD are not well understood, although this patient had bidirectional donor-recipient HLA class I and II mismatches which may support immune surveillance of the lung allograft. Abnormally low telomerase activity is associated with impaired immunosurveillance and defective cell-mediated immunity,6 and this report suggests that loss-of-function mutations in telomerase may reduce the ability to effectively eliminate donor immune cells in lung grafts.
We hypothesise that the loss-of-function mutation in the telomerase gene TERT 3100C>T and the associated impaired telomerase activity led to defective cell-mediated immunity and T cell exhaustion7 and contributed to the patient’s susceptibility for developing acute GVHD. Even though the donor lung allografts likely transferred a low number of T cells to the recipient, the recipient’s exhausted or depleted T cells may have left an immunological niche filled by donor T cells undergoing homeostatic proliferation to replete the overall T cell pool.8 In addition, the donor’s T cells may have had a competitive advantage over the recipient’s T cells with defective telomerase, and this may have supported engraftment and subsequent acute GVHD. Though the patient did not exhibit evidence of bone marrow failure prior to lung transplantation, her immune cells with defective telomerase may have been more susceptible to immunosuppressive medications than donor-derived cells. Once engrafted, donor T cells were likely stimulated with recipient-specific (eg, mismatched HLA) and/or pathogen-specific (eg, CMV) antigens to promote donor T cell proliferation and GVHD.
While recipient telomerase deficiency seems unlikely or is unknown to contribute to most reported cases of acute GVHD following lung transplantation,9 the present study suggests that telomerase mutations could potentially contribute in some cases. Future studies should further assess the relationship between telomerase mutations and the risk of developing acute GVHD, bone marrow failure, and related complications after lung transplantation, and how related changes in patient management will affect patient outcomes.
Acknowledgments
The authors thank the family of the patient for their kind support. We dedicate this project in memory of the patient, with the hope that continued research will improve or extend the lives of others.
Footnotes
JRB and ATV contributed equally.
Contributors JRB, ATV and KAB performed experiments. JRB, ATV, RDY and LFZB wrote the manuscript. All other authors were involved in the clinical management of the patient. Correspondence should be addressed to RDY and LFZB.
Funding JRB is supported by the Physician Scientist Training Program at the Washington University School of Medicine and funds from the Department of Pathology and Immunology, Washington University School of Medicine. ATV is supported by the Philip W Majerus Fellowship Award from the Division of Hematology, Washington University School of Medicine. KAB is supported by the National Fellowship Foundation. CL is supported by the Washington University Hematology Scholars K12 award (K12-HL087107-07). LFZB is supported by the NHLBI (4R00HL114732-03 and 1R01HL137793-01) and grants from the Department of Defense (BM160054), the V Foundation for Cancer Research, the Edward Mallinckrodt Jr Foundation, the American Federation for Aging Research, the Longer Life Foundation and the Center for Regenerative Medicine at Washington University.
Competing interests None declared.
Ethics approval Washington University Human Research Protection Office (HRPO).
Provenance and peer review Not commissioned; externally peer reviewed.